
Abstract
Recent studies have indicated that stem cell transplantation may be effective in the treatment of ischemic stroke. Therefore, we performed a meta-analysis to evaluate the safety and efficacy of stem cell therapy for ischemic stroke in preclinical and clinical studies. In accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, we searched the PubMed, Cochrane Library, Embase, Web of science, and Ovid databases from inception through May 2018. A total of 11 preclinical studies—18 independent interventions were ultimately included. Similarly, 11 clinical studies were finally included. Two authors independently screened trials. Lesion volume and modified neurological severity scores (mNSSs) were regarded as outcome measures for preclinical studies. The composite weighted mean [95% confidence interval (CI)] effect sizes for lesion volume, percentage of lesion volume, and mNSSs were −46.59 (−62.04 to −31.15; P < 0.001), −13.18 (−25.62 to −0.73; P = 0.04), and −1.85 (−2.17 to −1.53; P < 0.001), respectively. Our analysis revealed that all three outcomes were significantly more favorable in the stem cell group than in the control group. Barthel index (BI) values, modified Rankin scale (mRS) scores, National Institutes of Health Stroke Scale (NIHSS) scores, and Fugl-Meyer assessment (FMA) scores were regarded as outcome measures for human studies. Our results were as follows: NIHSS [mean differences, MDs = −2.57, 95% CI (−3.45 to −1.68), I 2 = 51%, P < 0.001]; BI [MD = 7.93, 95% CI (3.11 to 12.75), I 2 = 59%, P = 0.001]; mRS [MD = −0.53, 95% CI (−0.73 to −0.28), I 2 = 0%, P < 0.001]; FMA [MD = 5.50, 95% CI (2.05 to 8.95), I 2 = 15%, P = 0.002]. These results suggest that stem cell transplantation was associated with significantly better outcomes than control treatment. Adverse reactions such as mild headache and fever resolved shortly after treatment. Stem cell transplantation can significantly improve neurological deficits and quality of life in patients with ischemic stroke, without severe adverse reactions. Our results also suggest that such treatment is most effective when provided earlier and through the intravenous route.
Introduction
Stroke is one of the leading causes of death and disability worldwide [1]. Clinical treatments in the acute time window have improved [2]. Ischemic stroke affects >50 million people worldwide, with a yearly mortality rate approaching 10%. Moreover, most survivors experience long-term disability, reducing their quality of life and increasing the overall economic burden [3,4].
Currently, intravenous tissue plasminogen activator (t-PA) is the primary reperfusion therapy for acute ischemic stroke (AIS), and its time dependence is a key factor influencing its clinical efficacy [5,6]. However, very few patients with ischemic stroke (<10%) meet the current eligibility criteria for intravenous t-PA, including arrival within a relatively short treatment window (<4.5 h) after the onset of symptoms [5,7]. Meretoja et al. [8] demonstrated that a few minutes saved in delivering intravenous t-PA translates to significant benefits equivalent to days, weeks, and even months of disability-free life over the patient's lifetime.
Mechanical thrombectomy is advantageous in that it can extend the therapeutic time window [9]. In fact, an advance in acute stroke treatment since 2014 is the demonstration in several trials that thrombectomy with stent retrievers for recanalizing intracranial large vessel occlusion (LVO) improves both recanalization and long-term outcomes in several trials [10]. However, with the current evidence, AIS due to occlusion of a large vessel in the anterior circulation can undergo catheter-based intervention with a stent retriever only if they meet relevant criteria [10].
The DAWN and DEFUSE-3 trials demonstrated the benefit of endovascular thrombectomy (ET) in late-presenting AIS due to anterior circulation LVO [11]. Interestingly, recent studies have suggested performing catheter-based interventions in each patient with LVO. Desai et al. [11] indicated that trial ineligible patients with LVO strokes receiving off-label ET achieved outcomes comparable with DAWN and DEFUSE-3 eligible patients. Their research team pointed that a larger population of patients can potentially benefit from ET in the expanded time window if more permissive criteria are applied. Similarly, Desai et al. [12] suggested that ET appears to be safe and feasible in patients with AIS due to LVO meeting all DAWN trial criteria but treated beyond 24 h of time last known well.
Recent evidence suggests that stem cell therapy may be effective in patients with neurological deficits. Such studies have demonstrated that stem cell transplantation can lead to functional improvement in animal models of ischemic stroke. Beginning in 2005, Bang and colleagues [13] initiated several clinical trials of stem cell therapy in patients with stroke, investigating the therapeutic potential of mesenchymal stem cells. Their findings suggested that stem cell therapy is feasible, safe, and can promote recovery in patients with ischemic stroke. However, stem cell transplantation has not been fully evaluated for the treatment of ischemic stroke in clinical settings. Therefore, in this study, we performed a meta-analysis of the available data to evaluate the safety and efficacy of stem cell therapy for ischemic stroke.
Materials and Methods
Preclinical research methods
Search strategy
The present meta-analysis was performed in accordance with the guidelines outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [14]. For the full PRISMA checklist, see Table 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses Checklist for Minimum Set of Items for Reporting in Systematic Reviews and Meta-Analysis
CI, confidence interval; M, manuscript; PICOS, participants, interventions, comparisons, outcomes, and study design.
