
Abstract
miRNAs as non-coding, short, double-stranded RNA segments are important for cellular biological functions, such as proliferation, differentiation, and apoptosis. miRNAs mainly contribute to the inhibition of important protein translations through their cleavage or direct repression of target messenger RNAs expressions. In the last decade, miRNAs got in the focus of interest with new publications on miRNAs in the context of different diseases. For many types of cancer or myocardial damage, typical signatures of local or systemically circulating miRNAs have already been described. However, little is known about miRNA expressions and their molecular effect in skeletal diseases. An overview of published studies reporting miRNAs detection linked with skeletal diseases was conducted. All regulated miRNAs were summarized and their molecular interactions were illustrated. This review summarizes the involvement and interaction of miRNAs in different skeletal diseases. Thereby, 59 miRNAs were described to be deregulated in tissue, cells, or in the circulation of osteoarthritis (OA), 23 miRNAs deregulated in osteoporosis, and 107 miRNAs deregulated in osteosarcoma (OS). The molecular influences of miRNAs regarding OA, osteoporosis, and OS were illustrated. Specific miRNA signatures for skeletal diseases are described in the literature. Some overlapped, but also unique ones for each disease exist. These miRNAs may present useful targets for the development of new therapeutic approaches and are candidates for diagnostic evaluations.
Introduction
miRNAs and their relevance in diseases
M
The prefix “miR-” presents the nomenclature for the mature form of the miRNAs. A lower case letter a, b, or c is added if miRNAs present nearly identical sequences, except for one or two nucleotides. The suffix -3p or -5p is added to the description, if two mature miRNAs originate from opposite arms of the same pre-miRNA. The suffix -1 or -2 refers to pre-miRNAs that lead to an identical mature miRNA, but are located in different genome regions.
To date, 2,588 mature miRNAs have been identified in human cells (miRBase version 21;
In the last decade, miRNAs have been attracting increasing attention in the scientific community with new publications on miRNAs in the context of different diseases. For many types of cancer or myocardial damage, typical signatures of local or systemically circulating miRNAs have already been described [9,10]. In cardiology research, the activation of a specific signature of differentially regulated miRNAs after ischemic heart disease could be detected through systemic screening of circulating miRNAs [11]. Further investigations showed that many of the detected miRNAs are involved in the pathogenesis of ischemic heart disease. Thus, it is proposed that inhibiting the respective miRNAs could be used as therapeutic targets [12]. Demonstrated by another study, miRNAs also have a regulative effect on the differentiation of stem cells into heart muscle cells [13]. Besides the investigation of the important intracellular influence of miRNAs for the development of new therapeutic approaches, analysis of freely circulating miRNAs is also of interest in view of new diagnostic methods. Thereby, changes of miRNAs are possibly earlier detectable than protein-based biomarkers. Moreover, miRNAs show resistance to RNAase activity in the peripheral blood [14].
miRNA signatures are mostly known in association with cancer, but little is known about their expression and effects in skeletal diseases of human individuals. This review summarizes the regulation of miRNAs in human skeletal diseases, such as osteoarthritis (OA), osteoporosis, and osteosarcoma (OS). Up to now, no specific miRNA signatures are known for osteomalacia and osteopenia.
The skeleton
The skeleton, as the supporting structure of an organism, serves as a reservoir for minerals and is the location for blood cell production [15]. Different cells residing on the trabecular surface of the adult bone are responsible for a permanent, well-balanced construction, and degradation of the bone. The main three cell types involved in the bone homeostasis include bone-forming osteoblasts, bone-degrading osteoclasts, and osteocytes. Osteoblasts serve as producer of the organic bone matrix and aid its mineralization [16]; osteoclasts, a unique exocrine cell type, dissolve bone minerals and enzymatically degrade extracellular matrix proteins [17]; and osteocytes, postmitotic osteoblasts reside in the bone matrix, act as mechanosensors and endocrine cells [18].
Skeletal fragility is caused by excessive bone resorption, inadequate formation response during the bone remodeling or inefficacy to produce the optimal bone mass [19]. miRNAs may have a crucial impact on these metabolic mechanisms. An excellent summary of the regulating influence of miRNAs on the cells involved in physiological bone homeostasis is given by Lian et al. [20].
Bone damages can result from different impacts, for example, infections, tumors, and altered metabolic conditions. The most common skeletal diseases comprise fractures, OA, osteopetrosis, osteoporosis, osteopenia, osteomalacia, and OS. However, the probable clinical application of miRNAs in therapeutics for skeletal diseases depends heavily upon the detailed understanding of miRNAs and their targets. Thus, this review aims to give an overview of miRNA in musculoskeletal diseases and make relations to the tissues involved, such as bone and cartilage, concerning regeneration and degradation.
Materials and Methods
Literature study
Relevant articles were identified by a systematic search using the database PubMed with the keywords “miRNA” AND (“osteoarthritis” OR “osteoporosis” OR “osteosarcoma”) in the title or abstract. It was also searched for “osteopetrosis,” but as this returned in only one article [21], it was decided to leave this disease entity out. Furthermore, articles dealing with regeneration or degradation of tissues related to the abovementioned musculoskeletal diseases were taken into consideration. Search keywords were “miRNA” AND [(“cartilage” OR “bone”) AND (“degradation” OR “regeneration”)]. For this review, the used articles have to match the following inclusion criteria: (1) listed in PubMed, (2) written in English language, (3) the article presents original data.
Results
Osteoarthritis
OA, also termed degenerative arthritis or degenerative joint disease, goes along with chronic degenerative joint changes and cartilage degradations resulting in pain and functional limitations. The most prominent risk factor for the initiation and progression of primary OA is the increased age of the patients [22]. Worldwide, 9.6% of men and 18% of women aged over 60 years suffer from symptomatic OA [23]. Besides hereditary deficiencies, the loss of cartilage is due to developmental, metabolic, and mechanical deficits.
Chondrocytes, the single cellular component of adult hyaline cartilage, show specific physiological changes when obtained from patients with OA. The cells display an increased cell proliferation, a higher proteinase and catabolic cytokine production, a higher apoptotic rate, and the expressions of collagen types VI, III, X, and IIA are higher compared with healthy volunteers [24]. On the contrary, the OA chondrocytes show a decreased synthesis of collagen type II and aggrecan, which are most important for cartilage formation.
miRNAs associated with OA identified in tissue, cells, and in the circulation are summarized in Table 1. Thereby, the best analyzed ones seem to be miR-9, miR-140, miR-146, miR-223, and miR-483. For most miRNAs, the same expression patterns between tissue, cells, and circulation were found. Only miR-26 and miR-140 displayed different expression patterns. Interestingly, miR-146 displayed decreased expression during disease progress.
↓ = lower expressed, ↑ = higher expressed, →↓ = down-regulated over disease progress, / = not yet analyzed.
The influence of specified miRNAs on cartilage degradation and inhibition of regeneration processes are described in the following sections.
Cartilage degradation-related miRNAs
The flexible connective cartilage is strongly influenced by miRNAs and their influence on degradation processes (Fig. 1A). Many OA-associated miRNAs show repressing effects on the important matrix gene MMP-13 [25 –28]. This gene is known to have the capacity to degrade a wide range of matrix components such as different types of collagen; this makes it a key player in cartilage biology and OA pathology. In view of miRNAs, Jones et al., by analyzing human OA cartilage, could identify a higher expression of miR-9, that is involved in the regulation of MMP-13 expression and in combination with the higher expressed miR-98 and lower expressed miR-146 in the control of tumor necrosis factor (TNF)-α expression [29]. miR-130a correlates with TNF-α during the development of OA [30].
