
Abstract
Peripheral blood stem cell (PBSC) collection has been increasingly more popular than bone marrow donation, but little side effects induced by hemogram variation of donors for PBSC collection were reported. The peripheral blood cells were counted pre- and post-collection of PBSC from 166 allogeneic-related donors. Donors' hemoglobin concentration decreased from 144.95 (±16.175) g/L to 139.12 (±13.684) g/L (P < 0.05) and platelet counts decreased from 234.51 (±60.925) × 109/L to 93.00 (±28.439) × 109/L (P < 0.001) after sequential PBSC collections. The anemia condition was weakly correlated (r = 0.297, P < 0.02) and the decrease of platelet counts was strongly correlated (r = 0.719, P < 0.001) to the blood cells in the collection products. The hemoglobin concentration decrease had no significant difference in all four age groups between pre- and post-collection (P ≥ 0.05), but was significantly decreased between pre-collection and post-first collection, post-second collection (P < 0.05 and P < 0.001) in all the body mass index (BMI) groups, among which the underweight group was highly decreased. Neither of the BMI groups nor age groups indicated any statistical difference on platelet counts (P > 0.05). A slight decrease of hemoglobin and a significant decrease of platelet counts occurred after sequential PBSC collection, which was tolerable for donors younger than 60 years old. The collection characteristic of underweight persons should be fine-tuned to ensure their safety. The platelet decrease was independent of ages or BMI values.
Introduction
H
Materials and Methods
Research subject
Between January 2013 and December 2014, 166 allogeneic-related donors of hematopoietic stem cells were selected and mobilized by granulocyte-colony stimulating factor (G-CSF) at the First Affiliated Hospital of Medical School of Zhejiang University, China. Among the donors, 86 were male and 80 were female, with a median age of 40.5 years old (15–60 years old), a median body weight of 62 kg (40–110 kg), a median height of 165 cm (145–185 cm), and a median body mass index (BMI) of 23.1 kg/m2 (16.2–33.1 kg/m2) (Table 1). This study complied fully with all provisions of the Declaration of Helsinki. All donors gave written informed consent to participate. This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Medical School of Zhejiang University.
BMI, body mass index.
Laboratory methods
All the donors received G-CSF 5–10 μg/kg/day until PBSC collection finished. The actual PBSC collection date was on the third day for the 20 donors and on the fourth day for the other 146 donors. COBE® Spectra Apheresis System 6.1 (Terumo BCT) was programmed for mononuclear cell (MNC) collection, and the blood treatment volume was set to 1.5–2.5 times of the donor's total blood volume (7,000–11,000 mL). Acid citrate dextrose (ACD) was used as an anticoagulant, and the flow rate was set at 30–75 mL/min, and the collections were conducted twice sequentially. A small amount of mixed collection product was used for the suspension counting of MNC and CD34+ cells. The total amount of MNC and CD34+ cells in each product was calculated accordingly. The complete blood cell counts were measured in the samples before the mobilization and collection and after each collection and from the donors' peripheral blood and the collection products by a Coulter blood cell counter.
Statistical analysis
The SPSS 19.0 software was used for conducting statistical analysis. Median ± interquartile range was used for non-normal distribution, and “
Results
The effects on white blood cells, red blood cells, and platelets after sequential collection
The effects on white blood cells, red blood cells, and platelets after sequential collection are as follows (Table 2). Compared with the level of pre-mobilization (baseline), the platelet count decreased (t = 3.240, P < 0.001), while white blood cell count increased (t = 38.440, P < 0.001) before PBSC collection. However, the hemoglobin concentration has no significant differences between pre-mobilization and pre-collection (t = 1.496, P = 0.136). While comparing with the level of pre-collection, the hemoglobin concentration decreased after the first collection (t = 2.265, P < 0.05) and the second collection (t = 2.435, P < 0.05). Similarly, the platelet count also decreased (t = 12.734, P < 0.001, t = 23.578, P < 0.05). Nevertheless, no statistically significant differences of white blood cells were observed (t = 0.739, P = 0.461, t = 1.613, P = 0.108).
Compared with the stage of pre-mobilization, P < 0.001.
Compared with the stage of pre-mobilization, P > 0.05.
Compared with the stage of pre-collection, P > 0.05.
Compared with the stage of pre-collection, P < 0.05.