We searched for studies regarding stem cell transplantation in animal models using the PubMed, Web of Science, Embase, and Ovid databases. The following search strategy was used (take PubMed, for instance): “strokes” or “ischemic stroke” or “cerebral infarct*” or cerebrovascular accident?” or “cerebrovascular apoplexy” or “apoplexy” or “brain vascular accident?” or “cerebrovascular stroke” or “ischaemic stroke” or “ischemia stroke”; “stem cell” or “bone marrow mesenchymal stem cells” or “umbilical cord blood stem cells” or “cord blood stem cells” or “neural stem cells” or “human embryonic stem cells” or “embryonic stem cells” or “induced pluripotent stem cells” or “peripheral blood stem cells”; “transplantation”; and #1 and #2 and #3 (filters: “randomized controlled trial” (RCT)).
Inclusion and exclusion criteria
We included randomized controlled trials (RCTs) that investigated the effect of stem cell therapy on stroke repair in animal models as determined based on the volume of the ischemic lesion or functional outcomes [ie, modified neurological severity scores (mNSSs)]. All included RCTs utilized either a placebo group or a sham-operated control group. Studies involving all types of stem cells were included. However, we excluded literature reviews, meta-analyses, meeting abstracts, and case reports. We also excluded studies in which the grouping method was ambiguous or whose raw data could not be transformed.
Data extraction
Two authors independently screened the literature according to the inclusion and exclusion criteria, extracted the data, and assessed the methodological quality of the studies. The quality score of each preclinical study was determined in accordance with the scale developed by Lees et al. [15], which includes 10 criteria based on the Stroke Therapy Academic Industry Roundtable (STAIR) guidelines [16,17]: (1) publication in a peer-reviewed journal, (2) statements describing control of temperature, (3) random assignment of animals to treatment group, (4) allocation concealment, (5) blinded outcome assessment, (6) avoidance of anesthetics with known marked intrinsic neuroprotective properties, (7) use of animals with relevant comorbidities, (8) inclusion of a sample-size calculation, (9) statement of compliance with animal welfare regulations, and (10) inclusion of a statement declaring the presence or absence of any conflicts of interest. One point was given for each criterion reported. Potential scores range from 0 to 10, with higher scores indicating greater methodological rigor. A third investigator adjusted the quality judgment when disagreement or uncertainty arose.
Data analysis/statistical analysis
Pooled mean differences (MDs) or standard deviations (SDs) with 95% confidence intervals (CIs) were used to determine the differences in outcomes between models involving stroke in which stem cell treatment was performed and those in which conventional forms of treatment were performed (RevMan 5.3 software).
Clinical research methods
Search strategy
The present meta-analysis was performed in accordance with the guidelines outlined in the PRISMA statement [17] (Table 1).
We searched the PubMed, Web of Science, Embase, and Ovid databases from inception through May 2018 for RCTs regarding stem cell transplantation for ischemic stroke. The following search strategy was used (take PubMed, for instance): “strokes” or “ischemic stroke” or “cerebral infarct*” or cerebrovascular accident?” or “cerebrovascular apoplexy” or “apoplexy” or “brain vascular accident?” or “cerebrovascular stroke” or “ischaemic stroke” or “ischemia stroke”; “stem cell” or “bone marrow mesenchymal stem cells” or “umbilical cord blood stem cells” or “cord blood stem cells” or “neural stem cells” or “human embryonic stem cells” or “embryonic stem cells” or “induced pluripotent stem cells” or “peripheral blood stem cells”; “transplantation”; human; and #1 and #2 and #3 and #4 (filters: “randomized controlled trial”).
Inclusion and exclusion criteria
We included studies involving all types of stem cell interventions, including the application of autologous mononuclear stem cells (BMSCs), autologous peripheral blood stem cells (PBSCs), (autologous) mononuclear stem cells (MNCs), (autologous) mesenchymal stem cells (MSCs), and umbilical cord mesenchymal stem cells. Inclusion criteria for research participants (patients with ischemic stroke) were as follows: (1) diagnosis of brain stroke in accordance with World Health Organization (WHO) criteria and exclusion of cerebral hemorrhage based on brain computed tomography (CT) or magnetic resonance imaging (MRI) and (2) acute or chronic onset of neurological impairment. Studies performing comparisons between stem cell transplantation and other methods of treatment for ischemic stroke were included. All included studies provided at least one outcome measure regarding transplantation or adverse reactions. Included studies utilized at least one of the following for the assessment of treatment outcomes: National Institutes of Health Stroke Scale (NIHSS), Fugl-Meyer assessment (FMA), Barthel index (BI), or modified Rankin scale (mRS).
Poorly designed RCTs, those in whom the treatment of ischemic stroke through stem cell transplantation was not compared with other methods, and those involving patients under the age of 18 years were excluded. Studies involving participants with severe organ dysfunction, mental illness, or poor physical condition preventing completion of stem cell transplantation were also excluded. Studies without literature to support the data, those from which data could not be extracted, literature reviews, meta-analyses, meeting abstracts, case reports, repeated studies, experimental models, and studies regarding other diseases were also excluded.
Data extraction
Two authors independently screened the literature according to the inclusion and exclusion criteria, extracted data, and assessed the risk of bias based on Cochrane systematic review guidelines (5.1.0 RCT bias risk assessment tools). We extracted the following data: authors, country, year of publication, patient age, gender, time/type of cerebral ischemia, number of patients (treatment group/control group), type of stem cell intervention, intervention dose, route of delivery, and outcome indicators. Furthermore, when the treatment was administered in multiple doses, we considered the sum of all doses administered. We also extracted data regarding the date of the final follow-up outcome assessment.
