
Abstract
This study evaluated the efficacy of umbilical cord blood (UCB) cell for patients with cerebral palsy (CP) in a randomized, placebo-controlled, double-blind trial and also assessed factors and mechanisms related to the efficacy. Thirty-six children (ages 6 months to 20 years old) with CP were enrolled and treated with UCB or a placebo. Muscle strength and gross motor function were evaluated at baseline and 1, 3, and 6 months after treatment. Along with function measurements, each subject underwent 18F-fluorodeoxyglucose positron emission tomography at baseline and 2 weeks after treatment. Cytokine and receptor levels were quantitated in serial blood samples. The UCB group showed greater improvements in muscle strength than the controls at 1 (0.94 vs. −0.35, respectively) and 3 months (2.71 vs. 0.65) after treatment (Ps<0.05). The UCB group also showed greater improvements in gross motor performance than the control group at 6 months (8.54 vs. 2.60) after treatment (P<0.01). Additionally, positron emission tomography scans revealed decreased periventricular inflammation in patients administered UCB, compared with those treated with a placebo. Correlating with enhanced gross motor function, elevations in plasma pentraxin 3 and interleukin-8 levels were observed for up to 12 days after treatment in the UCB group. Meanwhile, increases in blood cells expressing Toll-like receptor 4 were noted at 1 day after treatment in the UCB group, and they were correlated with increased muscle strength at 3 months post-treatment. In this trial, treatment with UCB alone improved motor outcomes and induced systemic immune reactions and anti-inflammatory changes in the brain. Generally, motor outcomes were positively correlated with the number of UCB cells administered: a higher number of cells resulted in better outcomes. Nevertheless, future trials are needed to confirm the long-term efficacy of UCB therapy, as the follow-up duration of the present trial was short.
Introduction
U
Designed as a double-blind randomized controlled trial, the present study aimed to outline the efficacy and safety of allogeneic UCB cell therapy in children with CP. 18F-fluorodeoxyglucose positron emission tomography (18F-FDG-PET) was utilized to evaluate the effects of UCB on the brain, particularly in terms of inflammatory status. While our previous study showed reduced inflammation in periventricular white matter following coadministration of UCB and EPO [4], no studies to date have investigated the effects of UCB treatment alone on the inflammatory status of the brain. Additionally, we also analyzed cytokine levels and blood cell components to assess the effects of this therapy on inflammatory responses in relation to motor outcomes. In a preliminary study, which was conducted to screen for the effects of UCB therapy on inflammation, pentraxin 3 (PTX3) emerged as an acute reactant (Supplementary Fig. S1; Supplementary Data are available online at
Methods
Participants
Patients diagnosed with CP of ages 6 months to 20 years were eligible for inclusion in this study. The exclusion criteria were as follows: medical instability due to pneumonia or renal dysfunction at enrollment; known or suspected genetic syndrome; allergy to concomitant medications; clinically uncontrolled epilepsy; and lack of family support. From February 2012 to July 2012, 41 patients were screened at CHA Bundang Medical Center. Excluding five, a total of 36 patients were finally enrolled. Power analysis to determine the sample size was not conducted due to the limited number of participating subjects. Patients or their legal representatives provided written informed consent before conducting any study-related procedures.
Study design and masking
This study was designed as a placebo-controlled, double-blind study and conducted in accordance with the Declaration of Helsinki. An independent statistician produced a randomization table for patient grouping using SAS software. Subjects were randomly assigned (1:1) into the UCB or control group in accordance with this randomization table.
To maintain study blinding, participants from both groups were moved to the treatment room after being sedated in accordance with the sedation protocol for children. Each study subject remained in this room for a similar length of time. All UCB infusions were conducted by two independent physicians apart from the clinical study team. Control subjects received placebo materials in place of the concomitant medications (cyclosporine and solumedrol) administered to the UCB group. Investigators, assessors, participants, and their parents were all blinded to the group allocation until the study was completed. This study was approved by the Institutional Review Board and Ethics Committee of CHA Bundang Medical Center and was registered at
The initial study duration was 3 months after treatment. Additionally, outcome scores at 6 months after treatment, which were measured during routine follow-up, were used to determine the efficacy of UCB therapy on motor outcomes over this longer period of time.
UCB preparation and delivery
Cord blood units with ≤2 human leukocyte antigen (HLA) disparities among HLA-A, B, and DRB1 at high resolution and with ≥2×107 total nucleated cells (TNCs)/kg were selected. If a single UCB unit did not satisfy these criteria, multiple units were used. The UCB units were thawed and washed before UCB infusion via intravenous or intra-arterial routes. Intra-arterial cell administration under transfemoral cerebral angiography was preferred for cord blood units with TNC <6×107/kg in patients who were older than 4 years.