The correlation between blood cells in the collection product and the decrease of peripheral blood cells
We counted the blood cells in two collection products separately and put them together. On one hand, the hemoglobin concentration in the product was 24.14 (±9.88) g/L, which was weakly correlated with the hemoglobin concentration decrease in peripheral blood (r = 0.297, P < 0.02) (Fig. 1). On the other hand, the platelet count in the collection product was 4.06 (±1.17) × 1012/L, which was highly correlated with the platelet count decrease in peripheral blood (r = 0.719, P < 0.001) (Fig. 2).
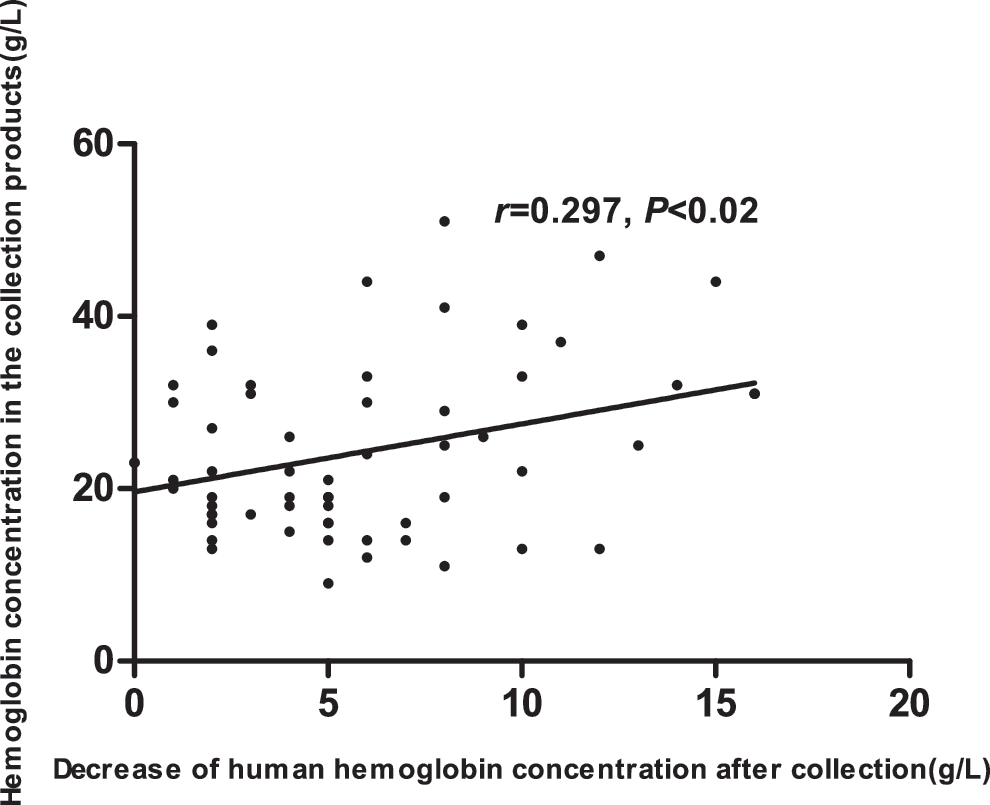
Hemoglobin concentration correlation between collection products and peripheral blood after the PBSC collection. The hemoglobin concentration in product was weakly correlated with the hemoglobin concentration decrease in peripheral blood (r = 0.297, P < 0.02). PBSC, peripheral blood stem cell.