Data analysis/statistical analysis
Pooled MDs or SDs with 95% CIs were used to determine differences in outcomes between patients with stroke undergoing stem cell treatment and those undergoing other forms of treatment (RevMan 5.3 software). Chi-square tests (level of significance = 0.05) were used to analyze the heterogeneity of the included studies. Chi-square tests were also used to quantitatively determine the magnitude of heterogeneity in combination with I 2. If no significant heterogeneity or small heterogeneity was observed, a fixed-effects model was used. If a large amount of statistical heterogeneity was observed, a random-effects model was used after exclusion. Subgroup analyses were performed when heterogeneity was evident.
Results
Preclinical results
Study characteristics
Our search identified 552 studies related to stem cell therapies for ischemic stroke. Two studies were obtained through other methods, and 62 duplicate articles were removed using Note Express 3.2.0 software. By reading the titles and abstracts of 492 articles, we then excluded 465 articles with irrelevant topics or study types. We then evaluated the full text of the remaining 27 studies for inclusion, after which 11 studies were included. Finally, a total of 11 studies—18 independent interventions were ultimately included. (If more than one intervention was provided in a single study, each intervention was regarded as independent. For example, in the study characteristics shown in Table 2, two independent studies took the form of “Author I and Author II,” with two different interventions in each study) (Fig. 1a shows the retrieval flow chart).

Characteristics of Preclinical Studies
hMSCs, human mesenchymal stem cells; hUCB-MNCs, human umbilical cord blood mononuclear cells; hUCB-MSCs, human umbilical cord blood-derived mesenchymal stem cells; IA, intra-arterial; ICa, intracerebral; ICb, intrathecally; IP, intraperitoneal; IV, intravenous; MCAO, middle cerebral artery occlusion; mNSS, modified neurological severity score; MRI, magnetic resonance imaging; NA, not applicable; NSCs, neural stem cells; rMNCs, rat mononuclear stem cells; rMSCs, rat mesenchymal stem cells.
Five types of stem cell therapy were identified: one involving neural stem cells (NSCs), six involving rat mesenchymal stem cells (rMSCs), one involving rat mononuclear stem cells, eight involving human mesenchymal stem cells, and two involving human mononuclear stem cells. Six of the 18 interventions were performed in an animal model of transient middle cerebral artery occlusion (MCAO), whereas the remaining 12 were performed in a model of permanent MCAO. Treatments were administered intravenously in 10 studies, through the carotid artery in 5 studies, through intracerebral transplantation in 1 study, and intrathecally in 1 study. The route of administration was not reported for the remaining intervention. The duration of follow-up ranged from 1 to 14 weeks. Fourteen studies reported outcomes regarding infarction volume, which was assessed using histological methods. Functional outcomes were assessed based on mNSSs in seven studies. For detailed characteristics, see Table 2.
Quality assessment and bias risk
The quality score of each preclinical study was determined in accordance with the scale developed by Lees et al. [15], which includes 10 criteria based on the STAIR guidelines [16,17]. For detailed characteristics, see Table 3.
Quality Score Criterion of Each Included Study
Meta-analysis and effect evaluation
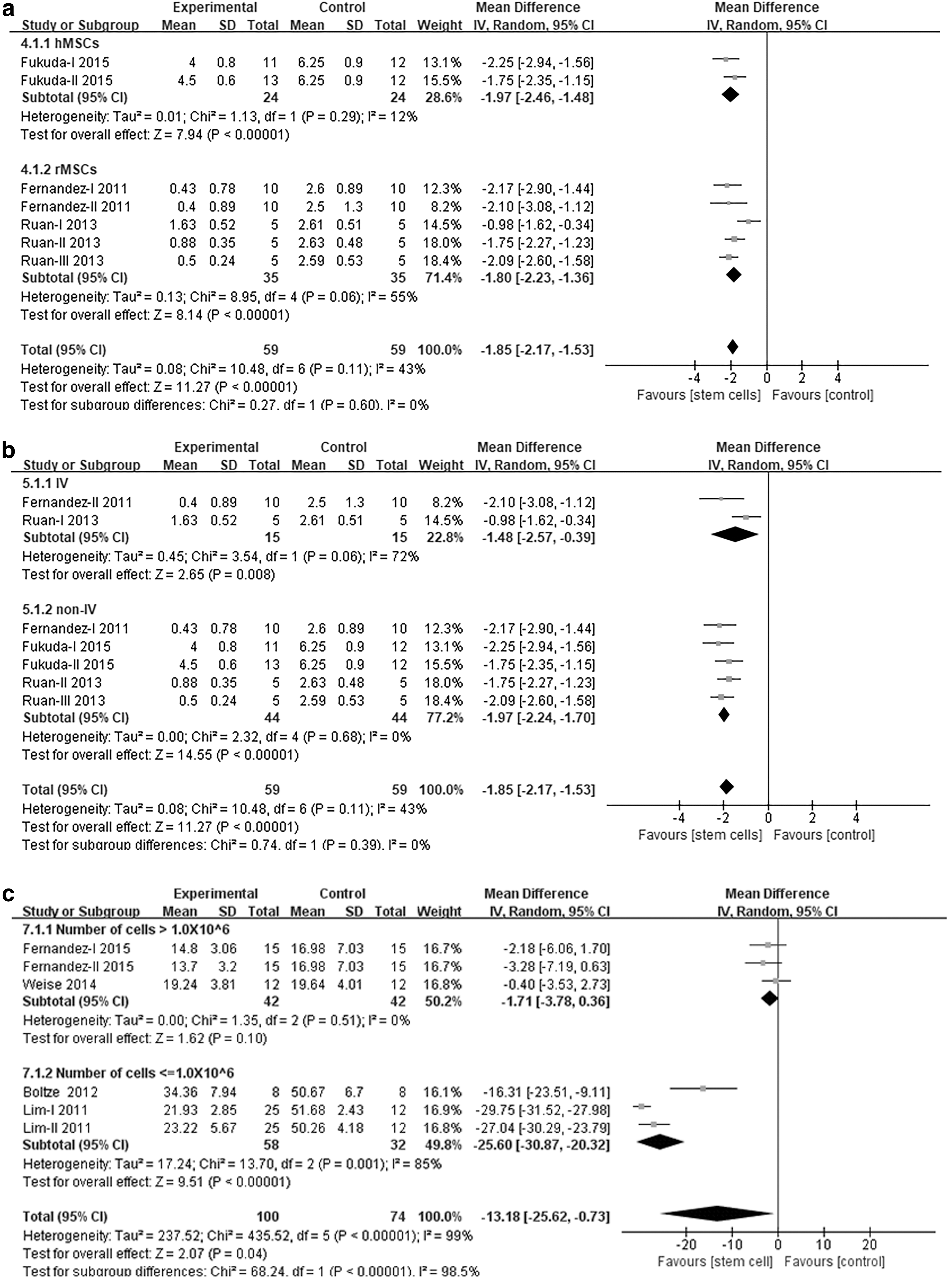