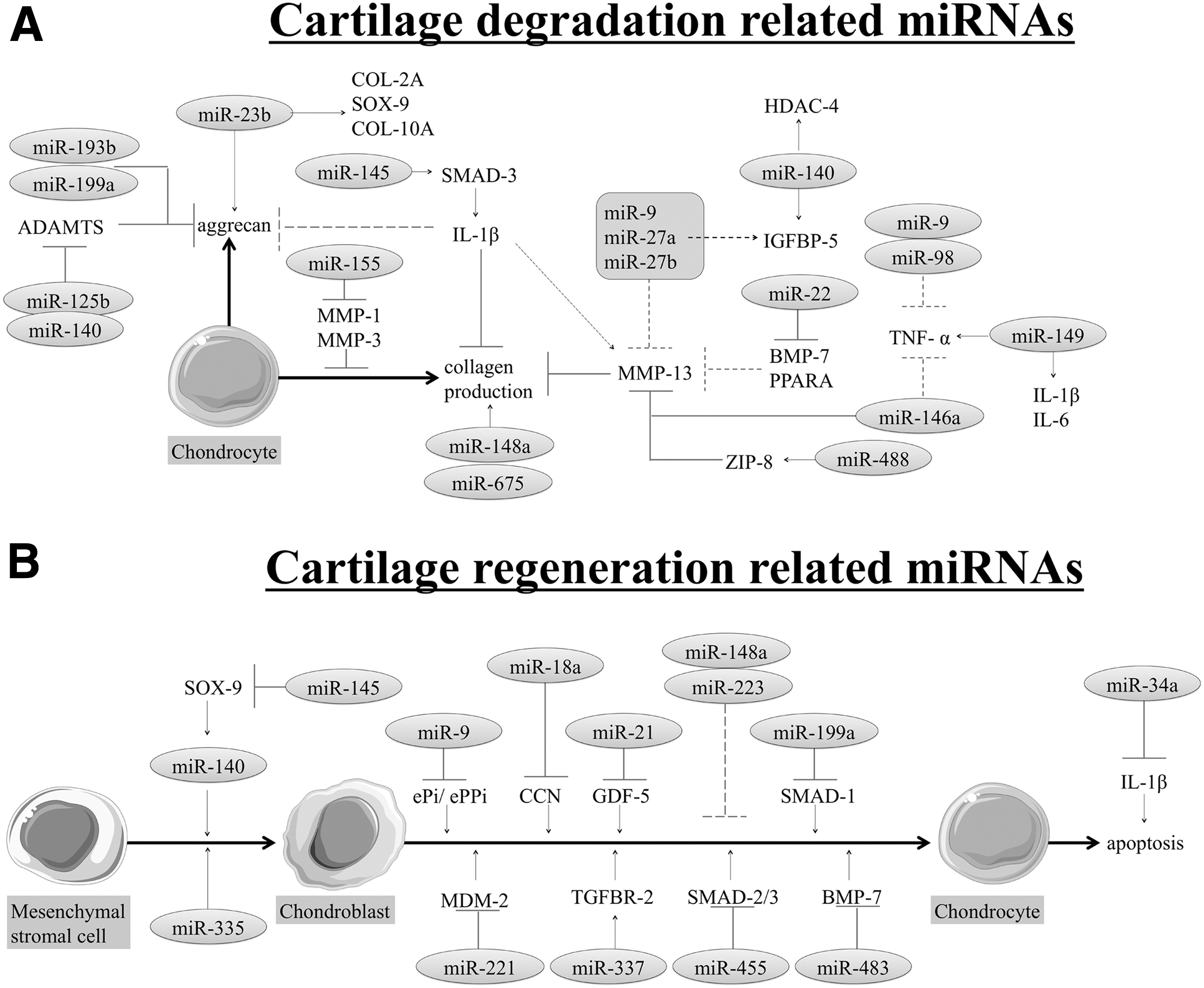
Presentation of miRNAs associated with OA. miRNAs either involved in cartilage development
The dysregulation of miR-9, miR-98, and miR-146 suggests that these miRNAs may play a protective role in OA. This was also assumed by Li et al., whereas they could also identify miR-183 beside miR-146a [31]. Lower expression of both miRNAs in the central compartments was closely associated with the higher expression of inflammatory pain mediators responsible for OA joint pain. For miR-146a, a strong expression in OA chondrocytes could also be detected, which gradually decreased during progressive tissue degeneration [32,33]. Furthermore, high expression patterns of miR-146a were associated with MMP-13 inhibition.
miR-22, which is highly expressed in OA tissue, cells, and circulation directly inhibits peroxisome proliferator-activated receptor and BMP-7 at the mRNA and protein levels, resulting in an increased MMP-13 activation, respectively [34]. For miR-27, different results were obtained. Tardif et al., who detected higher levels of miR-27a expressions in OA chondrocytes compared with healthy controls, suggested that miR-27a may indirectly regulate the levels of both MMP-13 and IGFBP-5 by targeting upstream positive effectors of both genes [28]. In contrast, miR-27b expression was found to be significantly lower in OA cartilage samples compared with their normal counterparts and was inversely correlated with the expression of MMP-13 [35].
Investigations by Yang et al. have shown that miR-145 directly regulates SMAD-3 expression, contributing to interleukin (IL)-1β-induced impairment of COL2A1, aggrecan, and MMP-13 [36,37]. Described by Song et al., miR-488 was significantly decreased in OA chondrocytes. Furthermore, they could show that miR-488 positively influenced the chondrocyte differentiation and cartilage development by inhibiting MMP-13 activity through targeting ZIP-8 [38]. They could also show that miR-222 regulates MMP-13 through targeting HDAC-4 [27].
Collagen type II and aggrecan are the most important factors for cartilage building. Aggrecan expression is induced by several miRNAs as for example by miRNA-23b. Its expression increased during chondrogenic differentiation of OA synovial fluid cells and led to higher gene expressions of COL-2A, SOX-9, COL-10A, and aggrecan after overexpression [39]. miR-125b was expressed in both healthy and OA chondrocytes, whereas the expressions were significantly lower in chondrocytes from OA patients compared with chondrocytes from healthy volunteers [40]. Decreased miR-125b led to a higher expression of ADAMTS-4 resulting in the degradation of aggrecan [41].
Similar regulating effects were found when analyzing miR-140, which plays an important role in the OA pathogenesis by targeting ADAMTS-5, IGFBP-5, and HDAC-4 [28,42,43]. For the last mentioned target, miR-365 also seems to play a role during OA and is induced by IL-1β and mechanical stress [44]. As two further aggrecan production-inhibiting miRNAs, miR-193b and miR-199 could be identified [45]. Another study identified a decreased miR-148a expression in OA chondrocytes. By overexpression of this miRNA, the production and deposition of collagen type II could be improved, which led to an increased retention of proteoglycans [46]. Similar effects were reported for miR-675 [47].
miR-149 was found to be lower expressed in OA human primary chondrocytes. This lower expression seems to increase the expression of proinflammatory cytokines, such as IL-1β, IL-6, and TNF-α [48]. miR-155 is higher expressed in rheumatoid arthritis synovial fibroblasts and had repressive effects on the expression of MMP-1 and MMP-3, which underlines the miRNA modulation properties of the destructive processes in OA [49].
