
Abstract
There is great demand for transplant kidneys for the treatment of end-stage kidney disease patients. To expand the donor pool, organs from older and comorbid brain death donors, so-called expanded criteria donors (ECD), as well as donation after circulatory death donors, are considered for transplantation. However, the quality of these organs may be inferior to standard donor organs. A major issue affecting graft function and survival is ischemia/reperfusion injury, which particularly affects kidneys from deceased donors. The development of hypothermic machine perfusion has been introduced in kidney transplantation as a preservation technique and has improved outcomes in ECD and marginal organs compared to static cold storage. Normothermic machine perfusion (NMP) is the most recent evolution of perfusion technology and allows assessment of the donor organ before transplantation. The possibility to control the content of the perfusion fluid offers opportunities for damage control and reparative therapies during machine perfusion. Mesenchymal stromal cells (MSC) have been demonstrated to possess potent regenerative properties via the release of paracrine effectors. The combination of NMP and MSC administration at the same time is a promising procedure in the field of transplantation. Therefore, the MePEP consortium has been created to study this novel modality of treatment in preparation for human trials. MePEP aims to assess the therapeutic effects of MSC administered ex vivo by NMP in the mechanisms of injury and repair in a porcine kidney autotransplantation model.
Introduction
K
This situation has resulted in the extension of the minimal criteria required for a person to be a potential donor regarding age and health conditions [3], as well as a more widespread use of donation after circulatory death (DCD) organs. A donor is classified as expanded criteria donor (ECD) by being older than 60 years or older than 50 years and suffering from two out of these three: hypertension, having a cerebrovascular cause of death, and a serum creatinine concentration above 1.5 mg/dL at the time of organ donation [4]. Thus, more kidneys will be used for transplantation, thereby reducing the time people have to wait for a kidney, but at the cost of a higher risk of primary nonfunction (PNF) and delayed graft function, as well as inferior graft function and graft survival.
Increase in Available Kidneys, Decrease in Quality
Organs from circulatory death donors are increasingly considered for transplantation. DCD organs have a prolonged period of warm ischemia before retrieval and higher risk of PNF and poorer organ quality. Delayed graft function defined as need of dialysis occurs in 24% of the transplant recipients in standard criteria donation (SCD). Delayed graft function in DCD donors has been reported in up to 52% of the recipients [5] and for ECD it is 70% higher than in SCD donors [6]. Primarily, organs from brain death donors are used for transplantation. Brain death induces a massive release of inflammatory cytokines such as tumor necrosis factor (TNF)-α and interleukin (IL)-6 in the potential donor [7], which is associated with an elevated risk of delayed graft function [8,9]. Donation after brain death is correlated with more rejection and inferior graft survival [10,11], whereas delayed graft function is similar to DCD donation [12]. Despite increasing the number of kidneys available for transplantation, ECD organs have been shown to have a poorer outcome when compared to standard criteria transplantation [13,14]. Graft function from ECD has been proven to be inferior to kidneys from standard donors [3,6] and combined with lower graft survival this may explain inferior patient survival.
Ischemia/Reperfusion Injury
An inherent problem of organ transplantation regardless of the type of donor is ischemia/reperfusion injury (IRI). During ischemia, the lack of nutrients causes metabolic disruption. Lack of oxygen supply stops aerobic metabolism and leads to accumulation of waste products resulting in a toxic environment. The reactivation of cells at the time of reperfusion is accompanied by the formation of reactive oxygen species and an inflammatory response in the organ [15], which is a primary cause of acute kidney injury (AKI) [16]. Both ischemia time and reperfusion can be optimized to reduce oxidative damage and inflammatory response and hence improve organ quality.