Concomitant medications
Twelve hours before UCB administration, cyclosporine (2.0 mg/kg) mixed with normal saline was infused twice intravenously. Cyclosporine was then administered intravenously at 1–2 mg/kg, twice daily, for 3 days after UCB administration. Oral cyclosporine was administered for an additional 9 days thereafter. The target plasma cyclosporine range was 100–200 ng/mL. One intravenous injection of solumedrol (3 mg/kg) was given 1 h before UCB administration.
Functional assessments
Manual muscle testing (MMT) score was calculated as the sum of test results for 40 muscle groups: flexor and extensor of the neck; flexor and extensor of the trunk; flexors, extensors, abductors, adductors, and internal and external rotators of the bilateral shoulder and hip joints; flexors and extensors of the bilateral knee; and dorsiflexors and plantar flexors of the bilateral ankles. Muscle strength was converted into scores of zero, 0; trace, 1; poor, 2; fair, 3; good, 4; and 5; normal. Thus, total MMT scores ranged from 0 to 200 [15].
Gross Motor Function Measure (GMFM) and Gross Motor Performance Measure (GMPM) were utilized to assess gross motor control ability; the reliabilities of these examinations at the study facility have been reported previously [16]. Raw scores for the Bayley Scales of Infant Development, second edition (BSID-II), were also used to assess neurodevelopmental progress, the reliabilities of which have also been previously described [17]. According to the authors of BSID-II, the scale is applicable in individuals of developmental ages <42 months, although they may in actuality be older [18]. The Functional Independence Measure for Children (WeeFIM®) [19] and the Pediatric Evaluation of Disability Inventory (PEDI) [20] were also used. The MMT, GMFM, GMPM, BSID-II, WeeFIM, and PEDI were assessed at baseline and 1, 3, and 6 months post-treatment.
18F-FDG-PET image acquisition
Brain 18F-FDG PET images were acquired at baseline and at 2 weeks after UCB administration in all participants using a Gemini PET/CT scanner (Phillips). Before injection of the radiotracer, a transmission computed tomography (CT) scan was performed to generate attenuation maps. Approximately 50 min after the intravenous administration of 370 MBq of 18F-FDG, 90 brain-emission images were obtained over a period of 20 min. A board-certified nuclear physician reviewed the 18F-FDG-PET/CT scans. After excluding data from participants who had severe encephalopathy or structural cortical damage, PET images from 30 subjects were analyzed (15 from the UCB group and 15 controls) after image reconstruction using the row action maximum likelihood algorithm. Spatial, preprocessing, and statistical analyses were performed using SPM8 within Matlab R2011a (Mathworks) to compare differences in regional brain glucose metabolism between the two groups and between pre- and post-treatment images. The 18F-FDG PET images were converted from DICOM to the ANALYZE format using MRIcro software (
Cytokine analyses
Blood samples were collected in ethylenediaminetetraaceticacid (EDTA) Vacutainer® tubes at baseline, 1 day before UCB administration, and 1 day, 12, and 90 days after treatment. Samples were preserved at −80°C in a freezer, after separating the plasma and buffy coats via centrifugation at 2,000 g for 20 min. Plasma levels of PTX3, interleukin (IL)-8, and IL-10 were measured using enzyme-linked immunosorbent assay (ELISA) test kits purchased from R&D Systems, in accordance with the manufacturer's instructions. Briefly, EDTA plasma samples were diluted with reagent diluent at 23% (v/v) for PTX3 and at 50% (v/v) for IL-8 and IL-10. The samples were then incubated in 96-well plates, and targeted proteins were detected by biotinylated antibodies, followed by streptavidin-horseradish peroxidase. The signals were visualized by the addition of 100 μL of 3,3′,5,5′-tetramethylbenzidine for 30 min, followed by 50 μL of the stop solution. Each sample procedure was repeated twice. Cytokine levels are presented as ng/mL.
Receptor analyses
Serum levels of toll-like receptor (TLR)4, TLR2, and mammalian target of rapamycin (mTOR) were also measured in plasma-free buffy coat samples from selected participants within each study group who showed similar brain lesions, clinical features, ages, and severity of gross motor impairment. Buffy coat samples were diluted in phosphate-buffered saline (PBS) at 20% (v/v), with 1% (v/v) protease inhibitor cocktail (Thermo Scientific) and 1% (v/v) Triton-X100, to lyse the red and white blood cells. These samples were then diluted to 5% (v/v) with PBS before analysis of TLR4, TLR2, and mTOR using ELISA test kits purchased from Elabscience, following the manufacturer's protocols.
Bradford assays were performed using the manufacturer's protocol (Bradford Protein Assay Kit No. 23200; Thermo) to measure total protein levels in the blood samples. Total protein levels were used to normalize blood receptor level data. The average protein level was calculated for each patient, and the ratio of sample total protein level/average total protein level was used to normalize TLR4, TLR2, and mTOR levels. The levels of these receptors are presented as ng/mL.