Cartilage regeneration-related miRNAs
Besides miRNAs responsible for cartilage degradation, miRNAs are also involved in the inhibition of OA regeneration (Fig. 1B). Some miRNAs could be identified to influence the chondrogenic differentiation of mesenchymal stem cells (MSCs). Yang et al. for example observed the regulation of miR-140 by miR-145 and the Wnt/β-catenin signaling. Thereby, miR-145 inhibited SOX-9, which in turn regulates miR-140 expression. Conversely, SOX-9 and aggrecan proteins are highly expressed after stimulation with miR-140 [50]. Thus, miR-140 is positively associated with chondrogenesis [51]. These interactions influence the cartilage homeostasis and development, including chondrogenesis and endochondral ossification in MSCs [52]. Furthermore, miR-31, miR-181a, miR-201, miR-335, and miR-574 were identified to regulate the chondrogenic differentiation processes of MSCs [51,53,54]. This is in accordance with the presence of this miRNA in precursor chondrocytes during embryonic development [55]. OA-derived MSCs display a clear trend toward a lower expression of miR-335 compared with MSCs from healthy volunteers [56].
miR-9, which is increased in IL-1β-stimulated human chondrocytes, contributes to the acquirement of an altered chondrocyte phenotype by disrupting the balance of the major regulators of the mineralization process, namely ePi and ePPi [57]. By directly targeting the CNN gene family, miR-18a could also be identified to repress chondrogenesis of cells [58]. An increased miR-21 expression was detectable in OA tissue. Targeting analysis revealed an inhibiting effect of miR-21 on GDF-5, which is important for chondrogenesis [59]. In Sprague-Dawley rats, the silencing of miR-34a could effectively reduce IL-1β-induced apoptosis of rat chondrocytes [60]. Similarly, miR-29a and miR-140 are protective against IL-1β-induced proliferation stop and matrix signaling changes [61].
miR-148a expression, which is decreased in OA chondrocytes, results in the inhibition of hypertrophic differentiation when being higher expressed [46]. miR-199a identified during chondrogenic differentiation targets SMAD-1 [62], whereas SMAD-3 is targeted by miR-16 [63]. It could be shown that in developing cartilage, miR-199a is present in both precursor and hypertrophic chondrocytes [55]. Chondrocyte proliferation and matrix deposition is promoted by miR-210 through HIF-3α and inhibiting NF-κB in OA [64,65], whereas miR-139 inhibits proliferation and migration [66]. Suppressing effects on the chondrogenesis by negatively regulating MDM-2 could be detected by analyzing miR-221 [67].
An overexpression of miR-223, as determined by Shibuya et al., was found in human rheumatoid arthritis synovia compared with the synovia from OA patients. This overexpression results in the suppression of the osteoclastogenesis, which was analyzed with a coculture system [68]. The exact molecular contributions of miR-233 were controversially discussed depending on the cell origin [69]. miR-337 is lower expressed through chondrogenesis targeting TGFBR-2 expression, known for its important role in cartilage development and inflammation [70].
In articular cartilage, the expression of miR-455 was detected during chondrogenesis, where miR-455 regulated TGF signaling and suppressed the Smad-2/3 pathway [71]. Qi et al. examined a murine model and found a significantly higher expressed expression of miR-483 in the cartilage tissues derived from old OA mice [72]. Target identification experiments on mRNA level showed a negative correlation between miR-483 expression and the gene expression of BMP-7, underlining the relevance of miR-483 for the pathogenesis of OA. miR-634 overexpression diminishes extracellular matrix synthesis and survival of OA chondrocytes through PIK3R1 [73].
Summarizing, important genes of the chondrocytes differentiation processes are influenced by the above-described miRNAs. By manipulating these miRNAs, improved differentiation results could be realized; this opens new therapeutic approaches for regenerative processes in OA.
Osteoporosis
As a systemic skeletal disorder, osteoporosis is characterized by a change in the microstructure of bone tissue and a reduction in bone mass, which increases bone fragility and the risk of fractures [19]. Especially the hip, wrist, and spine are affected by fragility fractures. Often only after fragility fracture, patients are diagnosed with osteoporosis for the first time [74]. According to the World Health Organization (WHO), osteoporosis counts to one of the 10 most common diseases, affecting ∼75 million people in Europe, the United States, and Japan. Thirty to 50% of all women and 15%–30% of all men worldwide will suffer from a fracture due to osteoporosis during their lifetime [74]. Patients with osteoporosis suffer from chronic pain, loss of autonomy, and are endangered by increased mortality because of frequently required hospitalization.
miRNAs associated with osteoporosis identified in tissue, cells, and in the circulation are summarized in Table 2. The best characterized ones seem to be miR-21 and miR-133a. For the most miRNAs, the same expression patterns between tissue, cells, and circulation were found. Only miR-21 and miR-125b displayed different expression patterns. Mainly all miRNAs, except miR-10, miR-22, miR-31, miR-210, and miR-503, were higher expressed in tissue and cells from osteoporotic patients. Interestingly, miR-10, miR-22, miR-31, miR-125b, and miR-210 were lower expressed during disease development. Besides miRNAs identified in material of osteoporotic patients, the influence of specified miRNAs on bone formation inhibition and on the support of osteoclastic activity are described in the following sections.
↓ = lower expressed, ↑ = higher expressed, →↓ = down-regulated over disease progress, / = not yet analyzed.
Bone formation-related miRNAs
During lifetime, bone undergoes radial and longitudinal growth, modeling, and remodeling. The osteoblasts, osteoclasts, and osteocytes participating in bone homeostasis are the major players for skeleton integrity. Interactions of these three cell types are detailed described by Crockett et al. [75]. In osteoporosis, an unbalance of bone resorption and bone formation occurs due to the overactivity of osteoclasts in comparison to osteoblasts. Regarding the inhibition of osteoblasts differentiation and extracellular matrix formation, several miRNAs are described (Fig. 2A). Osteoclasts can also produce miRNAs that inhibit bone formation by osteoblasts [76] showing the intricate relationships between the cells and miRNA.

Presentation of miRNAs associated with osteoporosis. miRNAs either related to bone formation
Transcription factor-inhibiting miRNAs
Several studies found miRNAs that are crucial for regulating the osteoblastic differentiation transcription factors RUNX-2 and OSX. RUNX-2, localized on chromosome 6p21, belongs to the family of runt-related transcription factors and is known to target the important osteogenic genes OC, COL-1α1, BSP, MMP-13, and OP [77]. A mutation of RUNX-2 causes major skeletal phenotype changes, which underlines the master role of it in bone formation processes.
Many identified miRNAs directly inhibit RUNX-2 expression (miR-23a, miR-23a-27a∼24-2, miR-30s, miR-31, miR-103a, miR-133, miR-135, miR-137, miR-204, miR-205, miR-211, miR-217, miR-218, miR-335, miR-338, miR-433, and miR-3077-5p), whereas for example miR-23a and miR-34s inhibited the expression of SATB-2 leading to an inhibition of HOXA-2, which is important for RUNX-2 [78 –89]. miR-23 also inhibits osteogenic differentiation of MSC by targeting LRP5 [90]. Myocyte-enhancing factor 2c is inversely correlated with miR-27 and is associated with osteoporosis, as it was shown to be crucial in MSC osteoblastic differentiation [91]. This may also be related to Sp7 involvement in Satb2-induced osteogenic differentiation [92]. Furthermore, Satb2 is also inhibited by miR-33 [93].