Toward Improving Kidney Transplantation Outcome
Since ischemia is a major cause of inflammation, new strategies have arisen to improve preservation techniques and reduce the time that organs are starved of nutrients and oxygen. Machine perfusion of donor organs is an alternative to static cold storage, which has been the standard method for preserving organs so far. Machine perfusion involves connecting the kidney to a circuit that will pump and recirculate a perfusion fluid. Machine perfusion can be carried out at different temperatures and settings. Hypothermic machine perfusion (HMP) has been demonstrated to improve the outcome of renal transplantation [17,18]. Normothermic machine perfusion (NMP) has the advantage that kidney function can be assessed during preservation before transplantation [19]. Currently, several perfusion conditions are being tested to achieve the best possible outcome such as different temperatures, perfusion characteristics, or fluid composition.
Hypothermic Machine Perfusion
HMP as an alternative to cold storage has been proven to be effective in improving kidney function in animal models through two main postulated mechanisms: preservation of endothelial function by maintaining the expression of key genes such as eNOS, improving circulation during reperfusion [20] and reducing the activation of caspases, meaning that HMP may have a protective role on cell apoptosis [21]. Human studies have shown that HMP reduces inflammation by decreasing the secretion of inflammatory cytokines and thus decreasing the severity of IRI [22].
Normothermic Machine Perfusion
To further improve the physiological conditions for kidney transplants, NMP has been developed. This technique allows to maintain the metabolic requirements of the organ and reduces the ischemic injury by perfusing it with a fluid at physiological temperature, which is supplemented with nutrients and oxygen. This technique is useful to reduce cold ischemia and, additionally, it offers the possibility of assessing organ viability before transplantation [23]. In the only published clinical series, this procedure has been proven to decrease delayed graft function in kidneys, particularly in ECD organs [23,24].
Introduction of Other Therapies During Machine Perfusion
NMP offers the possibility of monitoring kidney function and perfusion fluid content can be measured permanently in such a way that it is possible to perform metabolic profiling during perfusion [25,26]. This is translated in the possibility to add other therapies such as pharmacologic treatments in a very controlled manner [27 –29]. Drug delivery during machine perfusion has been proven effective in reducing IRI during NMP [30]. Cell therapy is also a very interesting option to be used during ex vivo perfusion. Mesenchymal stromal cells (MSC) have potential for regeneration and interaction with the immune system [31,32] and could be administered before transplantation during NMP.
Mesenchymal Stromal Cells
MSC are adult stem cells with the ability to differentiate into several cellular lineages [33 –35]. They are usually retrieved from bone marrow [36] and adipose tissue [37], but MSC are present in almost every adult tissue [38,39]. They are characterized by their plastic adherence properties, their ability to differentiate toward adipocytes, osteoblasts, and chondroblasts, and the expression of a combination of surface markers, including CD73, CD90, CD105, and a lack of expression of markers of the blood cell lineages and the endothelial cell (EC) marker CD31 [40]. There are subtle differences between MSC from different sources [41 –43], but it is unclear whether these differences impact the therapeutic potential of the cells. In addition, MSC are a heterogeneous cell population and there are indications that specific subsets have superior regenerative and immunomodulatory properties [44,45]. The interest in the use of MSC for therapy is based on the easy expansion of these cells in vitro, their regenerative and immunomodulatory effects, and low immunogenicity. The lack of expression of major histocompatibility complex (MHC) class II and low expression of MHC class I and costimulatory molecules [46] make them poorly recognizable by the immune system. Several studies have demonstrated that MSC derived from bone marrow and adipose tissue are immunosuppressive and suppress alloreactivity [31,32,47].
MSC, therefore, have been tested and proved to possess regenerative and immunomodulatory properties, and results of preclinical studies qualify them as a very promising therapeutic agent [48], although possible detrimental side effects have still not been fully explored.
MSC as Mediators of Healing
MSC interact with injured tissue and cells of the immune system in multiple ways. MSC have been shown to locally release a wide variety of growth factors and immunomodulatory cytokines, which change the microenvironment at sites of injury [49] affecting the immune response and tissue regeneration [50 –53]. However, this secretory capacity seems to be not enough [54] as direct physical interaction is needed for MSC to be able to exert their effects [55].