Statistical analyses
Statistical analyses were performed using Prism software, version 5.0 (Graphpad Software), and Statistical Package for the Social Sciences software, version 21.0 (IBM;
Results
Thirty-six children with CP participated in the study, and 34 subjects completed all of the testing procedures (Supplementary Fig. S2). The general baseline characteristics of the UCB and control groups were not significantly different (Table 1). Also, no serious adverse events occurred during this study (Supplementary Table S1).
Values represent number of patients unless otherwise noted. No baseline characteristics were significantly different between the two groups (P-value>0.05 for all comparisons).
UCB group received umbilical cord blood and rehabilitation.
Control group received rehabilitation only.
Age corrected for preterm birth.
NBW was defined as birth body weight≥2,500 g, LBW <2,500 g, VLBW <1,500 g, and ELBW <1,000 g.
UCB, umbilical cord blood; NBW, normal birth weight; LBW, low birth weight; VLBW, very low birth weight; ELBW, extremely low birth weight; GMFCS, Gross Motor Function Classification System; SD, standard deviation; MRI, magnetic resonance imaging.
Effects of UCB on motor outcomes
Improvements in functional measures
No significant difference in baseline functional scores was discovered between the UCB and control groups (Supplementary Tables S2 and S3). The UCB group showed significantly greater improvements in MMT from baseline to 1 and 3 months post-treatment than the control group (Ps<0.05); GMPM scores also significantly improved in the UCB group from baseline to 6 months post-treatment (P<0.01) (Fig. 1; Supplementary Table S2). Analyses of the data after excluding subjects who received intra-arterial administration resulted in similar findings (Supplementary Fig. S3).

Comparison of functional outcomes between UCB and control groups. Changes in
Effects of HLA compatibility on functional measures in the UCB group
In the UCB group, changes in functional outcome scores were compared in relation to HLA disparity. Compared with the two-HLA mismatched subgroup, the fully HLA-matched and 1-mismatched subgroups showed greater increases in MMT, BSID-II motor scale, and WeeFIM scores. Notwithstanding, the fully HLA matched and 1-mismatched subgroups did show higher baseline scores thereof, compared with the two-HLA mismatched subgroup (Supplementary Table S4).
Effects of TNC number on functional measures in the UCB group
The median number of TNC/kg was 5.46×107. To analyze the effect of cell number on improvements in functional measures, subjects from the UCB group were divided according to the median number of TNC/kg. Differences in functional measure scores between the subgroups at baseline were not statistically significant. Participants who received more than the median number of TNC/kg showed greater improvements in BSID-II motor raw score than those who did not (Supplementary Fig. S4A). Additionally, we noted a significant positive correlation between BSID-II motor scale scores at 3 months and the number of TNC administered (r=0.54, P<0.05) (Supplementary Fig. S4B). TNC counts, route of UCB administration, body weight, and HLA disparity for each subject in the UCB group are listed in Table 2.
TNC, total nucleated cell; HLA, human leukocyte antigen.
Effects of UCB on brain 18F-FDG-PET images
Baseline scans of the UCB and control subjects showed no marked differences. Two weeks after UCB administration, subjects in the UCB group showed a prominent decrease in activity in bilateral white matter of the occipital and temporal lobes, whereas increased activity was observed in multiple cortical areas of the frontal and parietal lobes (Fig. 2A; Supplementary Tables S5 and S6). Subjects in the control group showed decreased activity in multiple areas of the cerebrum and increased activation of limited areas of the frontal and parietal cortices (Fig. 2B; Supplementary Tables S7 and S8).
