
Abstract
Adipose-derived stem cells (ASCs) possess a well-characterized capacity to enhance cutaneous wound healing. However, many controversies exist regarding ASCs from diabetic patients (dASCs). No report exists on the administration of dASCs for the treatment of pressure ulcers. The aim of this study was to compare properties of dASCs and nondiabetic ASCs (nASCs). In addition, we studied if dASCs enhanced pressure ulcer healing in a rodent pressure ulcer model and investigated underlying mechanisms. We found similar expression of cell surface markers and characteristics in dASCs and nASCs, although dASCs exhibited decreased proliferation and osteogenic differentiation capacity and enhanced adipogenic differentiation capacity. dASCs had beneficial effects on chronic wound healing, though some aspects of their capacity were impaired. The ability of dASCs to promote nerve regeneration was not compromised. dASCs promoted pressure ulcer healing and improved healing by modulating inflammation, promoting angiogenesis and neuroregeneration, enhancing collagen deposition, and increasing re-epithelization. These data may provide a theoretical foundation for further clinical administration of ASCs for chronic wound healing in patients with diabetes.
Introduction
Diabetes mellitus is a chronic metabolic disorder that seriously harms human health worldwide and often leads to pressure ulcer formation. Chronic wounds present large challenges to health care systems globally. Current treatments for pressure ulcers rely on traditional surgical debridement, flap reconstruction, negative pressure devices, artificial skin substitute, and topical external application of growth factors [1,2]. However, in some cases, wounds appear that are highly resistant to treatment, for which treatment may be ineffective, or that progress slowly [3]. Therefore, developing new therapeutic methods that are more effective is necessary.
Mesenchymal stem cells (MSCs) are an attractive approach for cell-based therapy of intractable chronic wounds [4]. MSCs derive from many tissues, including bone marrow, adipose tissue, and umbilical cords [4]. Adipose-derived stem cells (ASCs) are adult stem cells that express the characteristics of MSCs and differentiate into various cell types [5]. In addition to their multipotency, ASCs are immunosuppressive and promote wound healing through secreting multiple cytokines [6]. Other advantages of ASCs include abundant availability, general absence of ethical restrictions, and ease of separation. Therefore, ASCs have become a promising source of MSCs for tissue regeneration and repair.
Animal studies showed that allogeneic transplantation of ASCs for intractable chronic wounds, including from diabetes, pressure ulcers, radiation, and burns, achieved good therapeutic effects [7 –9]. In clinical studies, autologous ASC transplantation also showed positive results [10,11]. However, few clinical reports are available on allogeneic transplantation of ASCs for wound healing. This absence of reports is because of the risk of immunogenic reactions in allogeneic transplantation, despite the low immunogenicity of MSCs [12]. Nonetheless, autologous ASC transplantation has attracted attention for clinical applications.
The environment from which MSCs are isolated may determine their usefulness. Previous studies showed that mitochondrial dysfunction is associated with the development of metabolic syndrome. MSCs isolated from patients with type 2 diabetes and metabolic syndrome exhibit dysfunctions in oxidative stress and autophagy, limiting their therapeutic potential [13,14]. In addition, metabolic syndrome affects cell viability, senescence, and oxidative stress in ASCs [15]. The microenvironment of hyperglycemia and glycosylation products in patients with diabetes can disrupt the ability of cells to promote healing, leading to compromised wound healing [16].
Previous studies showed that human endothelia progenitor cells from patients with diabetes exhibited impaired proliferation, adhesion, and incorporation into vascular structures [12]. The biological function of bone marrow-derived MSCs is also influenced by the diabetic microenvironment [17].
ASCs from diabetic patients (dASCs) are controversial. Diabetes impairs the function and efficiency of ASCs in promoting wound healing [18,19]. In contrast, few reports showed that dASCs still retain the ability to promote wound healing [20]. The administration of dASCs for the treatment of pressure ulcers has not been reported. Therefore, we compared the properties of dASCs and nondiabetic ASCs (nASCs). In addition, we investigated if dASCs enhanced pressure ulcer healing in a rodent pressure ulcer model and elucidated the underlying mechanisms.
Materials and Methods
Ethical approval
Adipose tissues from patients with and without diabetes were obtained from inpatients in the Affiliated Hospital of Zunyi Medical University. All protocols were approved by the Ethics Committee of the Affiliated Hospital of Zunyi Medical University. All animal experiments were approved by the Institutional Animal Care and Use Committee of Affiliated Hospital of Zunyi Medical University and conducted according to the guidelines of the National Health and Medical Research Council (China).
Animal model
Female C57BL/6 wild-type mice (6–8 weeks) were provided by the Animal Experimental Center of the Army Military Medical University (Chongqing, China). All mice were healthy and allowed to acclimatize for at least 1 week before induction of pressure ulcers via magnet application for a previously reported model [7]. Briefly, mice were anesthetized by intraperitoneal injection of 3.5% chloral hydrate (0.1 mL/10 g), and dorsum hair was shaved. Dorsal skin was gently pulled up and placed between two circular 12-mm diameter and 5-mm thickness neodymium magnets (Shanghai Qi Hao Electrical Co., Ltd, China) for 12 h. Magnets were removed after12 h for one ischemia–reperfusion (IR) cycle. Mice were exposed to two IR cycles, resulting in two wounds per mouse after 2 days. Histological examination of wounds confirmed the establishment of pressure ulcer model.