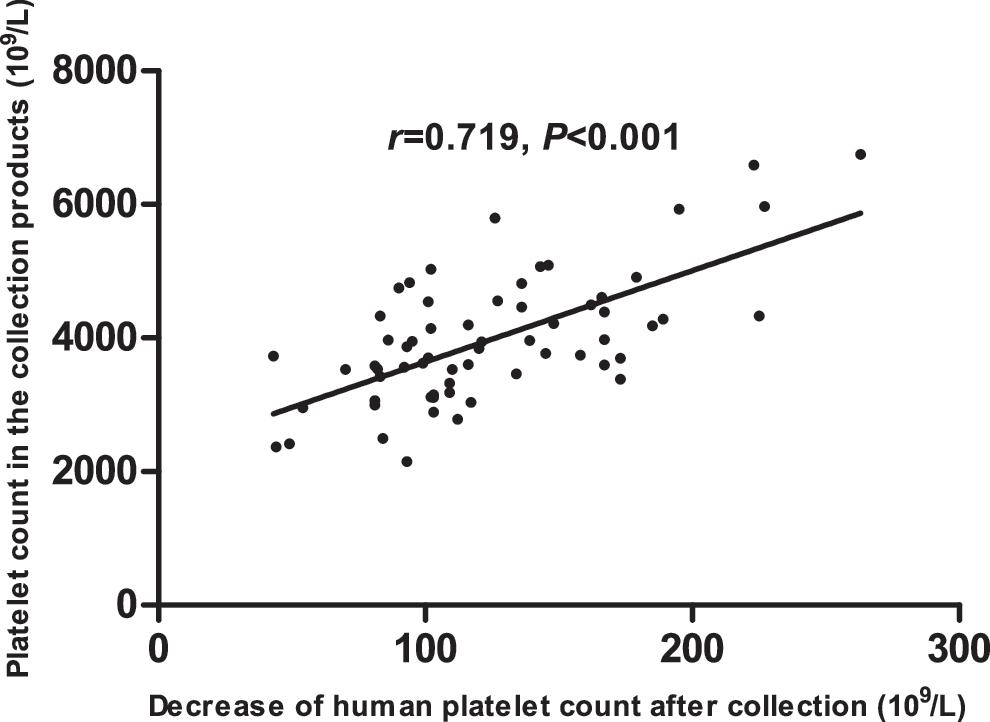
Platelet count correlation between collection products and peripheral blood after the PBSC collection. The platelet count in the collection product was highly correlated with the platelet count decrease in peripheral blood (r = 0.719, P < 0.001).
The effects of age on blood cell counts
We divided the donors into four age groups of ≤29, 30–39, 40–49, and ≥50 years old. The hemoglobin concentration and platelet count differences were compared between pre- and post-collection. We found out that the hemoglobin concentration significantly decreased in all four age groups between pre-collection and post-second collection (P < 0.05); however, there was no significant difference between any of the age groups (P ≥ 0.05). Neither was there any significant difference on platelet counts between any of the age groups (Table 3).
There was no significant difference between any of the age groups (P ≥ 0.05).
The effects of BMI on blood cell counts
Furthermore, the donors were divided into four groups according to their BMI values: underweight, normal, overweight, and obese. The hemoglobin concentration and platelet count differences were compared between pre- and post-collection. We found out that the hemoglobin concentration significantly decreased in all four BMI groups between pre-collection, post-first collection (P < 0.05), and post-second collection (P < 0.001). Among which, the underweight group decreased most. None of the BMI groups indicated any statistical differences on the platelet counts (P > 0.05) (Table 4).
Compared with the normal group, P < 0.05.
Compared with the underweight group, P < 0.02.
Compared with the underweight group, P < 0.01.
Underweight: BMI <18.5 kg/m2; normal: BMI 18.5–23.9 kg/m2; overweight: BMI 24.0–27.9 kg/m2; obese: BMI ≥28 kg/m2. There was no significant difference between other two groups (P ≥ 0.05).
Discussion
Peripheral blood usually contains very low amount of stem cells. CD34+ cells only account for 0.01%–0.1% of peripheral MNCs. Efficient mobilization could increase the PBSC tens to even hundreds of times with strong self-renewal and reproducing capability. It is generally recognized that PBSC donors are much less challengeable than bone marrow donors [4,5]. However, PBSC donors possess other stressful factors, including subcutaneous injection of G-CSF. The short-term and long-term effects of G-CSF on donors' health have not yet been thoroughly verified [6 –9]. Recently, it has been reported that G-CSF might induce hypercoagulability state in healthy donors [10 –12]. Compared to bone marrow transplantation, the major advantages of PBSCT are higher stem cell doses and more rapid engraftment, associated with reduced infectious complications and increased likelihood of graft-versus-host disease, potentially leading to a favorable graft-versus-tumor effect [13,14]. Current data have shown that the side effects on donors arising from allogeneic PBSC were much fewer than those from bone marrow transplantation [15]. Originally, PBSC was only used in related donors, but it has been gradually applied in unrelated donors since the accumulation of PBSC safety data. Two crucial factors on allogeneic PBSCT are donors' safety and the satisfactory collected products for the treatment of patients. When it comes to donors' safety, the two major concerns are G-CSF dosages and the cycles of PBSC separation. Because sufficient amount of CD34+ cells are required for a good clinical outcome, multiple cycles of PBSC collections are usually required [13].