Figure 2a–c shows the standardized effect sizes for infarct volume, the percentage of lesion volume, and mNSSs at follow-up between the stem cell therapy and control groups in each study and across all studies. The composite weighted mean (95% CI) effect sizes for lesion volume, the percentage of lesion volume, (the percentage of the lesion area measured in the literature), and mNSSs were 46.59 (−62.04 to −31.15; P < 0.001), −13.18 (−25.62 to −0.73; P = 0.04), and −1.85 (−2.17 to −1.53; P < 0.001), respectively. Overall, during the follow-up period, the lesion area decreased in the stem-cell treatment group, whereas the mNSSs be improved. Simultaneously, the meta-analysis revealed that all three outcomes were significantly more favorable in the stem cell group than in the control group.

Mean difference between stem cell therapy group and control group in individual trials and all studies combined. Standardized mean difference (95% CI) of total infarction volume
Subgroup analysis
We performed subgroup analysis of mNSSs and the percentage of lesion volume to further evaluate the efficacy of stem cell transplantation based on several variables in Tables 4 and 5. We focused on interactions between the type of stem cell intervention/number of cells and the percentage of lesion volume results. Similarly, we focused on interactions between route of delivery and the mNSS results, which were reported, respectively. The composite weighted mean (95% CI) effect sizes for the type of stem cell (rMSCs), the route of injection (intravenous), and the cell dose (≤1.0 × 106) were −1.80 (−2.23 to −1.36), I 2 % = 55%; −1.48 (−2.57 to −0.39) I 2 % = 72%; −25.36 (−30.87 to −20.37) I 2 % = 85%; (P < 0.001). Actually, the heterogeneity of all subgroups decreased, indicating that these factors may be the source of heterogeneity, which revealed that outcomes were more favorable in the rMSCs group, intravenous group, and low-dose (cells ≤1.0 × 106) group. Forest plots for other outcomes are included in Fig. 3a–c.
Subgroup analysis of preclinical studies. Type of stem cells
Study of Correlation Grouping and Heterogeneity Between Modified Neurological Severity Scores and Variables
Study of Correlation Grouping and Heterogeneity Between the Percentage of Lesion Volume and Variables
Clinical research results
Study characteristics
Our initial search identified 566 studies related to stem cell therapies for ischemic stroke. Six studies were retrieved using other methods, whereas 130 duplicate articles were removed using NoteExpress software. By reading the titles and abstracts of 442 articles, we excluded 413 articles with irrelevant topics, resulting in a potential total of 29 articles. After reading the full text, 13 articles were eventually included, although information could not be extracted from 2 studies. A total of 11 studies were ultimately included (Fig. 1b).
Eight studies utilized stem cells extracted from bone marrow. Stem cells were derived from peripheral blood and the umbilical cord in one and two studies, respectively. In addition, 7 of the 11 interventions were performed in patients with acute/subacute cerebral ischemia, whereas 4 were performed in patients with chronic cerebral ischemia. Furthermore, 3 of 12 treatments were administered through the subarachnoid space, whereas one treatment each was administered through the carotid artery, stereotactic transplantation, or the combined subarachnoid/intravenous route. Treatments were administered intravenously in five studies. The cell dose utilized in each study ranged from 3 × 106 to 300 × 106. The duration of follow-up ranged from 3 to 60 months. For detailed characteristics, see Table 6.
Characteristics of Clinical Studies
BI, Barthel index; BM-MNCs, bone marrow-derived mononuclear cells; BMSCs, autologous mononuclear stem cells; FMA, Fugl-Meyer assessment; MNCs, (autologous) mononuclear stem cells; mRS, modified Rankin scale; MSCs, (autologous) mesenchymal stem cells; NIHSS, National Institutes of Health Stroke Scale; PBSCs, autologous peripheral blood stem cells; UC-MSCs, umbilical cord mesenchymal stem cells.