Isolation, culture, and flow cytometric identification of dASCs and nASCs
Human subcutaneous adipose tissue was harvested after obtaining signed informed consent from donors with (n = 3) and without (n = 3) diabetes who were undergoing procedures at the Department of Plastic Surgery, Affiliated Hospital of Zunyi Medical University, China.
ASC isolation was performed as previously described [6]. Briefly, human subcutaneous adipose tissue was minced, washed, and digested with 0.075% collagenase type I (Sigma, St. Louis, MO) for 45 min in a shaker incubator at 37°C. Adipocytes and undigested connective tissues were discarded after centrifuging at 800 g for 5 min. Pellets were resuspended in phosphate buffered saline (PBS; Gibco, Carlsbad, CA) and filtered through a 200-mm mesh followed by centrifugation (800 g; 5 min) to harvest stromal-vascular fraction cell pellets. Retrieved cell fractions were cultured at 37°C with 5% CO2 in Dulbecco's modified Eagle's medium (Gibco) supplemented with 10% fetal bovine serum (Gibco) and 1% penicillin-streptomycin (Gibco). At 80% confluence, ASCs were subcultured and cells at passage 3 were used in experiments.
Analysis by flow cytometry of cell surface markers involved resuspending 1 × 106 ASCs in PBS and staining with anti-CD90, anti-CD105, anti-CD73, anti-CD44, and anti-CD34 (all 1:1,000; BD, Pharmingen). Samples were incubated for 30 min at room temperature, washed with PBS, and analyzed with a Mofloxdp flow cytometer (Beckman Coulter, Brea, CA) with Kaluza software (Beckman Coulter).
Osteogenesis and adipogenesis of dASCs and nASCs
Multilineage differentiation of ASCs was as described previously [20]. Osteogenic and adipogenic differentiation of ASCs with, respectively, 1% alizarin red S and oil red O staining were assessed on day 21. All differentiation experiments were performed in triplicate.
To examine the expression of genes related to osteogenic and adipogenic differentiation, nASCs and dASCs were assessed at day 14 after induction. Total cellular RNA was extracted with miRNeasy Mini kits (Dalian Bao Biological Co., Ltd., China) according to the manufacturer's instructions. RNA was purified with DNase I digestion (Invitrogen, Grand Island, NY) and reverse-transcribed using SuperScript VILO cDNA synthesis kits (Invitrogen). Quantitative real-time polymerase chain reaction was performed using EXPRESS SYBR GreenER qPCR SuperMix kits (Invitrogen) according to the manufacturer's instructions. The expression of target genes was analyzed using the ΔΔCt method.
In vivo animal studies
After establishing pressure ulcer models, 48 pressure ulcer wounds on 24 C57BL/6 mice were randomly divided into three groups: nASCs, dASCs, and control. Two types of ASCs were transfected with lentivirus coated with green fluorescent protein (GFP). ASCs (1.0 × 106) were resuspended in 0.5 mL sterile PBS and injected subcutaneously into wounds in the nASC and dASC groups using 27-gauge needles in 1-mL Leur-Lok tip syringes. Controls received 0.5 mL cell-free PBS. All injections were under anesthesia. Each mouse received a total 1 mL (0.5 mL per wound; two wounds per mouse). Injection sites were sealed with an antibacterial protective film (3 M, St. Paul, MN). On days 1, 5, 9, 13, 17, and 21 after injection, gross photos of wound with a steel ruler were taken with a digital camera.
Wound size was estimated by Image J software (Rawak Software, Inc., Germany) and wound healing rates were calculated as follows: (Primary wound size − Residual wound size)/Original wound size × 100%.
Histological examination
On days 11 and 21 after injection, half of each group was sacrificed. On the day of sacrifice, wound skin was harvested and fixed in 10% neutral buffer formalin (Sigma) for at least 48 h and embedded in paraffin. Skin sections (4 μm) were deparaffinized, rehydrated in HistoChoice (Sigma) and graded solutions of ethanol, and stained with hematoxylin and eosin (H&E) or Masson's trichrome stain according to the manufacturer's instructions (Sigma).
Skin sections stained with H&E were assessed for infiltration of inflammatory cell and epidermal thickness at wound centers using Image J software. Skin sections stained with Masson's trichrome were assessed for percentage collagen per skin section. An Image J algorithm was used to deconvolve color information acquired for slides stained with Masson's trichrome. The number of blue pixels was quantified and represented as a percentage relative to the total number of pixels per skin section.