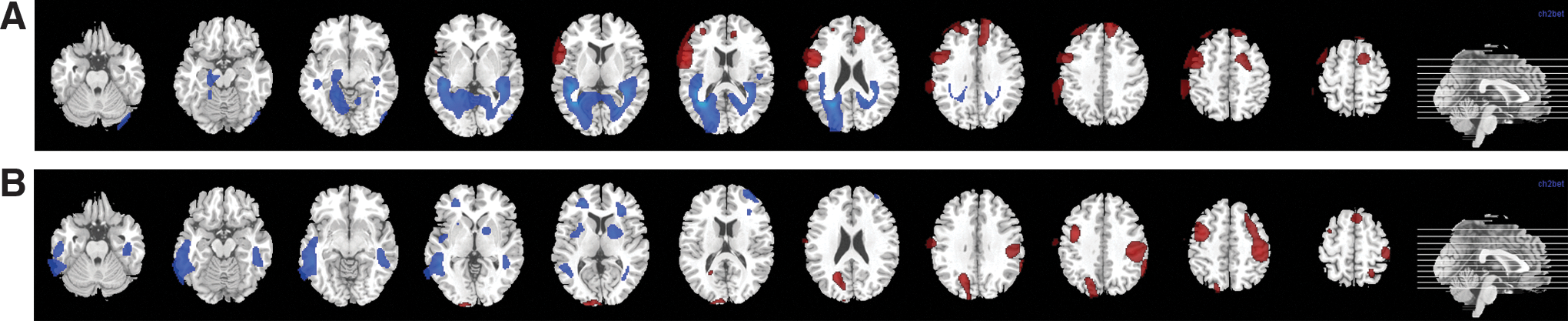
Changes in 18F-FDG PET/computed tomography glucose metabolism during the period between baseline and 2 weeks post-treatment. Areas in red denote increased glucose metabolism and blue highlights decreased glucose metabolism in the
Relationships between motor outcomes and inflammatory markers
Plasma PTX3, IL-8, and IL-10 levels and functional measures
Baseline levels of PTX3 and IL-8 at 1 day before administration of UCB or placebo were similar between the two study groups.
One day after administration of UCB, plasma levels of PTX3 increased significantly by 4.07±0.50 ng/mL, compared with the control group (−0.05±0.45) (P<0.001). By 12 days post-treatment, PTX3 levels had decreased slightly, although levels for the UCB group remained significantly higher than those observed in the control group (P<0.01). At 90 days after treatment, PTX3 levels were similar between the UCB and control groups (Fig. 3A; Supplementary Table S9). Interestingly, among UCB group subjects, those who showed higher levels of PTX3 at 1 day after treatment demonstrated greater improvements in their GMPM scores at 1 and 3 months post-treatment (Supplementary Fig. S5).
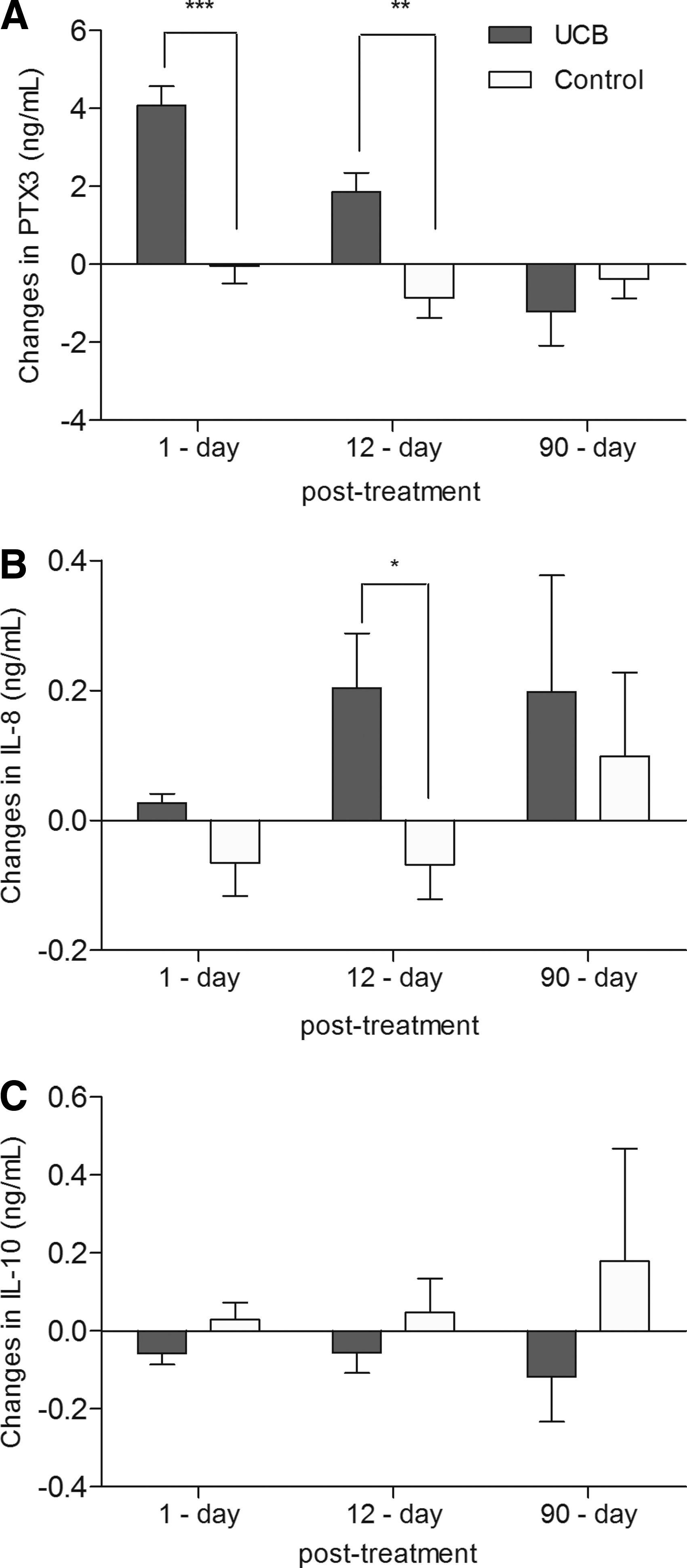
Comparison of changes in PTX3, IL-8, and IL-10 levels between UCB and control groups. Changes in
Changes in IL-8 levels during the initial 12 days after treatment differed significantly between the two groups; IL-8 levels increased by 0.20±0.08 ng/mL from baseline in the UCB group, but not in the control group (P<0.05). At 90 days post-treatment, IL-8 levels showed no significant difference between groups (Fig. 3B; Supplementary Table S9). Meanwhile, IL-10 levels were not significantly different between the study groups at any of the time points examined in this study (Fig. 3C; Supplementary Table S9).