Quality assessment and bias risk
Most studies are associated with some degree of bias. Owing to policies regarding the experimental design of the RCT, the risk of bias in English studies is lower than that in Chinese studies. However, due to the nature of stem cell transplantation, it is impossible to achieve double-blindness between the participant and the investigator when acquiring stem cells, although this does not influence the experimental results. Thus, we consider the included studies to have a low risk of bias (risk bias is shown in Fig. 4).
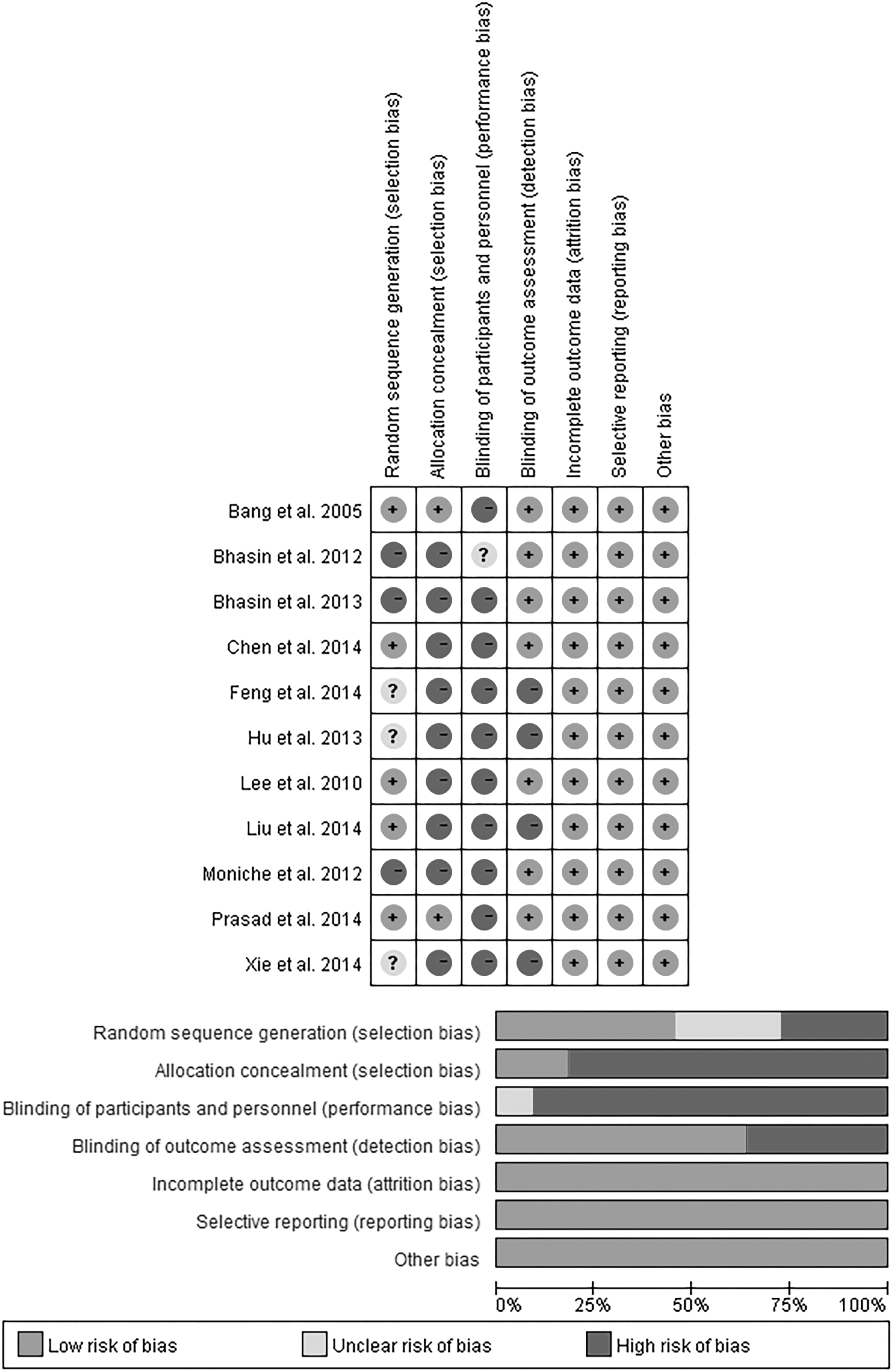
Clinical study quality or risk of bias report.