Immunohistochemical analysis
To quantify angiogenesis and neurogenesis within wounds, blood vessel endothelial cells were immunohistochemically stained with anti-CD31 (1:200; Abcam, Cambridge, United Kingdom) and Schwann cells with anti-S100 (1:150; Abcam). Specimens were pretreated through heating followed by blocking with 1% bovine serum albumin (Sigma) and incubated with primary antibody at 4°C overnight. The sections were incubated with secondary antibody (1:250, Abcam) for 30 min. Diaminobenzidine (Invitrogen) and hematoxylin were used to stain and then dehydration, transparent, and mounting were proceeded. Neovascularization of serial sections of specimens was counted with a microscope at high magnification. Percentage positive expression of S100 was determined with Image J software. Statistical analysis was performed on five high-powered fields per sample.
Immunofluorescence staining
Frozen sections were obtained from periwound edges at day 11 after ASC implantation. Samples were treated with frozen embedding agent (Invitrogen). Frozen sections were made and washed with PBS. Nuclei were stained for 5 min by DAPI (1:1,000; Sigma) and washed with PBS. After drying, sections were observed under an inverted fluorescence microscope. With blue light excitation, ASCs showed green and DAPI showed blue fluorescence.
Statistics
Experimental results are presented as means ± standard deviation and analyzed using SPSS (version 17.0; SPSS Inc., Chicago, IL). Student's t-test was used to compare the two groups at single time points. One-way analysis of variance was used to compare groups at all time points. P < 0.05 was considered statistically significant.
Results
Cultivation and identification of dASCs and nASCs
After isolating ASCs from normal subcutaneous adipose tissue and tissue from patients with diabetes, cells were characterized by microscopy and cell surface marker profiling. Two types of ASCs displayed fibroblast-like morphology, with no obvious differences in morphology (Fig. 1A, B). Flow cytometric analysis revealed that ASCs were >90% positive for CD90, CD105, CD73, and CD44 MSC-specific cell markers and negative for CD34 hematopoietic cell markers. Cell markers were expressed at similar levels in dASCs and nASCs (Fig. 1C). These findings demonstrated that dASCs and nASCs had indistinguishable phenotypes.

ASCs from human subcutaneous adipose tissue displayed mesenchymal stem cell characteristics. Phase-contrast micrograph of ASCs showing fibroblast morphology
Osteogenesis and adipogenesis of dASCs and nASCs
To examine the differentiation potential of dASCs, we cultured nASCs and dASCs under conditions that induced differentiation into osteoblasts and adipocytes. Staining with alizarin red examined calcification in osteoblasts, and oil red O staining showed lipid accumulation in adipocytes.
The number of brown-black calcium nodules was lower for the dASC group than the nASC group (Fig. 2A), suggesting weaker differentiation ability toward the osteocyte lineage in dASCs than in nASCs. The number of round lipid droplets was higher for the dASC group than the nASC group (Fig. 2A), suggesting stronger differentiation ability toward the adipocyte lineage in dASCs than in nASCs. Consistent with these gross observations, the expression of two osteogenic genes (bone morphogenetic protein-2 [BMP-2] and bone gla protein [BGP]) was lower in dASCs than in nASCs (Fig. 2B). The expression of an adipocyte-specific gene (peroxisome proliferater-activated receptor-γ [PPARγ]) was higher in dASCs than in nASCs (Fig. 2C).

ASCs differentiated into osteoblast-like and adipocyte-like cells. Differentiation ability differed for nASCs and dASCs. dASCs had less osteogenic differentiation than nASCs, and nASCs had greater adipogenic differentiation ability
ASC treatment enhanced pressure ulcer healing
The efficacy of two types of ASCs in pressure ulcer wound healing was investigated in 6- to 8-week-old mice. The base of wounds was injected with 1.0 × 106 ASCs and assessed over 21 days. The delivery of ASCs to the wound site accelerated wound healing in mice (Fig. 3A). As early as day 5, mice treated with nASCs or dASCs displayed better wound healing than mice treated with PBS. The trend of ASC-accelerated wound healing continued until wound closure was complete on day 17. On days 9 and 13, mice treated with nASCs displayed better wound healing than those treated with dASCs (Fig. 3B).