MSC have been shown to be able to adapt to their microenvironment, altering their behavior and secretory profile [56]. Their plasticity gives MSC a therapeutic advantage above conventional drugs. For instance, stromal cell-derived factor 1 is secreted by ECs during hypoxic conditions [57] enhancing the recruitment of MSC [57 –60]. As a result of oxygen deprivation, ECs also secrete hepatocyte growth factor (HGF) [61], which has been shown to increase EC growth [62] and stimulates MSC migration [63]. MSC express the HGF receptor c-met allowing MSC homing to the injured endothelium. MSC themselves secrete HGF and via autocrine signaling remain present at the site of injury [63,64].
MSC also help to repair wounds and have antifibrotic effects that avoid the formation of scar tissue [65] via paracrine secretion of proangiogenic factors [66] and increasing keratinocyte and fibroblast migration toward injured tissue [67].
In addition, MSC exert angiogenic effects by secreting a variety of cytokines. Simultaneous release of HGF and vascular endothelial growth factor (VEGF) by MSC has been found to reduce endothelial permeability during inflammation [68] and to enhance angiogenesis [69]. Moreover, vasculature integrity is protected through angiopoietin-1 interaction with EC [70], while thrombospondin-1 protects platelet-derived growth factor from degradation and therefore enhances angiogenesis [71]. Matrix metalloproteases (MMP) are released under inflammatory conditions [72] and degrade collagen extracellular matrix. MSC inhibit MMP-related tissue disruption by releasing tissue inhibitor of metalloproteases, binding to MMP in a competitive manner and maintaining matrix structure [73].
In addition to their tissue protective and regenerative effects, MSC are potent mediators in reversing inflammatory processes. Several of the immunoregulatory effects of MSC are potentiated under inflammatory conditions. Expression of inhibitory molecules such as programmed death-ligand 1 on MSC membranes suppresses immune cell activation and proliferation [74,75]. Proinflammatory macrophage activation is inhibited via secretion of TNF-α-stimulated gene/protein 6 (TSG-6) by MSC, which at the same time prevents TNF-α secretion from macrophages and reduces inflammation [65]. Furthermore, prostaglandin E2 (PGE2) induces M1 to M2 macrophage metabolic shift [76], which has been shown to prevent tubular damage produced by AKI [77]. At the same time, PGE2 induces Th2 lymphocyte formation [78] and regulatory T cell proliferation [79,80]. Moreover, MSC inhibit effector T cell proliferation [31,81,82] by depleting the tryptophan from the medium as a result of indoleamine 2, 3-dioxygenase (IDO) secretion [82 –84].
MSC function is also based on cell-to-cell interaction. Mesenchymal and EC interaction at injured tissue is well documented [85]. Furthermore, cross talk between MSC and immune cells impairs their homing [86,87] and proliferation [88]. In addition to the secretion of soluble mediators, MSC express a range of cell surface molecules that enable them to interact with immune and tissue cells. MSC express very late antigen (VLA-4), and therefore, they can bind to EC via vascular cell adhesion molecule (VCAM-1) and P-selectin on the surface of EC [89,90].
Thus, the concerted action of soluble and membrane-bound molecules is responsible for the tissue protective and immunoregulatory effects of MSC.
MSC in Kidney Injury Animal Models
MSC therapy has the potential to limit IRI-induced damage, to stimulate regenerative activity in the kidney. Multiple studies have tried to prove the beneficial effect of MSC on tissue injury and inflammation in animal models with very promising results. Posttransplantation immune system modulation and IRI-induced AKI animal models have been developed to test the effect of MSC therapy. In a renal allograft transplantation model in rat, intra-arterial MSC injection resulted in improved early kidney function, reduction of lymphocyte infiltration, and decreased inflammation-related gene expression [91]. MSC have been shown to reduce infiltration of immune cells in the kidney after MSC infusion in rats [92,93], and they were also able to prevent renal fibrosis interacting with the renin–angiotensin system [94].