The SMAD family genes, influenced by miR-30s and miR-34s, are also known to induce RUNX-2 gene expression [85]. miR-34 cooperates with miR-145, which inhibits cbfb expression that is important for forming the active RunX2 complex [94].
Another study demonstrated the inhibition of BMP-2-induced osteogenic differentiation by miR-133 and miR-135. miR-133 is postulated as a negative regulator of RUNX-2 and miR-135a is known to trigger SMAD-5, leading to less translation of BMP-2, which is required as an osteogenic signal for bone formation [95]. Indeed, delivering inhibitors of miR-133 to MSC improved osteogenesis on collagen–nanohydroxyapatite scaffolds [96]. Moreover, inhibition of miR-222 induced osteogenesis of MSCs through allowing Smad-5 and RunX-2 activity [97]. miR-196a enhances the proliferation and inhibits the osteogenic differentiation of MSCs through HOX-C8 [98]. Liao et al. ascertained that miR-705 and miR-3077-5p are both significantly higher expressed in MSCs from osteoporotic bone marrow. The inhibition of both miRNAs restored the cell lineage commitment of MSCs through reestablishing the protein levels of RUNX-2 and HOX-A10 [99].
miR-2861, identified in primary mouse osteoblasts, displayed a repressing potential on HDAC-5, an enhancer of the RUNX-2 degradation [79]. Further studies by this group revealed miR-3960 as influencing the differentiation of osteoblasts through a regulatory feedback loop with miR-2861 [100].
OSX, another important transcription factor, is expressed in osteoblasts of all bones developed by either endochondral or intramembranous ossification. In OSX knockout mice, neither endochondral nor intramembranous bone formation occurs and osteoblast differentiation is arrested [101]. OSX is directly inhibited by the miRNAs miR-31, miR-93, miR-125b, miR-143, miR-145, miR-214, and miR-637 [102 –109]. miR-138, lower expressed during differentiation, inhibits the focal adhesion kinase signaling pathway and OSX; this modulates the osteogenic differentiation of human MSCs [110]. miR-141 and miR-200 could be observed to be involved in preosteoblast differentiation by inhibiting the OSX-linked transcription factor DLX-5 [111]. miR-216 targets the transcription factor c-Cbl, a RING-finger E3 ubiquitin ligase, and promotes thereby osteogenesis [112].
Further osteogenic gene-related miRNAs
The differentiation of MSCs to preosteoblasts is influenced by mir-34s, miR-26a/b, and miR-29b. Thereby, miR-26a/b and miR-29b were higher expressed during osteogenic differentiation of unrestricted somatic stem cells and inhibited osteogenesis by targeting the osteoinhibitory genes TOB-1, HDAC-4, CTNNBIP1, CDK-6 and the osteoinducing SMAD-1 [113 –115]. Interestingly, miR-26 inhibits GSK3β in bone marrow-derived MSC to induce osteogenesis, whereas in adipose-derived MSC it blocks Smad-1 and leads to impaired osteogenesis [116]. For miR-29, also an inhibiting effect on OSN was reported [115]. Analyzing the miRNA-family miR-34s (miR-34 a, b, c), an inhibitory effect on the osteoblast proliferation by suppressing CCN-D1, CDK-4, and CDK-6 could be detected. Furthermore, miR-34s inhibited SATB-2, as described in Transcription Factor-Inhibiting miRNAs section [87].
The translation of the important osteoinductive gene BMP-2 is inhibited by the miRNAs miR-135a, miR-149, miR-370, and miR-645. Thereby, miR-135a induced SMAD-5 leading to less translation of BMP-2 [95]. Analyzing miR-149 and miR-645, a negative correlation with mRNA and protein regulation of ALP and BMP-2 during osteogenic differentiation was detectable [117]. Also miR-370 was recently recognized to be relevant for viability and differentiation of MC3T3-E1 cells by inhibiting the expression of BMP-2 and ETS-1 [118]. Moreover, miR-208 could be identified to inhibit the osteogenic differentiation by targeting ETS-1 [119]. Differentiation of MSC was inhibited by miR-153 through inhibiting the expression of BMPR-2 [120]. This leads to the impairment of actions of BMP-2, among others.
Several other miRNAs are described to inhibit the development of preosteoblasts to mature osteoblasts. For example, miR-31 could be identified to inhibit the important gene BMPR-2 [86]. The same inhibitory effect could be seen by analyzing miR-100 [121]. Regarding miR-146a, an inhibitory effect on IRAK-1 was detectable [122]. Osteogenesis and osteoclastogenensis were suppressed through miR-155 by targeting the positive regulators SOCS-1 and microphthalmia-associated transcription factor (MITF) [123,124]. miR-182 is a negative regulator of the osteoblast proliferation and differentiation targets FoxO1 [125].
Decreasing expressions of miR-206 during osteogenic differentiation were recently found and an overexpression of it inhibits the differentiation by targeting CON-43 [126]. Regarding miR-210, an effect promoting osteogenic differentiation by suppressing TGFBR-1 is described [127]. A further study by Wang et al. detected the connection of miR-214 in the bone specimens of elderly patients with fractures with a lower degree of bone formation [128]. The in vitro osteoblast activity and matrix mineralization were promoted by direct targeting of ATF4 through antagomiR-214 and decreased by agomiR-214. The inhibiting effects on WNT/TGF-β signaling molecules were detectable by analyzing miR-221 and miR-1274a [129]. By targeting GALNT-7, miR-378 also negatively regulates osteogenesis [130].
Mature osteoblasts are known to produce extracellular matrix, for which the proteoglycans aggrecan and versican are also essential besides collagen [131]. In this context, miR-124, first described by Laine et al., was found to downregulate both proteoglycans [131]. Osteocytes, the most abundant bone cell type, account for 95% of all bone cells. These cells of osteoblastic origin develop at the end of the bone formation cycle and are incorporated in the bone matrix [75]. The differentiation of mature osteoblasts to osteocytes is inhibited by miR-127 and miR-136. Furthermore, those miRNAs promote cell apoptosis [133].
Osteoclastic activity-related miRNAs
Besides the influence on bone formation, miRNAs are also described to support osteoclastic activity leading to increased bone degradation (Fig. 2B). Several miRNAs have been elucidated in an in vitro study investigating osteoclastogenesis from RAW264.7 cells. Twenty-two miRNAs were higher expressed and 15 were lower expressed [134].
For example, miR-21 is known to go along with the inhibition of PDCD-4, which in turn inhibited the repression of c-Fos, allowing an increased osteoclastogenesis [83,135]. The miRNAs miR-29b and miR-155 were also enhanced by c-Fos. miR-26 inhibits osteoclastogenesis through suppression of connective tissue growth factor [136]. Overexpression of miR-29 inhibited the formation of tartrate-resistant acid phosphatase (TRAP)-positive cells and regulated specific osteoclast transcriptional programs [137]. miR-155 suppressed osteoclastogenesis by targeting the positive regulators SOCS-1 and MITF.
