
Abstract
The treatment of myelodysplastic syndromes (MDS) involves improving patient survival and quality of life (QoL) and decreasing the likelihood of progression to AML. Although the treatment outcomes of MDS remain unsatisfactory, few comparative studies have been performed while comparing the outcomes of low-risk and intermediate-risk patients treated with supportive care and chemotherapeutics to those of patients treated with allogeneic hematopoietic stem cell transplantation (allo-HSCT). Therefore, we designed a clinical control study to compare the outcomes of supportive care and chemotherapeutics versus allo-HSCT treatment in MDS patients. A total of 182 patients with MDS were enrolled in the study, including 91 in the no-HSCT (control) group and 91 in the allo-HSCT group. The complete remission (CR) rate in the allo-HSCT group was significantly higher than that in the control group (53.8% vs. 33.0%; P < 0.05). The QoL of patients in the HSCT group was much higher than that in the control group (53.8% vs. 37.4%; P < 0.05). The overall survival (OS) rates were 79.0% and 56.0% (P < 0.05) in the HSCT group and the control group, respectively. In conclusion, a high-dose fludarabine (Flu), busulfan (Bu), cyclophosphamide (CTX)-based conditioning regimen was well tolerated and significantly speeded hematopoietic recovery. In addition, this regimen increased procedure-related toxicity and improved QoL and OS.
Introduction
M
With the improvement of living standards, the treatment of MDS involves not only decreasing the likelihood of progression to AML but also improving patient survival and quality of life (QoL). The recent development of two new drugs, decitabine and azacitidine, has improved the therapeutic efficacy of MDS patients [4 –6]. Although these treatment methods have obtained hematological and cytogenetic responses in a proportion of patients, these therapies are not completely curative [7]. Currently, allogeneic hematopoietic stem cell transplantation (allo-HSCT) remains the only curative treatment for MDS [8].
Cutler et al. [9] showed that patients belonging to high-risk groups according to the International Prognostic Scoring System (IPSS) should be transplanted as soon as possible after diagnosis, whereas patients with low-risk diseases benefit from a wait-and-see approach with regard to allogeneic HSCT. Some scholars [10] think that MDS patients should be transplanted at 3 to 12 months after diagnosis, and the delay in transplantation will increase the recurrence rate and the transplant-related mortality. Nevertheless, few comparative studies have been performed while comparing the outcomes of low-risk and intermediate-risk patients treated with supportive care and chemotherapeutics against those treated with allo-HSCT, so the question of whether allo-HSCT is actually superior to drugs and supportive care in treating low- and intermediate-risk MDS remains unanswered. To clarify the role of allo-HSCT in the treatment of low- and intermediate-risk MDS, we designed a clinical control study to compare the outcomes of supportive care and chemotherapeutics versus allo-HSCT treatment in MDS patients.
Materials and Methods
Study design and patient characteristics
Ethics approval and patients' consent to participate: in accordance with the Helsinki Declaration, all patients consented to the use of their medical information for this research before entering the study. The Southeast University and Suzhou Medical University Ethics Committees consented and gave permission for the study and required participants to sign a written informed consent form.
From September 2008 to December 2015, 182 MDS patients were treated at two transplantation centers. Patients from the Southeast University Zhong Da Hospital Department of Hematology and Hematology Division from Suzhou Medical University participated in this study. The inclusion criteria were as follows: (1) Patient diagnoses were defined by the World Health Organization and French-American-British criteria [11 –13]; (2) IPSS classification was low risk, intermediate-risk 1, or intermediate-risk 2, and patients with high-risk MDS or whose disease had transformed into AML were excluded; (3) chromosomal and immunophenotyping analyses were performed with pretreatment bone marrow obtained at diagnosis; (4) low-risk patients had a platelet count of <20 × 109/L, absolute neutrophil count (ANC) <0.5 × 109/L, and/or hemoglobin <60 g/L, sustained more than 3 months; and (5) patients who had any severe pulmonary, cardiac, liver, renal diseases or any active infection before the study were excluded. On entering the study, patients were randomly assigned to treatment with allo-HSCT or no-HSCT group. Patients were followed until the end of the study evaluation period in March 2016. In accordance with the Helsinki Declaration, all patients consented to the use of their medical information for this research before entering the study. The Southeast University [ZDYJLY-2009 (29)] and Suzhou Medical University [SZLLY-2010 (108)] Ethics Committees approved the study and required participants to sign a written informed consent form. The characteristics of the patients including age, sex, disease duration time, IPPS risk group, and disease status were equivalent in two groups (Table 1).