In the UCB group, while increases in PTX3 from baseline to 1-day post-treatment were correlated with improvements in GMPM at 1 month post-treatment (r=0.71, P<0.01), increases in IL-8 level from baseline to 12 days post-treatment were correlated with improvements in GMFM at 6 months post-treatment (r=0.60, P<0.05) (Fig. 4).
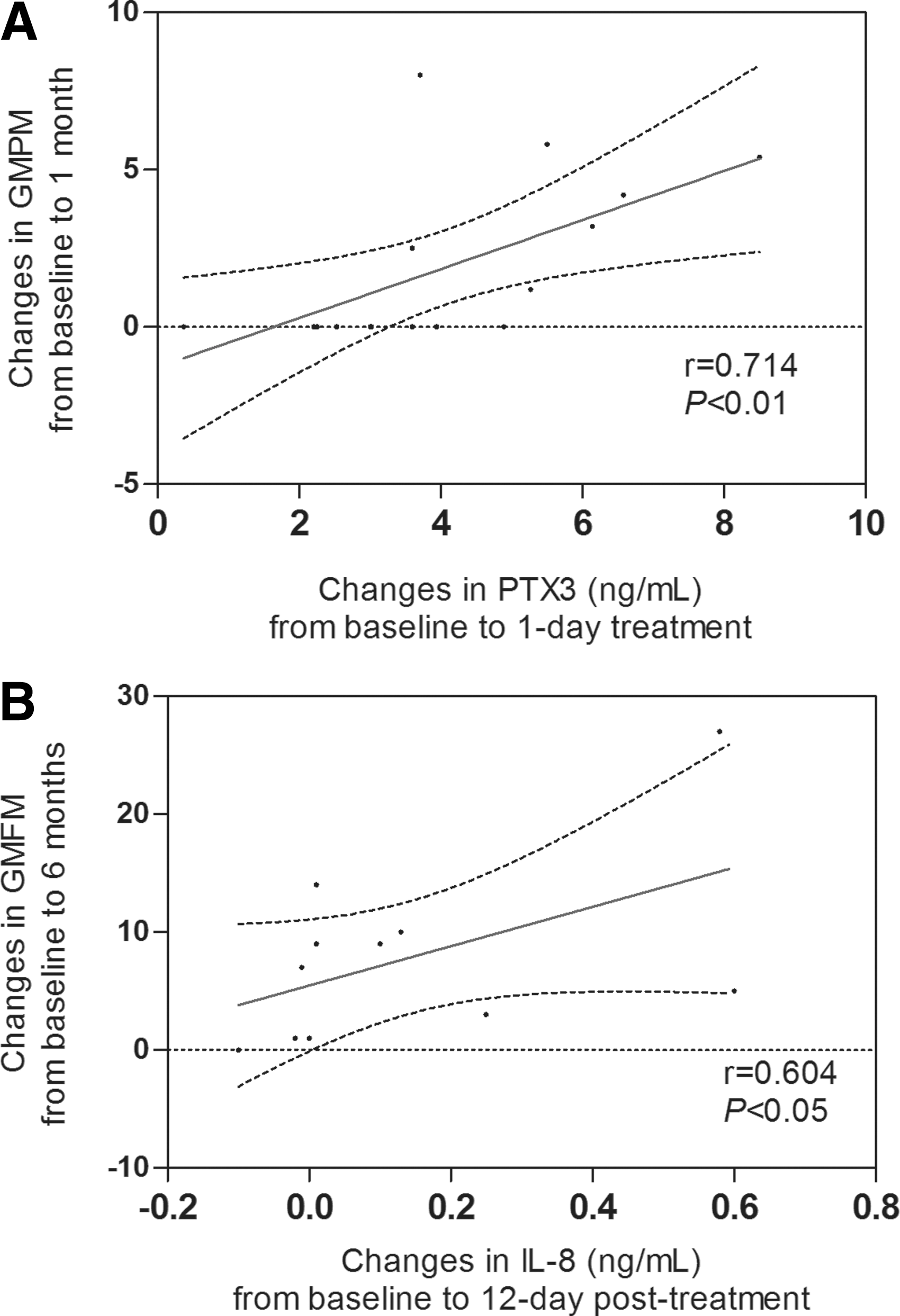
Relationship between changes in plasma cytokine levels and changes in scores of function measure in the UCB group.