Krzeszinski et al. identified miR-34a as a critical suppressor of osteoclastogenesis, bone resorption, and the bone metastatic niche. miR-34a was lower expressed during osteoclast differentiation and the proosteoclastogenic TGIF2 could be identified as its direct target. In vivo investigations revealed lower bone resorption and higher bone mass in miR-34a-overexpressing transgenic mice. On the other hand, a knockout of miR-34a led to a higher bone resorption and reduced bone mass [138].
miR-133a was identified in human circulating monocytes from postmenopausal women. They showed a higher expression in the patients with low bone mineral density (BMD) compared with the ones with high BMD. Wang et al. hypothesized that miR-133a supports the osteoclastogenesis by a higher expression of the three potential osteoclast-related target genes CXCL-11, CXCR-3, and the SLC39A-1 [139]. By inhibiting OSTM-1, miR-140 was identified to inhibit osteoclastogenesis [140]. Analyzing miR-146a, an inhibiting effect on the development of TRAP-positive multinucleated cells and on the expression of c-Jun, NF-ATc1, PU.1, and TRAP could be detected [141]. miR-148a, which is overexpressed in serum and bone tissue of osteoporotic patients, is known to promote the osteoclastogenesis in CD14+ peripheral blood mononuclear cells by targeting MAFB that negatively regulates receptor activator of NF-κB ligand (RANKL) [83,142].
Also, the lower expression of miR-503 in cells from postmenopausal osteoporotic patients induces osteoclastogenesis by lower inhibition of RANKL [143]. RANKL diminishes the expression of miR-218. The presence of miR-218 inhibits osteoclastogenesis through attenuating the expression of p38, c-Fos, and NF-ATc1 [144]. On the other hand, RANKL induces miR-183. miR-183 diminishes the expression of heme oxygenase 1, which inhibits osteoclastogenesis [145].
By affecting NFIA and MCSF-R, miR-223 also displayed an inhibiting effect on osteoclastogenesis [146]. miR-422a, identified by Cao et al., displayed a higher expression in human circulating monocytes from osteoporotic patients. Following target gene analysis identified the osteoclastogenesis-associated genes CBL, CD226, IGF-1, PAG-1, ERBB-2, and TOB-2 correlating negatively with the miR-422a expression [147]. As a further miRNA-supporting osteoclastogenesis, miR-378 could be identified [148]. Mature osteoclast survival was inhibited through miR-9 and miR-181a by targeting BIM [149].
Osteosarcoma
OS as an aggressive malignant neoplasm accounts for ∼60% of malignant bone tumors with an incidence of 4–5 per million people. OS develops from MSCs, which usually undergo osteoblastic differentiation, but after a transgenic transformation, these MSCs lead to the development of malignant osteoid. OS frequently occurs in the long bones and preferentially metastasizes to the lung [150]. The mainly affected organs are the joint in the tubular long bones, namely femur (42%), tibia (19%), and humerus (10%). On the other hand, the localization of OS in the cranial bone or the spinal column is very rare [151]. As clinical data revealed, OS is of poor prognosis, even with the current treatment, including operation and chemotherapy. Therefore, it is crucial to identify cancer-associated molecules for a better understanding of the molecular mechanism behind OS.
miRNAs associated with OS that were identified in tissue, cells, and circulation are summarized in Table 3. The best characterized ones seem to be miR-21, miR-miR-34a miR-126, miR-133, miR-142, miR-143, miR-145, miR-181a, miR-195, and miR-451. The expression pattern between tissue, cells, and circulation were equivalent, except for miR-16, miR-29, miR-31, miR-126, miR-132, miR-142, miR-150, miR-195, miR-223, and miR-451. Furthermore, different results for the expression could be revealed for miR-16, miR-31, miR-135b, miR-142, miR-150, and miR-223 due to different analyzed OS cells or fresh, frozen, or embedded tissue. Higher expressed miRNAs mainly inhibit the OS process, whereas lower expressed miRNAs support proliferation and invasion. Besides miRNAs identified in tissue and cells of OS, the influence of specified miRNAs on the supporting and suppressing of proliferation and migration as well as chemoresistant/drug-response-associated miRNAs are described in the following sections.
↓ = lower expressed, ↑ = higher expressed, →↓ = down-regulated over disease progress, / = not yet analyzed, s = family.
Proliferation/migration-related miRNAs
As OS is considered to be a disease of cell abnormalities caused by genetic changes, the proliferation of these abnormal cells plays an important role. In the literature, several miRNA associated with the proliferation/migration of OS cells are described (Fig. 3A).
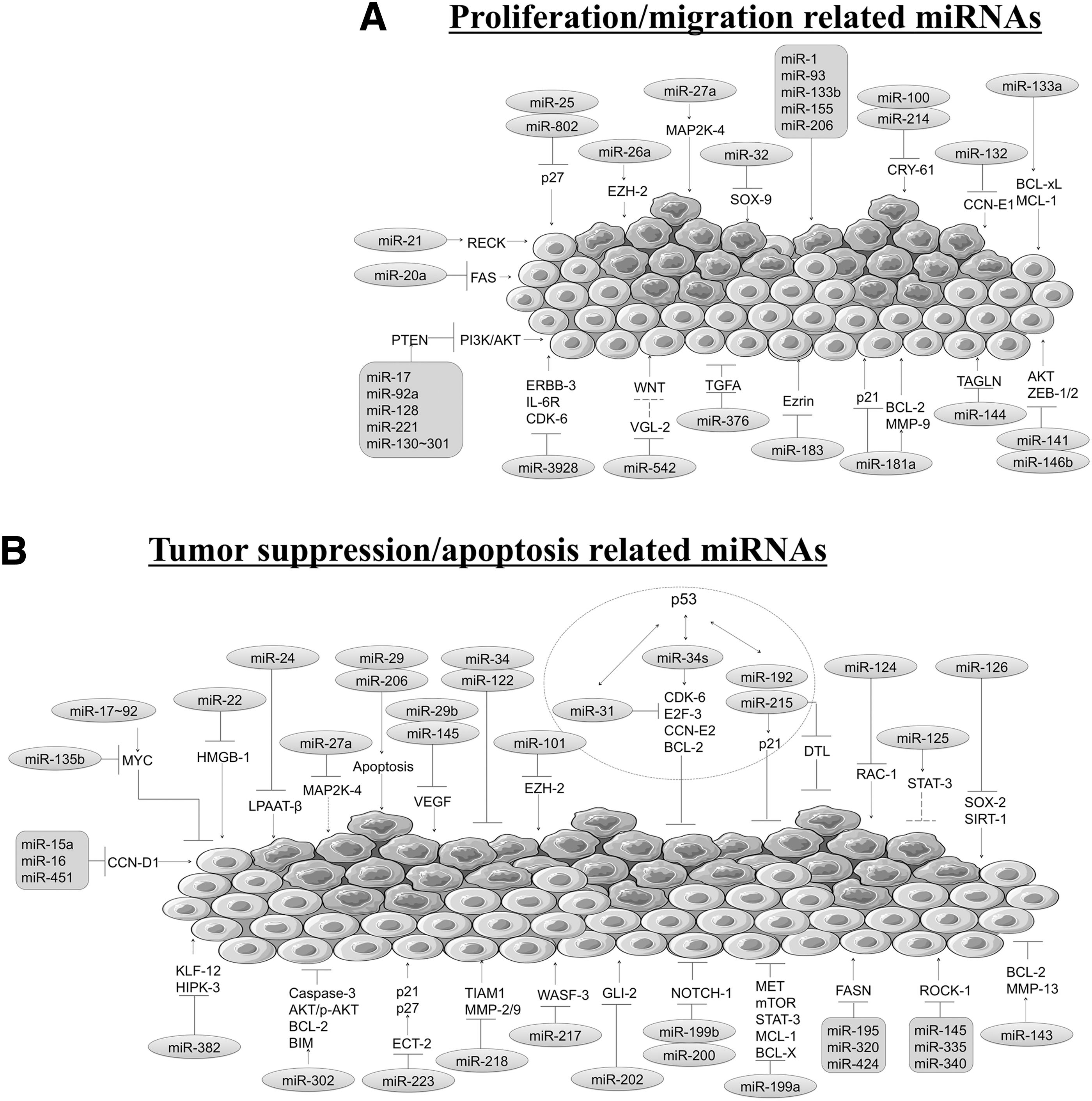
Presentation of miRNAs associated with OS. miRNAs either related to proliferation/migration
One pathway important for OS development, including proliferation, differentiation, survival, and death is the PI3K/AKT pathway. PTEN is known to negatively regulate AKT and thus the PI3K/AKT pathway. This is induced by several miRNAs. Altered expression of PTEN is associated with OS development [152]. For example, miR-17—normally higher expressed in OS cells and tissue—supported cell proliferation, migration, and invasion of OS cells by negatively regulating PTEN [153]. Also miR-92a and the miR-130 ∼ 301 were shown to target PTEN [154]. Shen et al. detected miR-128 significantly increased in OS tissues. Its overexpression significantly promoted proliferation of MG63 and U2OS cells by directly regulating the PTEN/AKT signaling interaction [155]. Higher expression of miR-221 in OS led to an induced cell survival, decreased cell apoptosis, and cisplatin resistance by targeting PTEN [156].