HSCT, hematopoietic stem cell transplantation; MDS, myelodysplastic syndromes; RAEB, refractory anemia with excess blasts; RARS, refractory anemia with ring sideroblasts; RCMD, refractory cytopenia with multilineage dysplasia; RCUD, refractory cytopenia with unilineage dysplasia.
Treatment design
Arm A: drugs and supportive care
There were 11 low-risk patients who received oral cyclosporine and androgen therapy, 9 intermediate-1 risk patients who received decitabine treatment, 30 intermediate-2 risk patients who received CAG and/or decitabine chemotherapy, 8 patients who received the antithymocyte globulin (ATG) regimen, 3 patients who received lenalidomide treatment, 2 patients who received azacitidine treatment, and 28 patients who received erythropoietin, G-CSF, and transfusion support treatment.
Arm B: allogeneic stem cell transplantation
For donor selection, all donors included in this analysis were HLA matched at A, B, and DR loci. HLA typing was performed by using molecular methods [polymerase chain reaction sequence-specific primer (PCR-SSP), polymerase chain reaction-sequence based typing (PCR-SBT), and DNA sequencing] for all loci (HLA-A, -B, -C, -DR, and -DQ) in unrelated donors. For 91 patients, of whom 13 patients received haploidentical transplants and 53 patients received their allografts from sibling donors, HLA-identical donors were available for 34 patients, donors with one locus mismatched were available for 14 patients, and donors with two loci mismatched were available for five patients. Twenty-five patients were paired with unrelated donors. Unrelated HLA-identical donors were available for 15 patients, donors with a sub-site of incompatibility were available for nine patients, and a donor with two sub-sites of incompatibility was available for one patient. Thirty-nine cases were ABO compatible, and there were 52 cases of blood group incompatibility.
Preparative regimen
Before allo-HSCT, it was recommended that patients only receive short-term eliminate iron therapy for <3 months if the patients relied on blood transfusions and had ferritin levels greater than 1,000 ng/L. The conditioning regimen consisted of fludarabine 30 mg/m2 for 6 days (transplant days −8 to −3) with busulfan (0.8 mg/kg administered every 6 h for a total of 10 to 12 doses, for −6 to −4 days), and cyclophosphamide (1.2 g/m2 daily, for −5 to −4 days; 1.0 g/m2 daily, for −3 to −2 days). All patients received an antithymocyte globulin (ATG Fresenius AG, Oberurse, Germany) at 4 mg/kg daily intravenous. In cases of HLA-mismatched/haploidentical sibling or unrelated donor transplants, ATG was administered for three to four consecutive days; in cases of HLA-matched patients, ATG was administered for two consecutive days (Fig. 1).

Fludarabine (Flu), busulfan (Bu), cyclophosphamide (CTX), and a low-dose antithymocyte globulin (ATG) regimen.
Graft-versus-host disease prophylaxis and supportive care
For unrelated or haploid donor transplants, cyclosporine A (CsA) combined with short-methotrexate (MTX) was given for acute graft-versus-host disease (GVHD) prophylaxis. Cyclosporine (2.5 mg/kg/day) was administered as a continuous 24-h intravenous infusion from day −1 and was continued until patients could tolerate oral medication; CsA was given with a target blood level of 200–400 ng/L and a short course treatment of MTX (15 mg on day 1 and 10 mg on days 3, 6, and 11, respectively). Mycophenolate mofetil (MMF 0.5 g twice a day orally) was started on day −1 and was discontinued on day 30. In sibling-matched donor transplants, cyclosporine was combined with MMF to prevent GVHD, with the same specific use as described earlier.
All patients were hospitalized in rooms with high-efficiency air filters and received standard antibiotic prevention of Pneumocystis carinii disease by oral trimethoprim-sulfamethoxazole. Intravenous ganciclovir (5 mg/kg) was administered twice a day from 8 days before the procedure to 2 days before transplantation. Cytomegalovirus DNA was monitored by PCR once a week. Prostaglan hematodin E1 (20 μg once a day) was administered for prophylactically hepatic veno-occlusive disease. All blood products were irradiated.