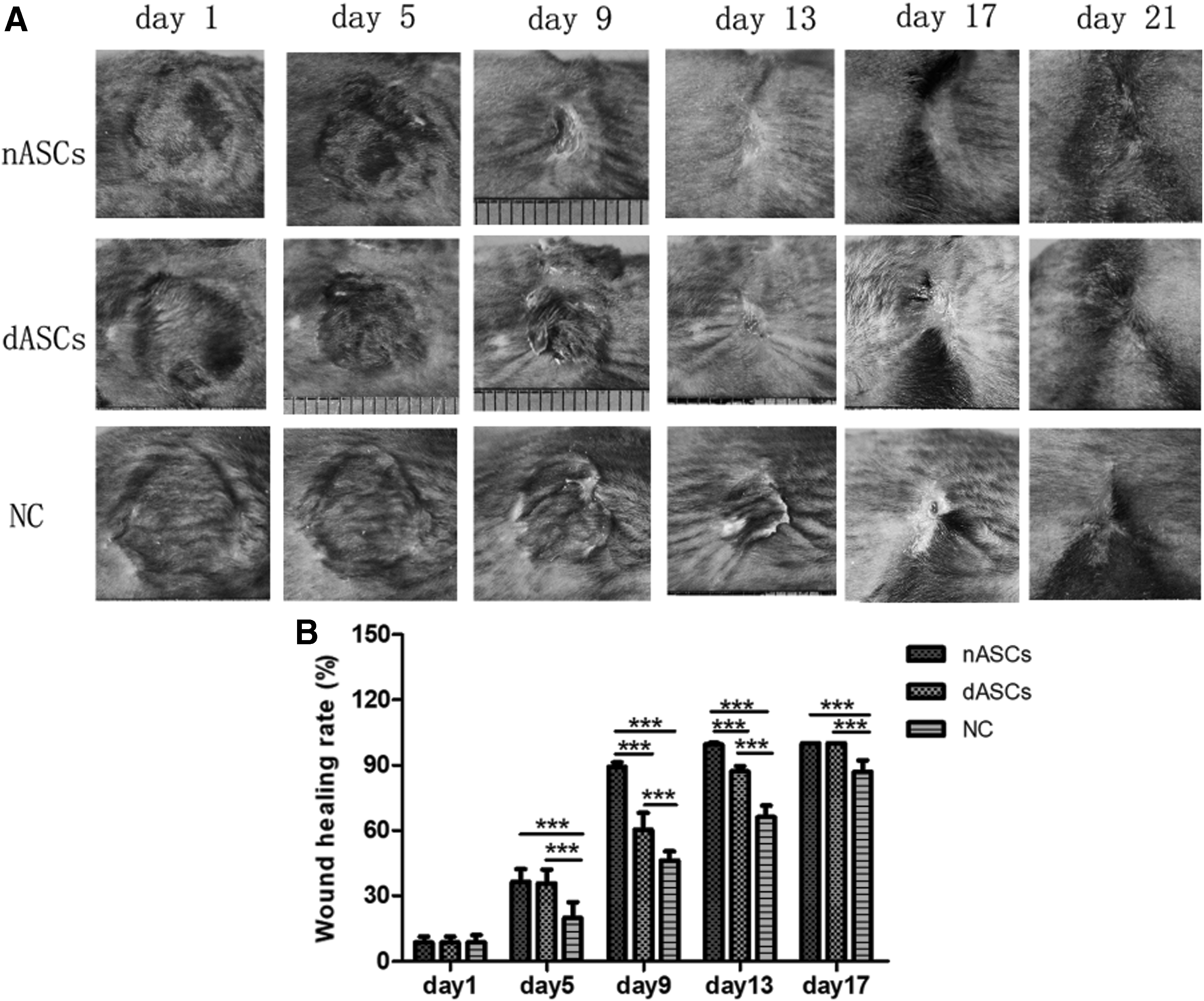
ASC injection into subdermal periwound edges promoted pressure ulcer wound healing. Representative images of wound healing at time points after ASC transplantation
ASC treatment suppressed periwound inflammatory responses and increased epidermis thickness
H&E staining of skin specimens of pressure ulcer wounds from mice revealed that the infiltration of inflammatory cells into the dermis decreased after treatment with nASCs compared with dASCs or PBS on day 11, and decreased with dASCs compared with PBS (Fig. 4A). No significant differences among the three groups were seen in inflammatory cell infiltration on day 21 (Fig. 4A, B). Epidermal thickness decreased in mice treated with nASCs, dASCs, or PBS on day 21 (Fig. 4C).
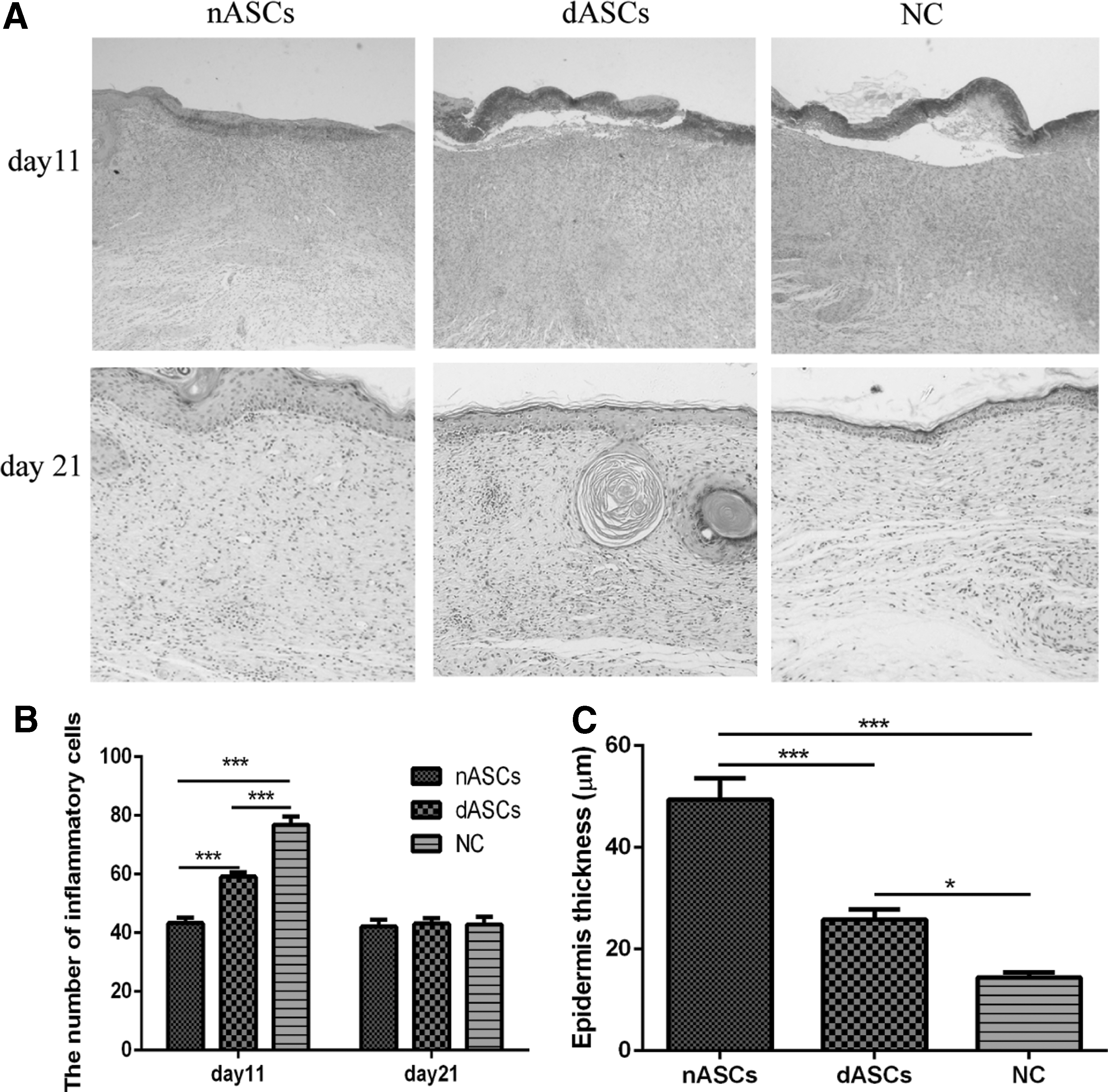