In large animal models, it has been found that administration of MSC improves kidney function after transplantation, restoring the glomerular filtration rate and decreasing tissue inflammation [95,96]. In a renal injury porcine model, administration of MSC resulted in a decreased kidney concentration of TNF-α and IL-1β and restoration of IL-10 levels [95] (Fig. 1). In a cisplatin-induced AKI rhesus monkey model, MSC infusion through the renal artery seemed to improve renal function and decrease serum creatinine concentration [96].
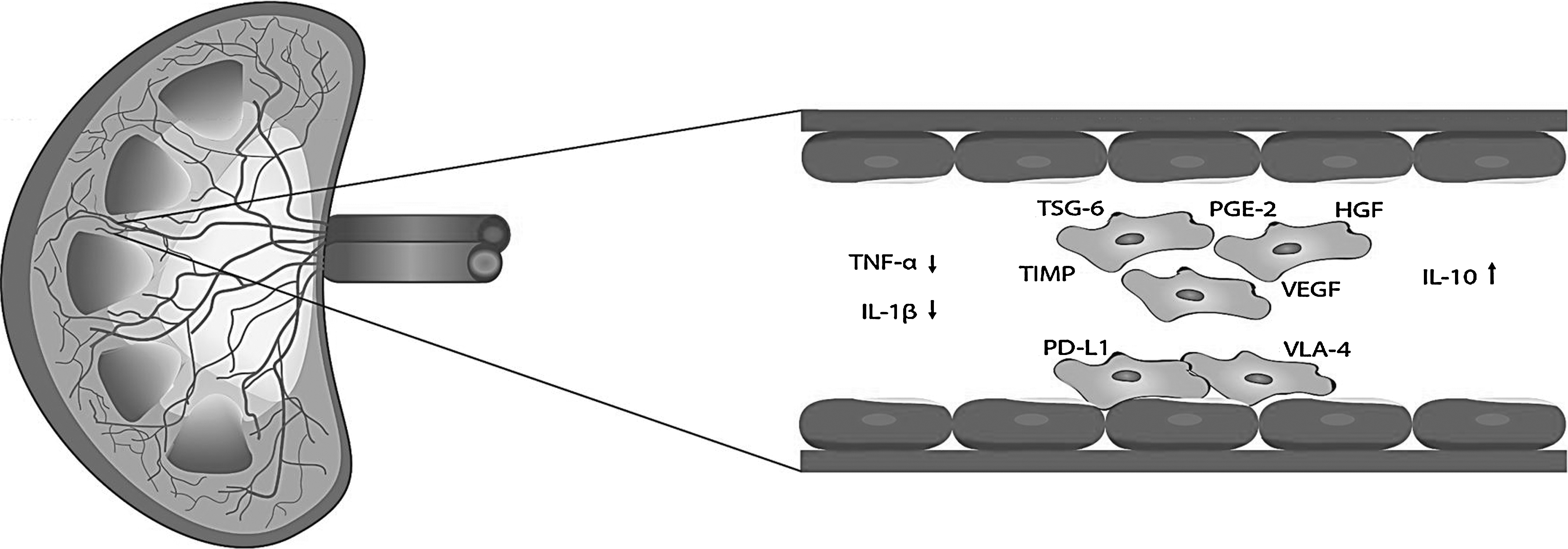
Interaction of MSC with the endothelium. The endothelial cells of the microvasculature of the kidney are the first cells MSC encounter after administration via the renal artery. MSC release a wide variety of anti-inflammatory and regenerative factors, which may interact with endothelial cells by reducing inflammatory responses and stimulate regenerative responses. Molecules present on the membrane of MSC such as PD-L1 and VLA-4 may provide further reparative signals to the endothelium. MSC, mesenchymal stromal cells; PD-L1, programmed death-ligand 1; VLA-4, very late antigen.