Engraftment and chimerism
Engraftment was defined as an ANC of >0.5 × 109/L for the first three consecutive days and a platelet count of >20 × 109/L for at least a week, independent of a transfusion, and was applied in cases of sex-mismatched donor–recipient pairs for whom assessment of donor chimerism was based on fluorescent in situ hybridization for X and Y chromosomes or on cytogenetic analysis. In addition, chimerism was identified with the analysis of short tandem repeat polymorphisms by using PCR technology (STR-PCR) in gender-matched transplantations.
MRD monitoring and definition
Marrow blasts for more than 5% of patients were monitored for MRD post-transplantation according to leukemia-associated immune phenotypes. Immune phenotypes were detected by 8-color flow cytometry (FCM; FACS Calibur; BD Biosciences). FCM positivity was defined as >0.01% of cells with leukemia-associated immune phenotypes in post-transplantation BM samples [14]. Routine MRD monitoring was performed at 3, 6, 9, and 12 months post-transplantation. The tests were repeated 2 weeks after positive FCM or PCR results were detected.
Preemptive IFN-α
Patients with an MRD-positive status were eligible for IFN-α treatment. Recombinant human IFN-α-2a subcutaneous injections (Intveen; Shenyang Sansheng Biotechnology, Shenyang, China) were administered at a dosage of 3 million units two to three times per week, for 3–6 months.
Responses criteria
According to the International Working Group criteria of efficacy, complete remission was defined as the recovery of hematopoiesis, with an ANC >1.5 × 109/L, platelet count >20 × 109/L, Hb >70 g/L, normalization of marrow blasts (5%), and all cell lines with normal maturity, chromosomes, and minimal residual disease reached normal range. Partial remission means that other conditions achieved complete remission criteria, but bone marrow blast cells before treatment decrease were ≥50% and >5% after treatment. Stable disease means that the condition has not met the minimum standards of partial remission for at least 8 weeks, but without evidence of disease progression. Disease progression means that blasts experience a ≥50% increase in underlying value with any of the following: ≥50% decrease when compared with the number of neutrophils or platelets' best mitigation effect, decreased hemoglobin ≥20 g/L, or transfusion dependence.
Evaluation of QoL
The Karnofsky Performance Scale (KPS) index was used to compare the effect of different treatments to evaluate individual prognosis and healthcare needs [15,16]. The European Cancer Research and Treatment Organization's Core Quality of Life Questionnaire [European Organization for Research and Treatment of Cancer Core Quality of Life Questionnaire (EORTC QLQ C30, version 1.0)] is an effective assessment HRQoL tool in cancer patients [17]. All patients were evaluated according to five functional scales (physical, role, emotional, social, and cognitive) and an overall health/global QoL Scale. Patients with higher scores had a better QoL. At the same time, three symptom scales monitored fatigue, pain, nausea, and vomiting; six single items that assessed symptoms commonly reported in cancer patients (dyspnea, sleep disturbance, loss of appetite, diarrhea, constipation, and economic impact) were also monitored. Patients with high scores showed greater symptomatology or impairments. The average scale and item scores were then transformed to a 0 to 100 scale based on the EORTC scoring manual. All patients were evaluated at four time points (baseline and follow-up at 3, 6, and 12 months after hematopoietic stem cell transplant or drugs and supportive care).
Statistical analysis
The primary end points of this study were DFS, overall survival (OS), and disease-related mortality. Univariate analysis was performed for age, sex, presence of cytogenetic abnormalities, percentage of blasts in the BM, presence of comorbidities, IPPS risk group, disease activity, methods of treatment, and time from diagnosis to treatment. OS and progress-free survival (PFS) were calculated by using the Kaplan–Meier method [18], with statistical comparisons completed by using the Log-Rank test and Cox regression for multiple regression analysis [19]. PFS was defined as the time from complete remission to disease progress or death from any cause. OS was defined as the time from stem cell infusion to death from any cause. Measurement data are shown as the mean ± standard deviation and were calculated by using t-test and chi-square analysis data count test (χ 2). All values were two tailed, and p < 0.05 was considered statistically significant. The statistical analyses were performed by using SPSS statistical software package (SPSS 11.5).
Results
A total of 182 patients with MDS were enrolled in the study, including 91 in the no-HSCT group and 91 in the allo-HSCT group. The characteristics of the patients in the two groups are summarized in Table 1. Patient age, sex and subtype, disease status, and risk stage of disease were compared between the two groups. The characteristics of the patients including age, sex, and disease status at treatment were equivalent in the two groups.