Meta-analysis and effect evaluation
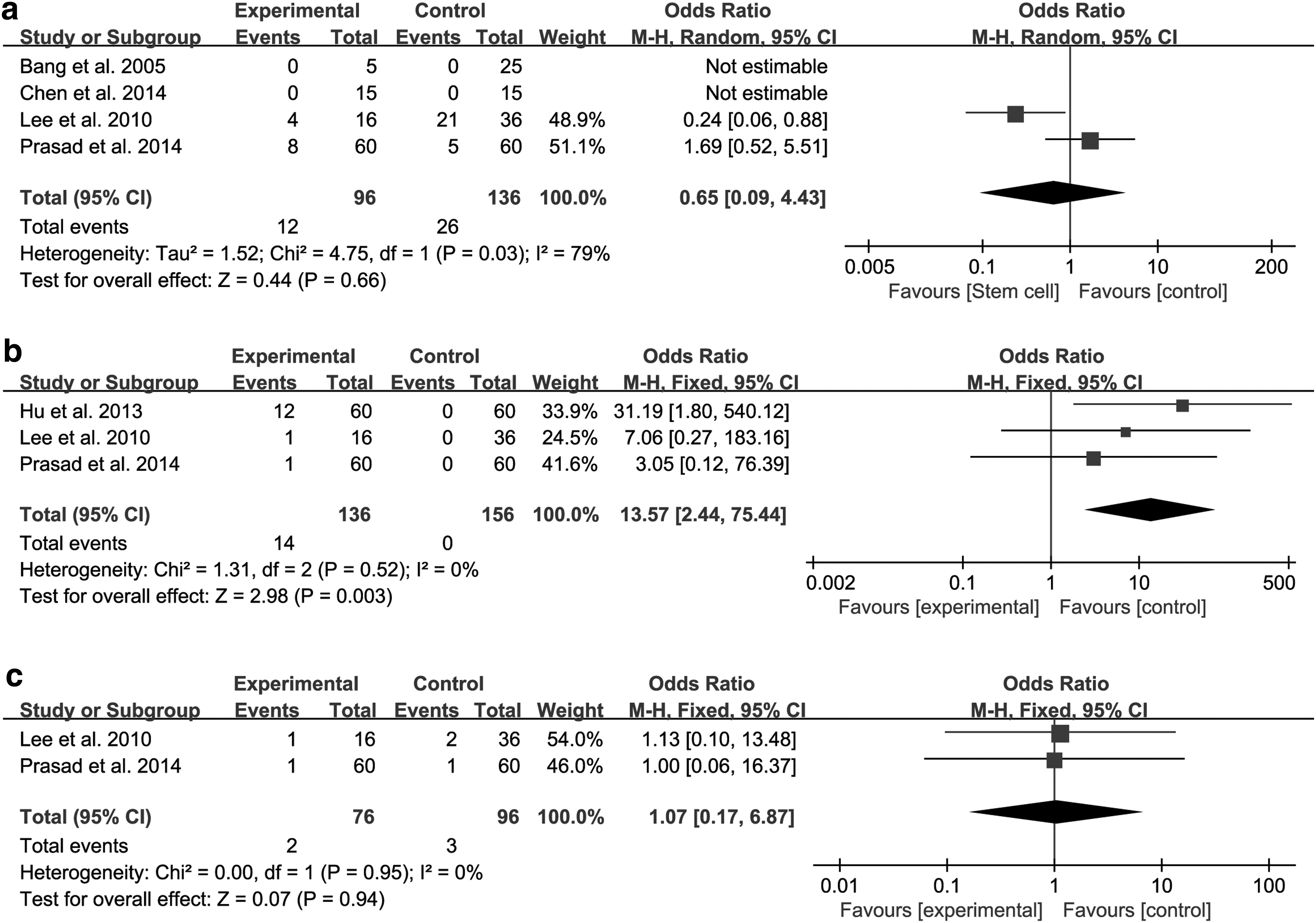
Our pooled analysis revealed that stem cell transplantation was associated with improvements in mRS scores in 4 studies [27 –30], FMA results in 5 studies [31 –35], mBI values in 7 studies [28,30,32,34 –37], and NIHSS scores in 6 studies [27,28,31,32,36,37]. The results of our meta-analysis were as follows: NIHSS [MD = −2.57, 95% CI (−3.45 to −1.68), I 2 = 51%, P < 0.001, Fig. 5a]; BI [MD = 7.93, 95% CI (3.11 to 12.75), I 2 = 59%, P = 0.001, Fig. 5b]; mRS [MD = −0.53, 95% CI (0.73 to −0.28), I 2 = 0%, P < 0. 001, Fig. 5c]; and FMA [MD = 5.50, 95% CI (2.05 to 8.95), I 2 = 15%, P = 0.002, Fig. 5d]. In fact, in the included studies, patients were enrolled on the basis of a NIHSS score of >7. In the stem cell treatment group, the improvement of the mentioned indicators was significantly superior to that of the control group. NIHSS and mRS scores in the treatment group were lower than those in the control group, and FMA and mBI scores in the treatment group were higher than those in the control group. These results suggest that stem cell transplantation was associated with significantly better outcomes than conventional treatments. Treatment was associated with adverse reactions such as mild fever and headache, which resolved after a short time. No significant differences in the rates of death or tumor were observed between the experimental and control groups, whereas significant differences in the rates of fever were observed between experimental and control groups. Death [MD = 0.65, 95% CI (0.09–4.43), P = 0.66, Fig. 6a]; fever [MD = 13.57, 95% CI (2.44–75.44), P = 0.003, Fig. 6b]; and tumor [MD = 1.07, 95% CI (0.17–6.87), P = 0.94, Fig. 6c].

Mean difference between stem cell therapy group and control group in individual trials and all studies combined. Standardized mean difference (95% CI) in NIHSS
Mean difference between stem cell therapy group and control group in individual trials and all studies combined. Standardized mean difference (95% CI) in death
Subgroup analysis
We analyzed the source of heterogeneity by evaluating BI and FMA results in a subgroup analysis (Tables 7 and 8). We focused on interactions between the type of stroke/type of stem cell intervention/route of delivery/number of cells, and outcome indicators, which were reported in the tables, respectively. The composite weighted mean (95% CI) effect sizes for the type of stroke (acute stroke), the route of injection (intravenous), the cell dose (≤100 × 106), and the type of stem cell (umbilical cord-derived stem cell) were 9.33 (0.24–18.42), I 2 % = 70%; 7.26 (1.10–13.42) I 2 % = 42%; 5.09 (3.82–6.36) I 2 % = 70%; 9.04 (3.95–14.13) I 2 % = 0% (P < 0.01). Actually, the heterogeneity of all subgroups decreased, indicating that these factors may be the source of heterogeneity, which revealed that outcomes were more favorable in the earlier umbilical cord-derived stem cells group, intravenous group, and low-dose (cells ≤100 × 106) group.