Moreover, FAS (CD95), as a member of the TNF family, is widely expressed in many different cell types. If the FAS ligand in FAS-positive targets binds to FAS, an induced apoptosis results [157]. An overexpression of miR-20a resulted in less FAS expression in SAOS cells contributing by altering the phenotype to the metastatic potential of OS cells [158].
miR-21 could be identified to support cell invasion and migration in OS by targeting RECK [159]. Furthermore, a higher expression of miR-21 is associated with an advanced Enneking stage (classification system) of the patients [160,161]. Cell proliferation and tumor growth in a xenograft mouse model was promoted by miR-25 targeting p27 [162]. The same is described for miR-802 [163]. With the lower expression of miR-26a targeting EZH-2, an increased tumor aggressiveness and tumor metastasis development were detectable [164]. miR-27a could be identified to function as an oncogene by targeting MAP2K-4 in the OS MG63 cell line [165]. miR-32, which is lower expressed in OS tissue, promotes cell proliferation in SAOS, and U2OS cells by negatively regulating SOX-9 [166]. Members of the integrin αV family are involved in tumor angiogenesis and metastasis. miR-548 can directly target the 3′-UTR of this gene family and be a potential therapeutic target. During OS, the expression of miR-548 is downregulated [167].
For some miRNAs, no target in OS cells was identified yet. For instance, miR-1 and miR-133b are both lower expressed in U2OS cells and were associated with high cell proliferation, decreased apoptotic fraction, a positively regulated MET protein expression, cell invasiveness, and motility [168,169]. Montanini et al. identified miR-93 to increase cell proliferation and invasiveness [170]. In OS, miR-155 is higher expressed and could be shown to significantly promote cell proliferation, colony formation, migration, and invasion [171]. Furthermore, miR-206, usually lower expressed in OS cell line MG63 and OS tissue, is associated with the progress of the clinical stage, metastasis development, T classification, and poor histological differentiation [172].
CRY-61, a growth factor associated with extracellular matrix, was negatively regulated by miR-100 [173]. The same gene-regulating abilities were shown for miR-214 [174]. In OS tissues, Wang et al. identified a significant lower expression of miR-132. By overexpression of miR-132, the cell proliferation in vitro and tumor growth in vivo were suppressed by targeting the CCN-E1 [175]. Further loss of microRNA-132 predicts poor prognosis in patients with OS [176]. Decrease of miR-133a in OS cells and tissue was significantly correlated with tumor progression and prognosis of OS patients by targeting B-cell lymphoma (BCL)-xL and MCL-1 [177].
miR-141, belonging to the miR-200 family, is less expressed in OS tissue, U2OS, SAOS, and MG63 cells. Its overexpression inhibits OS cell proliferation and induces cell apoptosis by targeting AKT and ZEB-1/2 [178]. The same targets were described for miR-146b [179]. By downregulating TAGLN, miR-144 was identified to regulate OS cell proliferation and invasion [180].
Viability, proliferation, and invasive abilities of MG63 cells were improved, and apoptosis was inhibited by overexpression of miR-181a by upregulating BCL-2 and MMP-9 and downregulating the tissue inhibitors MMP-3 and p21 [181]. miR-18, which is normally low expressed in human high metastatic carcinoma and colorectal cancer, acts through the repression of Ezrin, a protein associated with the metastatic potential of tumors [182]. miR-376c expression levels decreased in OS tissues and cell lines are associated with cell proliferation and invasion by negatively targeting TGFA [183]. By using a dual luciferase assay and western blot, Li et al. identified the noncanonical Wnt pathway suppressor VGL-2 as a target of miR-542-3p. The higher expression of miR-542-3p enhanced cell proliferation and migration ability of U2OS cells [161]. Lower expression of miR-3928 enhanced tumor growth by targeting the genes ERBB-3, IL-6R, and CDK-6 [184].
Tumor suppression/apoptosis-related miRNAs
Tumor suppression takes place through repressive effects on the regulation of the cell cycle and/or by promoting apoptosis. Several miRNAs are described to be involved in the tumor/migration suppression (Fig. 3B). For example, miR-15a and miR-16, which are lower expressed or not detectable in most cancer diseases, inhibit the CCN-D1 gene in vitro. This regulation induced apoptosis and cell cycle arrest as well as slower proliferation curves of OS cells [185]. Through modulating the expression of PGE-2 and CCN-D1 miR-45 overexpression also inhibited cell proliferation resulting in cell apoptosis [186].
The miR-17 ∼ 92 cluster induced apoptosis by targeting MYC [187]. The same regulating mechanisms were found for miR-135b [188]. miR-22 overexpression inhibited the HMGB-1-mediated autophagy during chemotherapy in OS cells, leading to an inhibition of cell proliferation, migration, and invasion [189]. By targeting LPAAT-β miR-24 inhibited OS cell proliferation [190]. An inhibition of miR-27a led to a higher MAP2K-4 expression, which in turn inhibited cell proliferation and migration through the JNK/p38 signaling pathway [165].
Apoptosis of OS cells is induced by miR-29a and miR-206 [172,191]. Overexpression of miR-29b suppressed cell proliferation, migration, invasion, and could induce apoptosis by directly targeting vascular endothelial growth factor [192]. The same is described for miR-145 [193]. Overexpression of miR-34 and miR-122 initiated apoptosis in cells and reduces the growth of OS xenografts in vivo [194]. Overexpression of miR-101 significantly inhibited migration and invasion of OS cells by inhibiting EZH-2 [195].
p53 plays an important role in DNA repair, growth arresting, and initiating apoptosis. These regulatory abilities have established p53 as a tumor suppressor. The miRNAs miR-31, miR-34family, miR-192, and miR-215 have regulatory effects on p53. Lower expression of miR-31 could be detected in several OS cell lines. A loss of miR-31 was associated with defects in the p53 pathway and functions in different types of cancers [196]. The miRNA-34-family target CDK-6, E2F-3, CCN-E2, and BCL-2 partially in a p53-dependent manner. The higher expression of these induced genes led to apoptosis, cell cycle arrest, and senescence [197]. Similar effects on metastasis of breast and skin cancers were identified by Krzeszinski et al., who analyzed miR-34a transgenic mice [138]. Regarding miR-192 and miR-215, regulatory effects on p-53-related cell arrest were also detectable [198].