ASC treatment suppressed periwound inflammatory responses and increased epidermal thickness. Histology of inflammatory cell infiltration from dermis to subcutaneous layers, showing a decrease in ASC-treated groups on day 11 compared with controls. The nASC group had the lowest infiltration of inflammatory cells
ASC treatment increased periwound collagen deposition
Masson staining showed more collagen deposition in the dermis of mice treated with nASCs or dASCs compared with those treated with PBS. No significant differences between the nASC and dASC groups were seen on day 11 (Fig. 5). On day 21, collagen deposition was higher in the dermis of mice treated with nASCs than those treated with dASCs or PBS. More collagen deposition was seen in the dermis of mice treated with dASCs than those treated with PBS (Fig. 6).
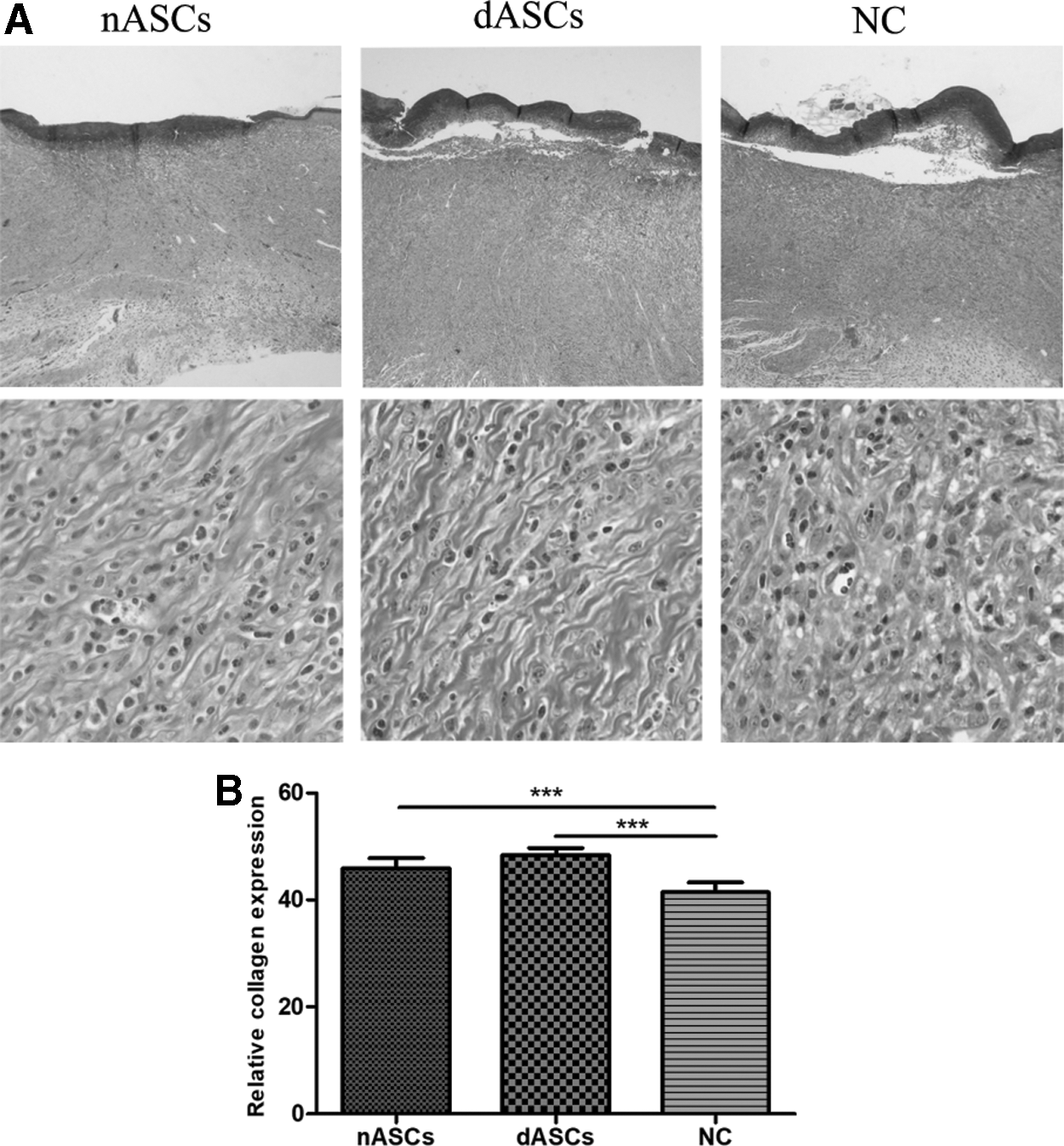
Collagen accumulation in wounds on day 11. Masson staining of collagen deposition in the dermis showed increases in ASC-treated groups on day 11 compared with control group. No significant difference was seen between the nASC and dASC groups
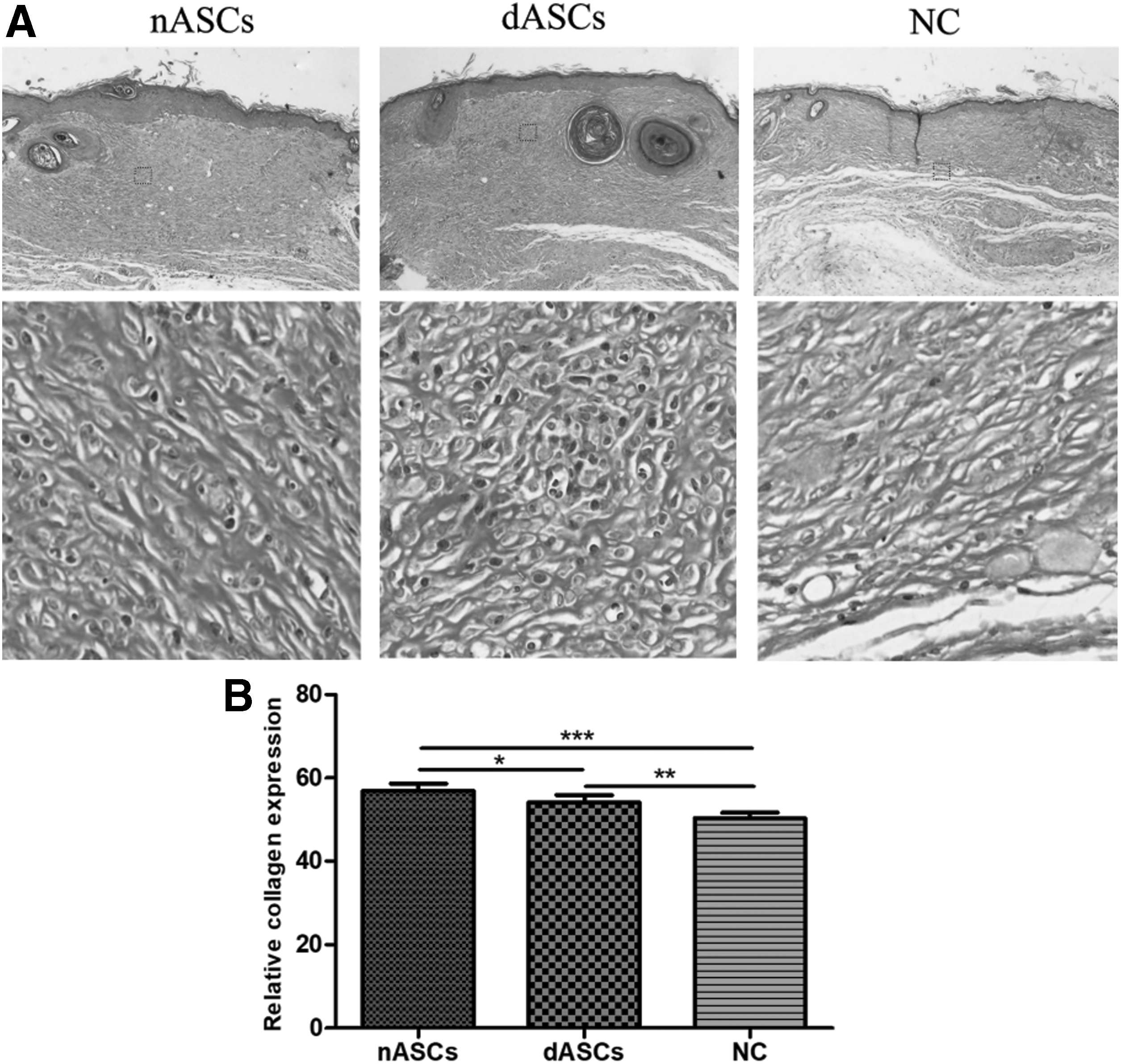
Collagen accumulation in wounds on day 21. Masson staining of collagen deposition in dermis showed increase in ASC-treated groups on day 21 compared with control group and the nASC group showed the highest deposition of collagen
ASC treatment increased periwound angiogenesis
To determine if dASCs increased angiogenesis in wound healing, we evaluated CD31 expression of blood vessel endothelial cells using immunohistochemical staining. More new blood vessels were seen in mice treated with nASCs or dASCs