TLR4, TLR2, and mTOR levels and functional measures
The age and functional severity of the participants selected from the UCB and control groups for these investigations were not significantly different. Additionally, there were no significant differences in baseline levels of TLR4, TLR2, or mTOR. At 12 days post-treatment, TLR4 levels increased more from baseline in the UCB group (1.77±0.57 ng/mL), than the control group (−1.21±1.85 ng/mL) (P<0.05) (Fig. 5A; Supplementary Table S9). TLR2 levels also increased above those at baseline at 12 days post-treatment (Supplementary Fig. S6). While mTOR levels tended to be elevated at 1 and 12 days post-treatment in the UCB group, there was no significant difference therein in comparison with the control group (Fig. 5B; Supplementary Table S9).
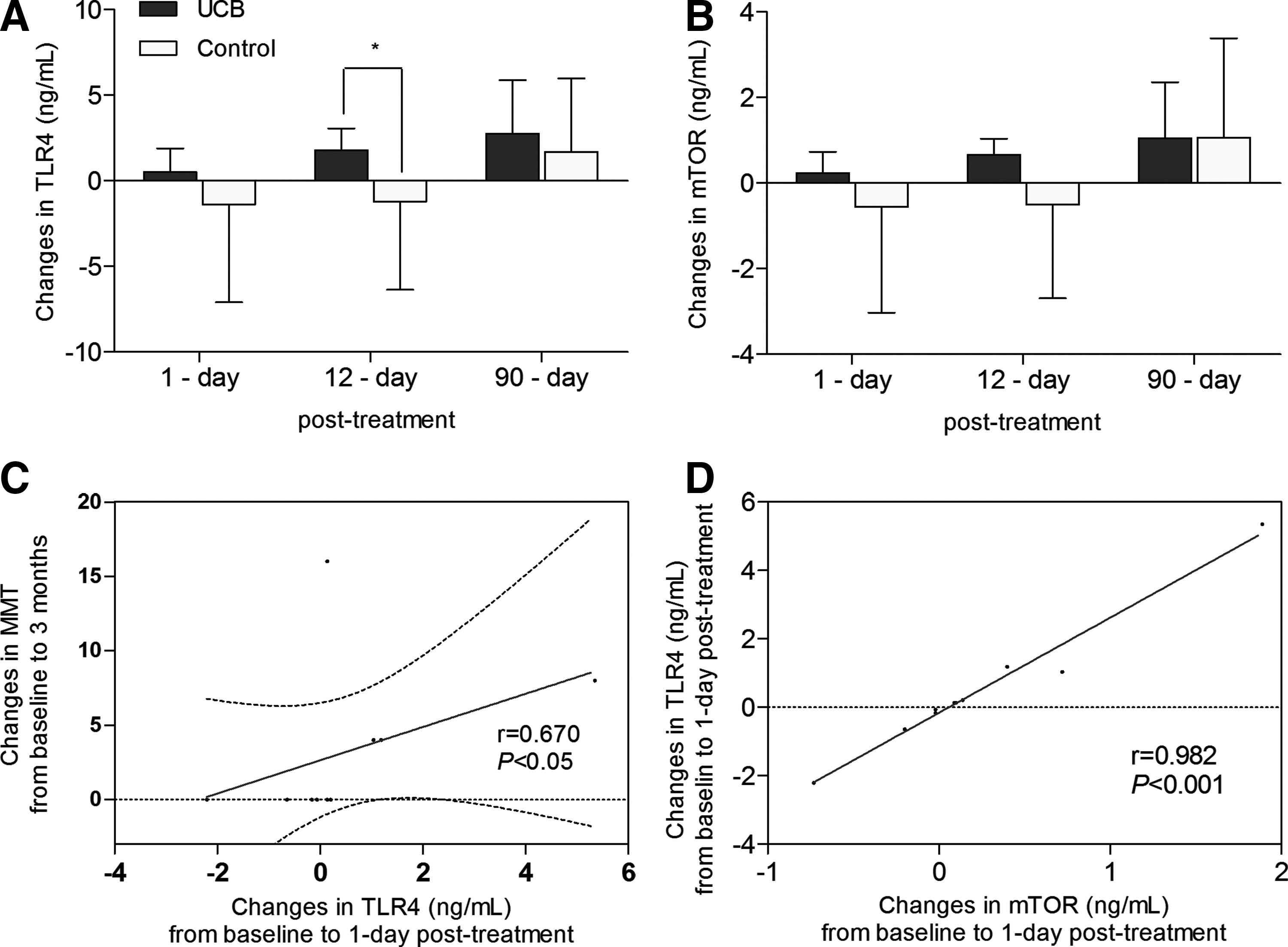
Comparison of TLR4 and mTOR levels between UCB (n=10) and control (n=5) groups and the correlation of TLR4 with functional outcome and mTOR in the UCB group (n=10). Changes in
Increases in TLR4 levels above baseline at 1 day post-treatment exhibited a positive correlation with improvement in MMT at 3 months post-treatment in the UCB group (r=0.67, P<0.05) (Fig. 5C). However, TLR2 levels showed no clear correlation with functional outcomes. Increases in TLR4 and mTOR levels above baseline at 1 day post-treatment were also correlated with each other in the UCB group (r=0.98, P<0.001) (Fig. 5D).