Furthermore, miR-215 suppressed the cycle-regulated nuclear and centrosome protein DTL leading to G2 arrest resulting in decreased cell proliferation. Thereby, these cells showed an increased chemoresistance [199].
Attenuated cell proliferation, migration, invasion, and induced apoptosis in MG-63 and U2OS were detectable by overexpressing miR-124 targeting RAC-1 in vitro [200]. miR-125b inhibited proliferation and migration by targeting STAT-3 [201]. miR-126 is another tumor suppressor by targeting SOX-2 and SIRT-1. Its overexpression inhibited the cell proliferation, invasion, and migration [202,203]. Shimbo et al. could show a significant reduction of the migration of OS cells by the higher expression of the normally lower expressed miR-143 [204]. Furthermore, overexpression of miR-143 reduced cell viability and promoted apoptosis by targeting BCL-2 [205]. By targeting MMP-13, miR-143 could also be identified to inhibit pulmonary metastasis development [206].
In cancer, ROCK-1 is known to play a central role in angiogenesis, cell motility, and metastasis [207]. Several miRNAs have an inhibiting effect on ROCK-1. For example, miR-335 that is regularly lower expressed in OS cells and tissue, significantly inhibited after overexpression cell proliferation, migration, invasion, tumor growth, and metastasis by downregulating ROCK-1 [208]. ROCK-1 is also less expressed by miR-145 and miR-340 [209,210].
Fatty acids (FASN) display high expression levels in a variety of human tumors [211 –214]. They count as a novel promising target for the anticancer therapy, because of their sustaining effect on the biological features of cancer cells. Furthermore, FASN may also influence cell metastasis. With the inhibition of the FASN expression in vitro and in vivo, a suppressive effect of the cell proliferation could be shown [215 –219]. Higher expression of miR-195 significantly inhibited FASN synthesis, decreasing migration and the invasion of U2OS cells [220]. Also, miR-320 and miR-424 are targeting FASN. Overexpression of both miRNAs led to the inhibition of cell proliferation [221,222].
Compared with normal tissues, miR-199a-3p, identified by Duan et al., suppressed the cell proliferation and migration by targeting MET, mTOR, STAT-3, MCL-1, and BCL-X by overexpression [223]. Inhibition of cell proliferation through NOTCH-1 was shown by analyzing miR-199b-5p and miR-200 [224,225]. miR-202 suppressed proliferation and induced apoptosis of OS cells by inhibiting the oncogene GLI-2 [226].
By targeting WASF-3, an overexpression of miR-217 functioned as a tumor-suppressive miRNA and inhibited the tumor genesis [227]. miR-218, detected by Jin et al., showed tumor suppression abilities in OS cells by downregulating TIAM-1, MMP-2, and MMP-9 [228]. miR-223, which is lower expressed in OS, inhibited the proliferation by arresting the cell cycle progression in G1 phase after overexpression. Bimolecular studies indicated that the gene expression of ECT-2 was directly inhibited by miR-223, leading to higher expression of p21 and p27, both involved in the G1 block [229]. miR-302b was found to inhibit cell proliferation, promote cell apoptosis, and cell cycle arrest by activating caspase-3 and regulate the AKT/p-AKT, BCL-2, and BIM expression [230]. Overexpression of miR-382 inhibited cell growth and chemoresistance by targeting KLF-12 and HIPK-3, respectively [231].
Chemoresistant/drug-response-influencing miRNAs
The effectiveness of cytotoxic drugs in malignant tumors is limited by the development of chemoresistance. This is particularly true for OS, which is characterized by the frequent refractoriness to chemotherapy. Chemoresistance in OS is regulated by several miRNAs. For example, miR-21 is higher expressed in OS cells and supported chemoresistance [160]. A higher expression of miR-33 was detected in chemotherapy-resistant OS cells. A negative correlation with TWIST was detected, which enhanced cisplatin-induced OS cell apoptosis by inhibiting multiple signaling pathways [232]. miR-140 was shown to increase chemoresistance to methotrexate (MTX) and 5-FU by targeting HDAC-4 [233]. Also, miR-215 improved resistance of OS cells against MTX by targeting DTL [199]. The native higher expression of miR-221 in OS cells went along with a decreased responsiveness to cisplatin [156].
Besides chemoresistance, the knowledge of good against poor responders in tumor therapy is also of high interest. In this context, Gougelet et al. could identify the miRNAs miR-92a, miR-99a, miR-193a-5p, and miR-422a to discriminate between good and poor responders using ifosfamide [234]. Furthermore, a decreased expression of miR-382 was detected in specimens of OS patients with a poor compared with those with a good chemoresponse [231].
Discussion
In the last decade, miRNAs have attracted the attention of scientists because of their regulatory character and physiological functions. It became evident that miRNAs convey a novel and efficient means for gene regulation and expression. In many physiological and pathophysiological processes, miRNAs have been demonstrated to play crucial roles [235]. Interestingly, one miRNA may have different targets. These distinct targets may be within the same pathway or even integrate effects between different pathways. These actions help to fine tune protein levels.
The identification of the regulative pathways of these miRNAs may be the key for innovative new therapeutic approaches. To try to facilitate the understanding of possible involvement in certain pathways, we have tried to group the miRNAs in the different diseases according to important targets found in the literature (Fig. 4). Thus, by describing effects on, for example, osteogenic gene-related mRNAs, possible roles in osteoporosis may be explained. Moreover, same miRNAs may also be found in transcription factor inhibiting pathways. Again, this shows the spectrum of targets for miRNAs. Furthermore, the analysis of freely circulating miRNAs is of interest in view of new diagnostic methods. Worldwide, almost 200 clinical trials based on the regulation of miRNAs to treat several diseases exist, such as cancer or cardiovascular diseases. However, none of these focused on central skeletal diseases (