Study of Correlation Grouping and Heterogeneity Between Barthel Index and Clinical Variables
Study of Correlation Grouping and Heterogeneity Between Fugl-Meyer Assessment and Clinical Variables
Discussion
In this study, we performed a meta-analysis to evaluate the safety and efficacy of stem cell therapy for ischemic stroke. The conclusions of our meta-analysis are consistent with those of previous meta-analysis [15,38,39]. although these previous meta-analyses included nonrandomized trials, we included standard RCTs only, to improve the overall quality of the included studies and ensure that more reliable data could be obtained for analysis. Similarly, a previous meta-analysis of clinical studies [40] includes a high number of Chinese studies, and the methods used for randomization and blinding in the included studies were not sufficiently rigorous. Furthermore, we combined data from preclinical and clinical studies to perform an overall analysis of the current status of stem cells in the treatment of ischemic stroke.
Although our overall meta-analysis indicated that stem cell therapy is effective in the treatment of ischemic stroke, 3 of the 11 preclinical studies [41 –43] reported no significant improvements. However, Riegelsberger et al. [41] and Weise et al. [42] indicated that they failed to detect the neuroprotective effects of cryopreserved human umbilical cord blood (hUCB) MNCs, even though previous studies have reported that freshly isolated hUCB-MNCs are generally associated with beneficial effects. These findings suggest that differences in cell storage and processing can impair the efficacy of treatment [7]. Furthermore, the authors also agreed that, although no reductions in infarct size were observed, rates of cell death were reduced, suggestive of early tissue preservation. In addition, these studies produced no critical evidence of adverse effects or tumor formation.
The subgroup analysis in this study showed that the efficacy in the stem cell group was superior to that of the conventional group through the intravenous route. However, the sample size of the subgroup analysis was small, and there may be false positive or false negative results. In addition, after intravenous infusion, most of the infused cells are trapped in filtering organs such as the lungs [44]. Admittedly, translation of stem cell therapy is dependent on achieving viable cell delivery to the human brain, with a volume a thousand times larger than the mouse. Intra-arterial (IA) injection can achieve a more localized distribution; however, its efficacy is limited by unpredictable cell destination, homing restricted to the vascular territory, and safety concerns [45]. Stem cell diameters range from 7 μm for bone marrow mononuclear cells, 13–15 μm for NSCs, and >25 μm for mesenchymal stem cells. Mesenchymal stem cells are frequently characterized by large size and expression of specific markers, including CD44, CD90, CD106, or Stro-1 [46]. Actually, small cells, which are not equipped with specific receptors, just go through cerebral vasculature unstopped, thus there is no major advantage of the IA route.
However, with large size cells, there is an obvious risk that the cells may cause considerable vascular obstructions [46]. Moreover, a recent study by Cui et al. [47] has noted that adverse effects may occur in animals (eg, microthrombi and reduced cerebral blood flow), and conducted that both cell dose and infusion velocity contribute to complications encountered after IA cell transplantation. However, Cui et al. [48] indicated that ITGA4 overexpression on MSCs enhances transendothelial migration in vitro, but not in vivo, although it improves safety after intracarotid transplantation into stroke rats. These studies on IA safety also deserve our attention. In addition, Walczak et al. [45] indicated that real-time MRI allows for highly precise IA infusion of stem cells to the central nervous system, which may facilitate the use of this minimally invasive route to deliver cells to the vast but defined brain regions, and is especially critical for large brains such as the human brain. They have showed the feasibility of this technique in large animals using clinical MR scanners, making this approach fully clinically translatable. Therefore, the different delivery routes deserve our close attention, which could provide more reliable evidence for the treatment of ischemic stroke by stem cell transplantation.
Among the 11 clinical studies analyzed, stem cell treatment was associated with significant improvements in daily living ability and motor function relative to the values observed for the control treatment. Several clinical studies have been performed on stem cell therapy recently. Kalladka et al. [49] performed a first-in-man study, which offered preliminary data on the feasibility, tolerability, and cell-related safety of stereotactic intracerebral injection of genetically modified CTX0E03 human NSCs in patients with chronic ischemic stroke. Similarly, Steinberg et al. [50] carried out the first reported intracerebral stem cell transplant study for stroke in North America; treatment with modified bone marrow-derived mesenchymal stem cells (SB623) was safe and well tolerated and demonstrated a significant improvement in neurological function after 12 months. In addition, Athersys has developed “MultiStem,” as a cell therapy for treatment of acute injury such as stroke, TBI, and spinal cord injury [51 –54].
Multipotent adult progenitor cells are a bone marrow-derived allogeneic cell therapy product that modulates the immune system and represents a promising therapy for acute stroke. Hess et al. [55] performed a phase 2 randomized double-blind placebo-controlled dose-escalation trial of intravenous multipotent adult progenitor cells in 33 centers in the United Kingdom and the United States. From their research, it was found that administration of multipotent adult progenitor cells was safe and well tolerated in patients with AIS. Most importantly, their results appear to indicate that the window of this therapy may extend beyond the limits of the current care using t-PA. However, due to the failure of data extraction, we failed to incorporate relevant research results into our analysis.