Analysis of prognostic factors
Because of some differences between the two groups in terms of their pretreatment characteristics, we analyzed the association of those characteristics with survival. The univariate analysis indicated that status of the disease, treatment regimen, poor chromosomal prognosis, and bone marrow blasts ≥10% influenced the OS. Age, gender, and MDS duration ≥1 year were not identified as risk factors for OS. A multivariable analysis indicated that the most independent predictors for OS were treatment regimen, active disease, bone marrow blasts ≥10%, and poor chromosomal prognosis, with hazard ratios of 3.37, 2.93, 2.26, and 2.68, respectively (Table 2).
CI, confidence interval; HR, hazard ratio with 95% CIs; multivariable analysis, factors with at least borderline statistical significance in the univariant analysis (P < 0.1) were included in a Cox proportional hazard model; multivariate analysis (P < 0.05) reaching the statistical significance; n, number; OS, over survival rate at 4-years.
Response to no-transplant treatment
Ninety-one patients were treated by using no transplant. Thirty patients (33.0%) achieved a CR, 12 patients (13.2%) achieved a partial remission (PR), 7 patients (7.7%) achieved stable disease, and 42 patients (46.1%) showed disease progression. The median follow-up was 48 months (range, 3–108 months) for all no-transplant patients. The 4-year OS rate was 56.0%.
Allo-HSCT
All patients (100%) were engrafted successfully. Twenty-eight (30.8%) of the 91 engrafted patients developed acute graft-versus-host disease (23 with grades I or II and 5 with grades III or IV), and 16 (17.6%) patients developed chronic graft-versus -host disease (13 had limited cases; 3 had extensive cases). Forty-nine patients (53.8%) achieved a CR, 11 patients (12.1%) achieved a PR, 8 patients (8.8%) achieved stable disease, 1 out of 12 patients with an MRD-positive status was eligible for IFN-α treatment, and 7 patients achieved a CR. Twenty-three patients (25.3%) showed disease progression or death.
Opportunistic infections
There were 94 cases of opportunistic infections in the patients during the follow-up period. A total of 28 patients in the no-HSCT group were infected, including four cases of infection that caused respiratory failure and death. A total of 38 patients in the HSCT group were infected, including six patients who died of severe infection. Infection rate was lower in the no-HSCT group than in the control group [30.8% (28 of 91) vs. 41.8% (38 of 91)] after the induction chemotherapy or immune therapy. However, no significant difference in severe infection rates was observed between the two groups [14.3% (4 of 28) vs. 15.8% (6 of 38), respectively; P = 0.763].
Health-related QoL
There were clinically significant differences at baseline in the direction of better QoL in the HSCT group for nine scales and items. The differences in global QoL [78 (range: 70–84) versus 53 (95% confidence interval [CI]: 46–59)] and fatigue [19 (range: 16–33) versus 41 (95% CI: 34–48)] were most significant. Our data suggest that the HSCT patients' physical and social functioning was significantly improved (Table 3). Furthermore, according to the KPS index, in the HSCT group, 19 patients were able to live at home and care for themselves, and 30 patients from this group were able to carry on normal activities with no evidence of disease. In the control group, there were 21 patients who required occasional assistance and were able to care for most of their personal needs, with a KPS of 60. Ten patients were able to care for themselves, but could not carry on normal activities or to do active work; only 34 patients were able to return to work, school, or housework. There was a significant difference in the recovery of function in QoL between the HSCT and control groups (53.8% vs. 37.4%, KPS >80; P < 0.05).
Higher scores indicate better functioning.
Mean (95% CI).
P < 0.01 for differences in mean scores, no-HSCT versus HSCT.
Higher scores indicate more symptomatology.
QoL, quality of life.
Disease progression and survival
With a median follow-up of 46 months (range: 2–82 months), 65 patients showed disease progression after treatment, including 23 patients in the HSCT group and 42 patients in the control group. The ratio of patients with progression-free disease survival was 74.7% versus 53.9% (P < 0.05). The Kaplan–Meier survival curves are shown in Fig. 2. The CR rate in the allo-HSCT group was significantly higher than that in the control group (53.8% vs. 33.0%; P < 0.05). The QOL of patients in the HSCT group was much higher than that in the control group (53.8% vs. 37.4%; P < 0.05). The OS rates were 79.0% and 56.0% (P < 0.05) in the HSCT group and the control group, respectively. Significantly higher proportions of CR, QOL, and OS were found in the allo-HSCT group compared with the control group.