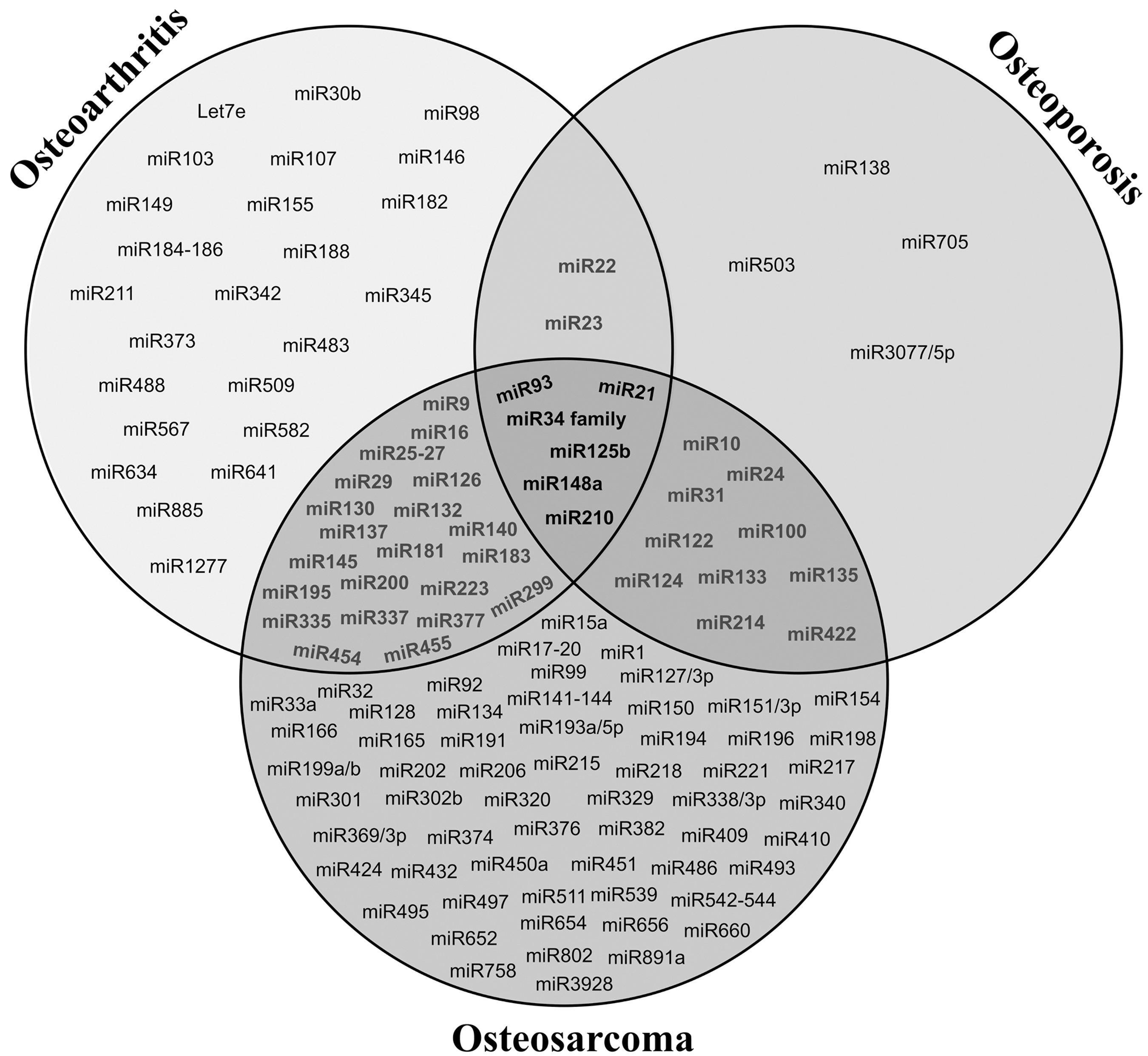
Summary of differentially expressed miRNA in OA, osteoporosis, and OS. Overlapping fields indicate the miRNAs that have been associated to two of these pathologies. In the center of the figure, six miRNAs are highlighted with different expressions that have been detected in these three musculoskeletal diseases.
Profound effects could be evaluated on skeletal disorder-related gene expressions by the inhibition or overexpression of specific miRNAs. For therapeutic approaches, silencing of miRNAs in vivo with “antagomirs” is of high interest, because of its specificity, efficiency, and long-lasting effect [236]. Additionally, Elmen et al. could prove that systematic administration of “antagomirs” modified with locked nucleic acids function without toxicity in nonhuman primates [237]. Advanced developments of combined therapeutics, for example, miRNAs with specific antibodies, may be a high-end solution for delivering the drug directly to the bone, cartilage, or tumor. Besides the therapeutic approaches, the identification of specific circulating miRNAs in physiological and pathophysiological skeletal diseases opens new opportunities for diagnostic means.
miRNAs may also mediate risk factors for skeletal diseases. Most of the miRNAs identified in osteoporosis and OA display the contrary regulation in comparison to the miRNAs found in OS. Furthermore, miR-138, miR-503, miR-705, and miR-3077 were unique for osteoporosis and so far neither detectable in OA and OS. The same was found for the miRNAs let-7e, miR-27b, miR-30b, miR-98, miR-103, miR-107, miR-146, miR-149, miR-155, miR-182, miR-184, miR-185, miR-186, miR-188, miR-211, miR-342, miR-345, miR-373, miR-483, miR-488, miR-509, miR-567, miR-582, miR-634, miR-885, and miR-1277 in OA.
These unique miRNAs may offer useful targets for the development of new diagnostic methods. It is clear that an overlap exists of certain miRNAs in the diseases. Interestingly, most overlap existed not only between OA and OS, but also between OS and osteoporosis. Some miRNAs can be found differentially expressed in all three skeletal diseases. These miRNAs may not be the correct ones for use in diagnostics. Only the ones that are solely expressed in one disease may be useful. However, it may also be that a certain panel constitution has predictive value for a certain disease. This may be especially true when differences in expression, that is, in one disease higher in the other lower expression, exist. For some miRNAs, relationships with certain musculoskeletal diseases have been shown several times, for others this was only in one article. The latter ones need further validation.
Regarding the regulatory effects, several miRNAs were involved in OA, osteoporosis, and OS triggering different targets. For example, miR-21 that was higher expressed in all three diseases could support the chondrogenic differentiation and inhibit osteoclastogenesis and OS cell invasion and migration by inhibiting it. Higher miR-9 expressions were detectable in OA and OS. By downregulating this miRNA, an improved aggrecan development, chondrogenesis, and an inhibition of osteoclastogenensis could be realized. miR-27a that was higher expressed in OA and OS, led to a better collagen production and inhibition of tumor progress.
The miR-34 family differently regulated in OA, osteoporosis, and OS could support the cartilage regeneration and osteoblast development and suppress osteoclast differentiation and OS tumor process through increasing its expression. miR-140, which is differently regulated in OA and OS, is involved in cartilage degrading, osteoclast differentiation, and supports chemoresistance. miR-145, differently regulated in OA and OS, showed a positive effect on cartilage development, chondrogenic and osteogenic differentiation, and angiogenesis by being lower expressed. miR-146 is lower expressed in OA and led to higher collagen deposits, a better osteogenesis, and to an inhibition of osteoclastogenesis and OS cell proliferation by higher expression. miR-148 on the other hand is lower expressed in OA and higher expressed in osteoporosis, and OS could improve collagen production and chondrogenesis and inhibit osteoclastogenensis by upregulating this miRNA.
Another interesting miRNA is miR-155, as it is involved in cartilage degrading, osteoblast and osteoclast development, as well as in the proliferation of OS cells. In OS, there is a higher expression of miR-221 and after its inhibition, there is an improved chondrogenesis, osteogenesis, and OS cell apoptosis. Finally, miR-223 is higher expressed in OA and lower expressed in OS and could inhibit osteoclastogenesis and OS tumor progress after inducing higher expression. These regulating effects of specific miRNAs could be very valuable for the development of new therapeutic approaches for the different diseases. Of course, further direct analytic approaches of all related cells are necessary.
Conclusions and Perspectives
The literature describes specific miRNAs for different skeletal diseases. Some miRNAs are differentially expressed in all three musculoskeletal diseases investigated, but also individually regulated miRNAs for each disease exist. This knowledge can be used to try to develop new diagnostic means for the diseases discussed in the article. Several questions remain regarding the network (targets) of the mRNAs influenced by the miRNAs, the kinetics of miRNAs’ expression, and the widespread influence of miRNAs on various organs in the body. This makes the miRNA interesting as possible therapeutic targets. Answering these questions will not be trivial, but could be solved in the future.
Footnotes
Acknowledgments
The authors would like to thank Fritz Seidl, MBA, MA (translating and interpreting) for proofreading this article. The authors would like to thank Servier for providing the graphics used for the figures.
Author Disclosure Statement
No competing financial interests exist.