Discussion
In this study, we identified improvements in MMT scores at 1 and 3 months after UCB treatment, which strongly suggested that this treatment can be utilized to effectively alleviate motor impairments in children with CP. The efficacy of treatment with UCB alone was also reflected by improvements in GMPM scores at 6 months post-treatment. However, the improvements in GMPM occurred later and were smaller (increase of 8.5 points) than those observed in our previous study of combined treatment with UCB and EPO, in which GMPM scores had improved by 3 months post-treatment to a larger degree (increase of 11.5 points) [4]. Thus, one could conclude that treatment with allogeneic UCB alone exerts a weaker effect on motor outcomes than combined UCB and EPO therapy. Notwithstanding, treatment with UCB alone led to improvements in MMT scores that were not observed in our previous study, although this may have been related to differences in the targeted muscles (axial muscles were included in this study) and in the subjects' characteristics [4]. Accordingly, since the purpose of this study was to investigate the efficacy of UCB therapy alone, strategies to augment the efficacy of this therapy should be considered in future trials.
Factors that may affect the efficacy of UCB treatments, such as immune compatibility and cell dose, were comparable to our previous trial [4]. Regarding HLA compatibility, fully matched or one-HLA mismatched subjects produced better motor outcomes than the 2-mismatched HLA subjects. This indicated that highly compatible UCB and, ideally, autologous UCB therapy could produce improved therapeutic outcomes in children with CP. Additionally, as the number of cells administered may also be important to the efficacy of UCB treatments, we divided and analyzed subjects treated with UCB alone according to the median number of TNC/kg administered. Although the optimal cell dose was not determined in this study, higher cell doses were correlated with better motor outcomes. Further studies are needed to determine the optimal cell doses for maximizing the efficacies of UCB treatments for CP patients.
Also, in this study, we demonstrated that innate immune responses potentially mediate the therapeutic effects of UCB by identifying correlations between PTX3 and TLR4 levels and functional motor improvements. Herein, elevations in PTX3 and TLR4 early after treatment (1-12 days) were correlated with long-term functional outcomes (at 1-6 months post-treatment). The innate immune system recognizes and reacts to pathogen-associated or danger-associated molecular patterns via pattern recognition molecules. Pattern recognition molecules are classified into two types: cell-associated receptors, represented by TLRs, and fluid-phase soluble molecules, represented by the long pentraxin PTX3 [9]. In our study, plasma levels of PTX3 showed the greatest changes, and the highest correlations with clinical outcomes (Fig. 4A). Recent findings have indicated that PTX3 is not simply a detrimental prognostic marker in inflammatory syndromes or brain injury. In fact, PTX3 deficiency has been shown to be associated with increased lipopolysaccharide-induced lung injury [21] and vascular inflammation [22], indicating a cytoprotective role for PTX3. Moreover, PTX3 reportedly serves a neuroprotective role against seizures [23] and is now suggested to be a candidate anti-inflammatory mediator [24].
TLR4 and TLR2 are cell membrane-bound receptors that act mainly as proinflammatory stimulators of macrophages, lymphocytes, and brain cells [25]. Nevertheless, experiments with TLR4 and TLR2 deficiency models have revealed the importance of these receptors in inflammation control and neuroprotection [26], and in neurogenesis [27]. In this study, TLR4 and TLR2 levels were elevated for up to 12 days post-treatment in the UCB group, although only TLR4 was correlated with motor outcomes. Interestingly, other studies have suggested that PTX3 and TLR4 may be directly related: activation of TLR4 could induce nuclear translocation of NFκB, promoting PTX3 gene expression [28], and PTX3 may influence TLRs [29] to direct cell fate decision making. Moreover, PTX3 and TLR4 have been interpreted as playing a regulatory role in inflammation [30,31]; their linkage with cellular repair and regeneration has also been suggested [12,27]. In the brain, the innate immune system is thought to respond to injury via activation of receptors in microglia, neurons, and astrocytes, to ultimately influence repair processes [32]. Together with the results of this study, we suggest that the therapeutic mechanism underlying the effects of UCB on motor outcomes in CP patients might involve innate immune responses, potentially via PTX3 and TLR4 [33].