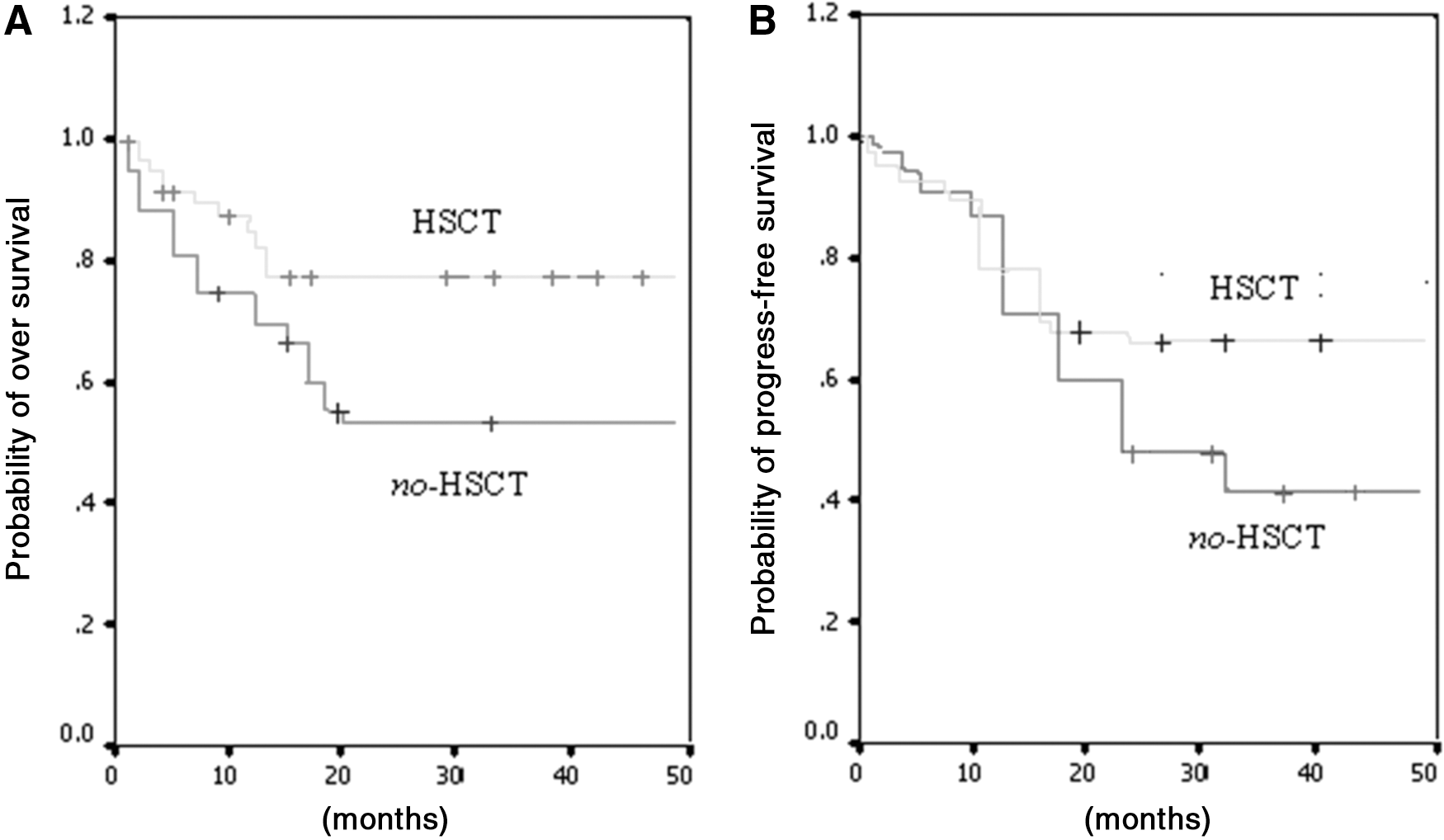
Kaplan–Meier curve estimate of over survival (OS) and progress-free survival (PFS) in patients between the HSCT and no-HSCT groups.