Cooling et al. [16] found that CD34+ cells decreased on the fifth day even though the total white blood cells kept increasing. Flommersfeld et al. [3] also reported that it was more effective to collect PBSC on the fourth day rather than on the fifth day. Thus, all donors in our hospital received G-CSF with the dosage of 5–10 μg/kg/day till collection finished and collection started after 3–4 days of mobilization.
Chen et al. [17] pointed out that right after the PBSC separation the hemoglobin concentration in the PBSC donors decreased, but it was still in the normal range. Platelet counts decreased slightly 5 days after the G-CSF stimulation and then it significantly decreased after the PBSC separation process. We found that the donors' hemoglobin concentration decreased after the first and the second PBSC collection and still higher or near low limit of normal value, which was consistent with what was reported by Chen et al. [17]. We also noticed that the platelet count decreased 3–4 days after the G-CSF stimulation. During which, detailed mechanism was not yet clear. Furthermore, platelet count was significantly affected by each PBSC collection and this result was also in accordance with Chen et al. results [17]. Since the platelet count decreases at an average of 33%–34.5% after each collection, the bleeding condition should be closely observed for those donors whose platelet count decreases at the beginning. Platelet should be infused when necessary to prevent clinical bleeding. National Marrow Donor Program (NMDP) of the United States suggested that collection safety should be a concern if the donors have platelet counts less than 120 × 109/L on the first day of collection or 80 × 109/L on the second day of collection to avoid platelet counts less than 50 × 109/L after collection [18].
Why did the hemoglobin concentration and platelet count decrease after PBSC collection? To answer this question, we analyzed the data of hemoglobin concentration and platelet count in both collection products and in the peripheral blood. We found out that red blood cell counts in the collection products were weakly correlated to the red blood cells decrease in the peripheral blood, which suggested that the mechanical destruction and removal of red blood cells during collection may contribute to the decrease of hemoglobin concentration in peripheral blood. The platelet count in the collected products was strongly correlated with the decrease of platelet count in the peripheral blood, which meant the platelet contamination in the collection products was the major reason for platelet count decrease in the donors.
Although there were significant differences of hemoglobin between pre- and post-collections in each age group, no significant differences could be observed between the different groups, neither were there any significant differences of platelet count observed. These results suggested that the current separation technique was safe for healthy donors below the age of 60. None of the donors reported any obvious dizziness, headache, or clinical bleeding tendency. Hemoglobin concentration significantly decreased in all four BMI groups between pre-collection and post-first and post-second collection. The difference between the normal group and the overweight group was most significant after the first collection. The differences were most significant between the underweight group and the overweight group and between the underweight group and the obese group after the second collection. It should be noticed that the decreasing amount of hemoglobin concentration in the underweight group was far more than those in the overweight group and the obese group. This could be attributed to fewer underweight donors and deviations from the collection characteristics. Therefore, the collection characteristic of underweight donors should be fine-tuned to ensure their safety.
After the PBSC collection, our continued follow-up found that most of the donors' white blood cell counts returned to the normal range 1 month after G-CSF stimulation. All of the donors' hemoglobin concentration went to normal range without any significant difference from pre-collection level. One month after PBSC collection, the average platelet count was recovered in the normal range; however, it took 3 months or longer [19] for the platelet count to return to baseline level, since the platelet count has a broad normal range. Kindwall-Keller [20] reported that 20 days after the PBSC collection, the platelet counts started to increase. Notably, there were no donors that showed any clinical symptoms such as bleeding or thrombosis from G-CSF mobilization by the end of the first month's follow-up observation, and therefore, no treatment was necessary. All their physical condition scores of ECOG Performance Status were 0.
In conclusion, sequential PBSC collections were tolerable for healthy donors from Chinese population below the age of 60, although the hemoglobin concentration had slightly decreased. The collection characteristic of an underweight person should be fine-tuned to ensure their safety. Although there were some risks of platelet count decrease, such decreases were not affected by ages or BMI values and were tolerable for all the donors. Overall, it was safe to collect PBSC once or twice from the donors using the COBE Spectra 6.1 blood cell separator. Further investigation is necessary to clarify whether more times of sequential PBSC collection will cause the donors to have more severe anemia or bleeding.
Footnotes
Acknowledgment
This work was supported, in part, by the Research Plan from the National Natural Science Foundation of China (no.81372256).
Author Disclosure Statement
No competing financial interests exist.