According to our subgroup analysis, early stem cell transplantation and intravenous delivery in the stem cell group appear to be more effective than in the control group. However, cell delivery through the intracerebral route is difficult to perform in the acute phase because of hematoma formation, which further increases the risk for cerebral bleeding. Meanwhile, the intravenous infusion route is indeed a relatively common infusion method. At the same time, it cannot be ignored that although IA transplantation is an invasive approach, it can directly implant these cells in the affected territory with less risk than direct stereotactic implantation and with better dose deployment compared with the intravenous route [56,57]. Although current treatment options alone cannot improve stroke outcomes, patients with brain damage due to stroke usually exhibit varying degrees of spontaneous recovery, suggesting that the brain contains endogenous repair mechanisms [58]. Although such mechanisms are insufficient for full recovery, several studies have suggested that stem cell therapy represents a promising strategy for the treatment of stroke [59].
Previous studies have suggested that stem cell transplantation may aid in forming new neuronal circuits, reducing apoptosis, reducing inflammation, promoting angiogenesis, promoting neurogenesis, and promoting other endogenous repair processes [60,61]. Our research team has also been committed to investigating the mechanisms underlying the efficacy of stem cell treatment for ischemic stroke. MSCs are considered to promote the protection and repair of brain tissue through paracrine activity. Huang et al. [62] suggested that astrocytes are critical for ischemic stroke, as they exert protective effects on mesenchymal damage mediated by MSCs.
In addition, Lv et al. [63] deemed that the death of BMSCs after transplantation is a serious obstacle to therapeutic outcomes after cerebral infarction. They, therefore, investigated whether modification with hypoxia-inducible factor 1α (Hif-1α) can improve the survival of implanted BMSCs, observing that Hif-1α protects against oxygen and glucose deprivation (OGD)-induced damage by promoting cell viability and inhibiting apoptosis. Despite the findings of previous animal studies, it remains unclear to what extent neurogenesis occurs in the mature human brain. Recently, a meaningful study [64] reveals that NHE1 protein is a potential therapeutic target critical for differential regulation of ischemic neuronal injury, demyelination and tissue repair. Fang et al. [65] performed a two-center randomized placebo-controlled phase 1/2a trial with blinded outcome assessment involving 18 patients with acute cerebral infarction within the MCA territory, with a follow-up duration of up to 4 years. Our results suggest that autologous transplantation of endothelial progenitor cells improves the long-term safety of treatment in patients with acute cerebral infarction, supporting the feasibility of this novel method for treatment of ischemic stroke. However, further research is required to fully elucidate the mechanisms underlying functional recovery, and to provide reliable evidence for translating stem cell-based therapies for use in clinical settings.
At present, stem cell transplantation is yet to be fully implemented for the treatment of ischemic stroke in clinical settings. In this study, we performed a meta-analysis to qualitatively and quantitatively evaluate the safety and efficacy of stem cell transplantation therapy. Taken together, our findings suggest that comprehensive treatment involving stem cell therapy represents a promising strategy for combating ischemic stroke. Although the clinical application of stem cell treatment for neurological disorders is currently in its infancy, our findings support the notion that early stem cell therapy may lead to greater improvements in cognitive and motor function in affected patients, relative to conventional treatments. Nonetheless, further studies involving larger sample sizes and longer follow-up periods are required to verify the efficacy and safety of such treatment.
Limitation
Several limitations of this study should be considered. First, our search strategy included English data and Chinese data, but did not take into account the fact that other languages may bring a certain degree of selective bias. In addition, some excellent clinical studies could not be included in the clinical analysis because of the lack of original data. Finally, in the analysis of our preclinical study, we used the mNSS as one of the outcome indicators. In fact, the mNSS was the most frequently applied behavioral test in the reviewed studies, but the improvement of mNSS may be due to improvement of complications rather than the recovery of motor function, especially in incomplete or even no randomized studies [66]. Subsequently, Knieling et al. [67] showed that a rich environment mainly improves behavioral results by compensating for motion. Jolkkonen colleagues [68] also pointed out the advantages and disadvantages of the outcome indicator in the form of a review published in 2018. They pointed since there is a spontaneous recovery mechanism in animal within 1 or 2 weeks, mNSS tends not to be useful for long term studies [68]. Consideration of that mentioned, all of our included preclinical studies were RCTs, and the follow-up time was almost 1–3 weeks, where the mNSS was applicable. However, to convincingly discriminate real functional recovery from compensation, more rigorous behavioral testing or kinematic analyses are required.
Footnotes
Acknowledgments
This study was supported by grants from the Natural Science Funds of China (grant nos. 81874077 and 81171179), Fund for Key Natural Science Foundation of Guangdong (grant no. 2016B030230004), and the Educational Commission of Guangdong (grant no. Yuejiaoyan (2018)17, no. 2013CXZDA008), Key Projects of Health Collaborative Innovation of Guangzhou (grant no. 201803040016, no. 201400000003-2) to Prof. Xiaodan Jiang. This study was also supported by part of the fund from the Guangdong Provincial Clinical Medical Centre for Neurosurgery (grant no. 2013B020400005).
Author Disclosure Statement
The authors declare that they have no competing interests.