Further supporting our hypothesis on the role of immune responses in UCB treatments, increases in IL-8 levels were also correlated with improved motor function in the UCB group. This cytokine is known to be angiogenic [34] and may therefore represent one of the potential effects of UCB treatment on CP. Even though mTOR levels did not change significantly in this study, TLR4 and mTOR showed an almost direct correlation in the UCB group. Reportedly, mTOR is active in regulating cell growth and proliferation, which is likely driven by TLR via the PI3K/Akt axis [35]; this may have played an indirect role in the UCB effects observed in this study.
Further expounding our findings, we suggest that the effects of UCB therapy are mediated mainly by immunomodulation or neurotrophic factors [36,37] rather than cell replacement. Presumably, microglia in the brain are involved in the initiation of innate immune responses to the cell therapy [38]. In support of this notion, one study demonstrated that intravenous cells modulate brain microglia toward anti-inflammation [39]. Such changes in microglia are supposed to impede apoptosis and induce restorative effects. To confirm our suspicions, use of a PET radiotracer targeting microglia would be helpful in future trials [40]. In our study, we identified anti-inflammatory findings [41] using18F-FDG-PET at 2 weeks after UCB treatment. The findings were remarkable at periventricular areas of the occipital and temporal lobes, the main locations of exaggerated inflammation and apoptosis in periventricular leukomalacia. This is relevant because periventricular leukomalacia is the most frequent cause of CP [42]. The PET finding can be interpreted as a treatment-related amelioration of brain tissue inflammation, despite elevations in serum biomarkers of inflammation at comparable time points: increases in IL-8, PTX3, and TLR4 levels were discovered at 12 days post-treatment, while 18F-FDG-PET findings were noted at 14 days post-treatment. Meanwhile, in contrast to the periventricular areas, frontal motor cortices in subjects of the UCB group showed increased glucose metabolism, which was different from the non-specific findings observed in the control group. We interpreted this to indicate an activation of motor function as a result of the UCB treatment.
In terms of route of cell administration, we attempted intra-arterial approach for older subject expecting higher efficacy than intravenous administration [43] because therapeutic efficacy did not appear to be evident in older children with CP in our previous trial [4]. Nevertheless, the intra-arterial approach did not appear to facilitate remarkable differences in treatment efficacy. Consequently, intravenous administration appeared to be the most rational approach.
This study has several limitations that warrant consideration. First, loss of follow-up data at 6 months, especially MMT, led to incomplete results, which might have generated the insignificance of MMT scores at 6 months post-treatment. Second, measurement of TLR4, TLR2, and mTOR receptors along the membranes of blood cells can be affected by total protein levels. To avoid inaccuracies, however, TLR4, TLR2, and mTOR levels were normalized using sample protein level/average protein level ratios. Third, our immune response findings in patients who received UCB therapy do not definitively demonstrate the direct involvement of the mechanism we proposed. To confirm the proposed relationships, the effects of UCB treatment should be investigated in animals in which TLR4 and/or PTX3 are suppressed. Fourth, cyclosporine was administered as an immunosuppressant in UCB group subjects, and this compound exhibits neuroprotective properties [44]. As well, cyclosporine is also known to suppress T lymphocyte activation [45], and its anti-inflammatory, antioxidative, and antiapoptotic actions are thought to exert neuroprotection [46]. Thus, further trials are needed to outline the effects of cyclosporine in allogeneic cell therapy by adding another group that does not receive cyclosporine.
In conclusion, treatment with allogeneic UCB alone improved motor outcomes in children with CP and proved to be therapeutically effective. Assays of inflammatory markers in the blood indicated that innate immune responses potentially mediate the therapeutic efficacy of UCB. Further studies are required to elucidate the mechanisms involved in cell therapy for brain injury patients and the role of immune responses therein.
Footnotes
Acknowledgments
UCB units used in this study were provided by “CHA Medical Center Cord Blood Bank.” This study was supported by CHA Bundang Medical Center, a grant of the Korean Health Industry Development Institute (HI3C1204), HSLee Welfare Foundation, and Gachon University Gil Medical Center (grant number: 2013-52). We appreciate Sunhee Lee R.N. for devoted assistance for conduction of the study and Anthony Thomas Milliken for his help with the editing of this article.
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.