Clinical Use of MSC in Kidney Transplantation
The encouraging results from preclinical studies have led to test the safety of MSC therapy as treatment for several conditions [97 –99]. Hence, a number of small clinical trials have studied the feasibility and effects of MSC therapy focusing on kidney transplant recipients. In these studies, MSC administered via intravenous infusion showed no deleterious effects on graft or patient survival [31,100,101]. Furthermore, there are indications that MSC treatment modulated the immune response of these patients. This has led to the presumption that the use of MSC might allow reduction of immunosuppressive drugs without elevating the incidence of rejection [100].
In the field of kidney transplantation, MSC therapy has also been used to reduce the dose of immunosuppressive drugs [102], to regenerate the graft [103] and to modulate the allo-immune response [101,104]. However, the administration of MSC as treatment for kidney transplant recipients via intravenous infusion has some practical limitations. Intravenously administered MSC are trapped in the microcapillaries of the lungs, are not capable of migrating toward injured kidneys [55,105], and may at least theoretically cause pulmonary embolism [106]. Targeted administration of MSC into the kidney in an ex vivo organ perfusion system circumvents the lung barrier and offers the possibility to bring MSC in direct contact with injured kidney cells, allowing localized delivery and optimizing the effect of the cells. Targeted delivery in the kidney furthermore offers the possibility to achieve therapeutic effects with relatively low numbers of cells.
Mesenchymal Stem Cells in Normothermic Ex Vivo Perfusion in Pigs: The MePEP Project
MSC therapy has the potential to limit IRI-induced damage, to stimulate regenerative activity in the kidney, and to reduce the use of immunosuppressive drugs in the transplant recipient. Machine perfusion offers the possibility to apply MSC therapy directly to donor kidneys ex vivo and bypass the lung barrier. To investigate the use of MSC for this purpose, an international consortium has been created with the goal of developing a pretransplant therapy based on MSC and NMP to improve the quality of donor kidneys.
Administration of MSC to donor kidneys via machine perfusion (Fig. 2) delivers MSC directly to the injured organ and possibly in direct contact to injured tissue. The addition of MSC to the perfusion fluid may lead to their adherence to the injured endothelium. This may enable them to interact with ECs both physically [107,108] and via cytokine secretion.

Schematic drawing of a kidney connected to a perfusion machine. The renal artery is connected to a pump and also the ureter is cannulated
When donor organs are reperfused, the release of reactive oxygen species occurs, leading to organ damage and inflammation [15,109]. NMP in combination with MSC may potentially attenuate the inflammatory processes and regenerate injured tissue, eventually leading to reduced fibrosis and better patient outcomes with improved graft survival [52,65]. Localized secretion of immunomodulatory effectors may be able to modulate the immune response of the host after transplantation, decreasing rejection and improving early graft function. Studies within the MePEP project will attempt to resuscitate the kidney before transplantation to reduce the severity of IRI and its consequences. In addition, optimal growth conditions and pretreatment of MSC as well as administration of the cells will be studied together with possible side effects in a porcine autotransplantation model.
In summary, the shortage of kidneys for transplantation is leading to the acceptance of lower quality organs for transplantation in an effort to increase the number of transplanted patients and reduce waiting times. The main objective of this research is to develop a procedure based on NMP and MSC to improve the quality of transplanted organs, as well as the reduction of the immune response against the transplanted kidney by the host. If the results from these large animal studies will be favorable, human studies will follow. Ex vivo MSC therapy could eventually lead to more and better donor kidneys for transplantation and an increase in patient and graft survival, with less use of immunosuppressive drugs.
Footnotes
Acknowledgment
The MePEP project is funded by the Lundbeck Foundation under grant application no. R198-2015-184.
Author Disclosure Statement
No competing financial interests exist.