than those treated with PBS; no significant differences were seen between the nASC and dASC groups on day 11 (Fig. 7). On day 21, mice treated with nASCs had more new blood vessels than those treated with dASCs or PBS, and mice treated with dASCs showed more new blood vessels than those treated with PBS (Fig. 7).
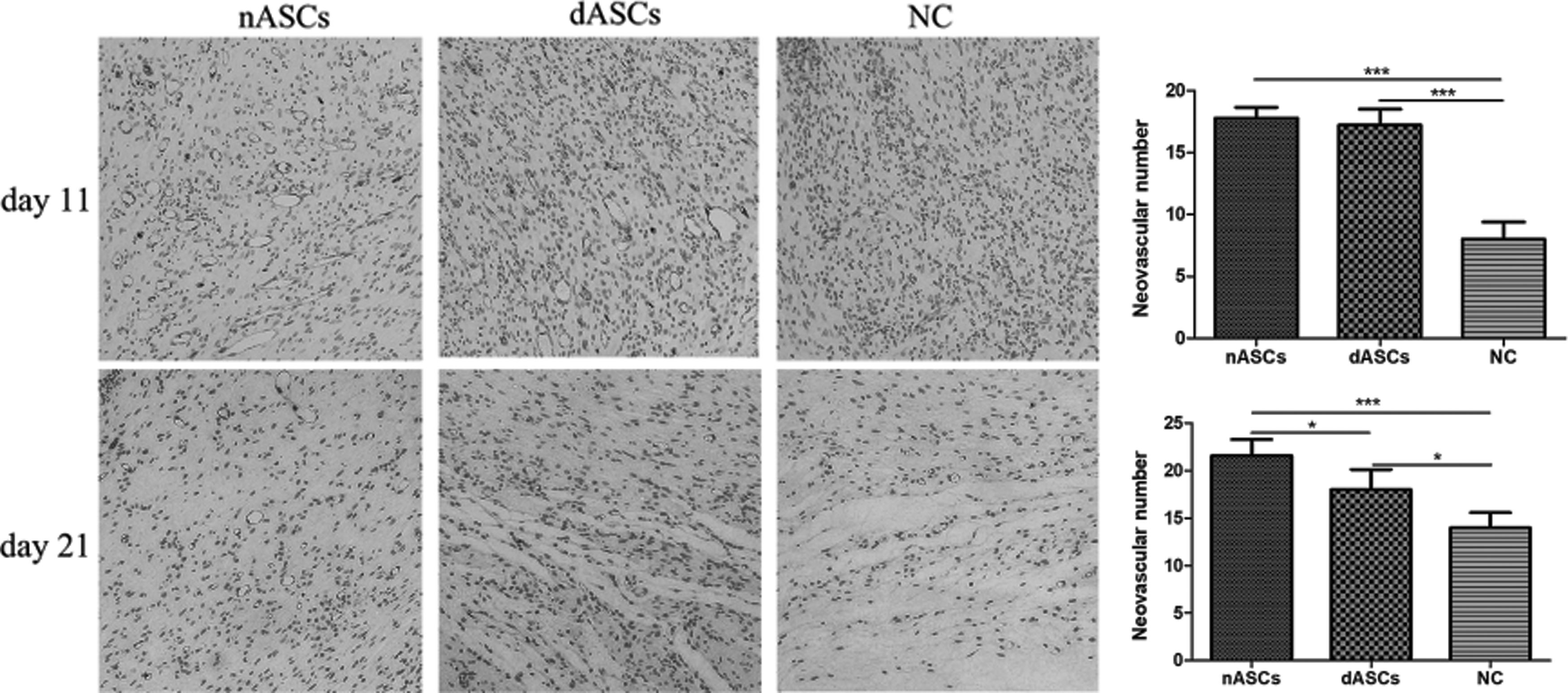
Effects of ASCs on wound neovascularization on days 11 and 21 after cell transplantation. CD31 immunohistochemical staining showed more new blood vessels in ASC-treated groups on day 11 than in the control group with no significant difference between the nASC and dASC groups. On day 21, more new blood vessels were in ASC-treated groups than the control group, with the nASC group having the most new blood vessels. Magnification: 200 × ; *P < 0.05, ***P < 0.001.