Discussion
Allo-HSCT is a curative treatment modality for myelodysplastic syndrome [20,21]. However, due to the presence of certain risks, selecting the time and conditioning regimen of transplant and deciding which patients actually need transplants are still controversial. The traditional wisdom is that in progressive MDS, transfusion dependence should be transplanted as soon as possible [22]. International MDS Risk Factors of the Working Group realized that intermediate-2 or high-risk patients had a poor prognosis and a high risk of progression to AML, whereas low-risk and intermediate-1 patients have a better prognosis. Some studies have shown that patients less than 60 years of age and patients with intermediate-2 risk and high risk should be treated with allo-HSCT as soon as possible. For patients with low risk and intermediate-1 risk, it is best delay a transplant, but to avoid pretransplant disease progression [9,23]. However, IPSS with defective components is not considered to be clinically severe thrombocytopenia, and although for low-risk patients the chances of transforming into AML are low, they can also lead to death if serious bleeding occurs (especially intracranial hemorrhage); therefore, the prognosis is very poor. The IPSS has been used to stratify MDS patients into different risk groups, whereas the Revised IPSS (IPSS-R) does take into account the extent of cytopenias and would reclassify many low- and intermediate-1 risk patients into intermediate-2 or higher risk categories. On the other hand, some patients with severe anemia must rely on red cell transfusions, which may lead to hemochromatosis and poor QoL. Once medical therapy has proven ineffective, transplants should be performed as soon as possible.
The MDS conditioning regimen is usually a busulfan (Bu), cyclophosphmide (Cy) or fludarabine (Flu), busulfan (Bu) program, as well as a high-dose TBI program. Recently, a number of new programs have been shown to be better tolerated by patients, such as high-dose TBI, reduced busulfan doses, replacing TBI with fludarabine as an immunosuppressant, and the application of anti-thymocyte globulin [24 –26]. In this study, the busulfan, fludarabine, and cyclophosphamide pretreatment program played a better role in immunosuppression. In addition, pretreatment plus a low dose of anti-thymocyte globulin was shown to further enhance the recipient's immune suppression and was conducive to the implantation of donor cells, while reducing the incidence of GVHD and improving the transplant patient's QoL. In this study, out of 91 hematopoietic stem cell transplant patients, none experienced primary implantation failure; although 21 were transfusion dependent and had a high risk of graft rejection, the donor cells were still successfully implanted. Our study has shown that the high-dose fludarabine (Flu), busulfan (Bu), cyclophosphamide (CTX) (FBC) conditioning regimen had no adverse effect on the implantation of the donor cells and reduced early relapse after transplantation. This may be associated with graft versus MDS clone effects, especially when the tumor burden is low [27,28].
Severe GVHD and relapse remains a leading cause of death after transplantation in patients with MDS. In the present study, we investigated whether high-dose conditioning regimen combined with IFN-α may be a potential alternative for MRD-positive patients and reduced the rate of relapse. IFN-α may have an immunomodulatory effect in HSCT recipients, which can induce a GVL effect and clear tumor cells [29,30]. In this study, 5 patients died of severe acute GVHD, 14 patients died of infection, and only 2 patients relapsed after transplantation. In this study, 21 cases of transfusion-dependent patients from MDS-RAS and MDS-RCMD experienced better transplants, suggesting an effective eradication of MDS clones by the high-dose conditioning regimen rapid engraftment of donor hematopoiesis. Only three patients had the limitations of chronic GVHD, and their QoL quickly returned to normal levels. A low relapse rate after a 4-year follow-up period in this study also suggests that a GVL effect can be expected in this conditioning setting.
In the present study, we showed that low-risk and intermediate-1 MDS patients with transfusion dependence should have transplants performed as soon as possible after medical therapy is proven ineffective. An ATG-based high-dose FBC conditioning regimen with interfer-α achieved a higher CR rate than conventional no
Conclusions
A first plausible explanation for these findings is that an ATG-based high-dose FBC conditioning regimen with interfer-α can significantly speed hematopoietic recovery after allo-HSCT in MDS patients, thereby reducing relapse and improving the QOL and OS. We acknowledge that our study involved a limited number of patients with various IPPS risk group diseases treated at two transplantation institutions and that some potential bias in the selection of the treatment regimens may have existed. A larger multicenter prospective trial and the IPSS-R is needed to assess the long-term benefit of a new conditioning regimen in low-risk, intermediate-risk MDS.
Footnotes
Acknowledgments
The authors thank the three transplantation institution staff members, nurse practitioners, and nurses at Hematopoietic Cell Transplantation for their dedication and excellent patient care.
Author Disclosure Statement
Consent for publication: all authors and participants, or in the case of children their parent or legal guardian, consented to publishing this article and were required to sign a written informed consent form.
Competing interests statement: the authors declare that they have no competing interests.
Financial: the sources of the funding body for this study with regard to the design of the study and collection were supported by Key Department of Jiangsu Medicine (2016–12).