ASC treatment increased periwound neuroregeneration
To determine if dASCs increased neuroregeneration in wound healing, we evaluated S100 expression in Schwann cells using immunohistochemical staining. No positive expression was seen in the three groups on day 11. On day 21, mice treated with nASCs or dASCs had more new Schwann cells than those treated with PBS, with no significant differences between the nASC and dASC groups (Fig. 8).

Effects of ASCs on wound neuroregeneration on day 21 after cell transplantation. S100 immunohistochemical staining of nerve cells increased in the dermis in ASC-treated groups compared with the control group with no significant difference between the nASC and dASC groups
ASC periwound homing in vivo
The state of nASCs and dASCs at wound sites was determined by examining GFP expression. Immunofluorescence indicated that GFP-positive ASCs accumulated in the subdermal layer of wound margins in both nASC and dASC groups at 21 days post injection (Fig. 9).
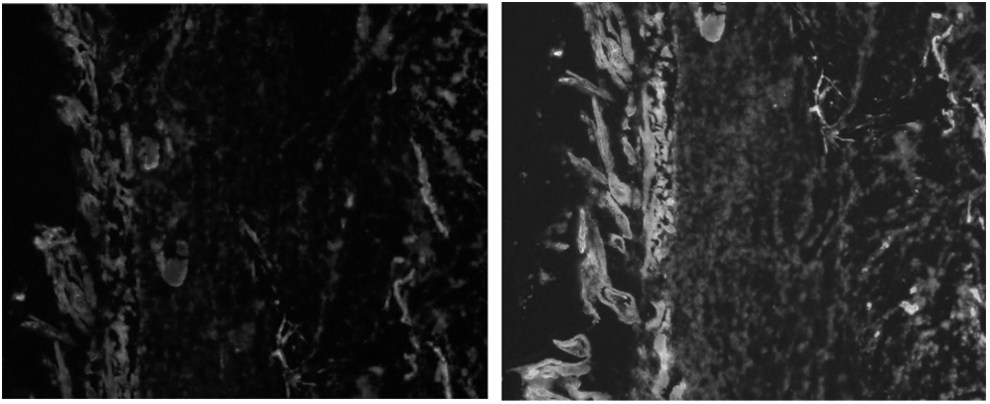
ASCs tracked in vivo in mice with pressure ulcer wounds. GFP-labeled ASCs concentrated at wound edges on day 21 after ASC transplantation.
Discussion
In this study, we compared the biological characteristics of dASCs and nASCs. The expression of cell surface markers in dASCs and nASCs was similar and characteristic of MSCs. Our results were consistent with those of Cianfarani et al. [21]. However, Nawrocka et al. showed that the morphology of these two types of cells is diverse and changes significantly after the addition of fibroblast growth factor [22]. Liu et al. [23] reported that the immunophenotype of dASCs changes and leads to impaired capacity for reducing inflammation.
nASCs had a higher proliferative capacity than dASCs, consistent with Cianfarani et al. [21]. In addition, Cheng et al. also showed that nASCs exhibit decreased proliferation and migration in a diabetic environment [24].
Both types of ASCs can differentiate into osteoblasts and adipocytes. The differentiation capacity of ASCs appears to vary with their source; dASCs have stronger adipogenic differentiation ability than nASCs and weaker osteogenic differentiation ability than nASCs. Our results were consistent with those of Cramer et al. [25]. Cramer et al. indicated that some changes in dASC gene expression are irreversible and the function of dASCs can be recovered only partially after insulin intervention [25]. These results suggest that hyperglycemia may increase the adipogenic capacity of ASCs, and a hyperglycemic environment is unfavorable for homologous osteogenic differentiation of ASCs.
In wound healing experiments, we found that nASC-treated wounds had more rapid wound closure than those treated with dASCs. dASCs accelerated wound healing and improved healing associated with decreased inflammation, enhanced angiogenesis and reepithelization, increased deposition of collagen, and promoted peripheral nerve regeneration. Previous studies demonstrated that the release of hepatocyte growth factor, vascular endothelia growth factor, fibroblast growth factor, insulin-like growth factor, and monocyte chemoattractant protein-1 was significantly reduced from dASCs; these factors are important for healing acute and chronic wounds [26 –28]. Liu et al. [23] showed that dASCs reduced the secretion of prostaglandin E2 (PGE2), and PGE2 reduces the inflammatory response and participates in immune regulation.
Angiogenesis and collagen deposition are important processes in wound healing. In this study, on day 11, H&E staining of wound skin sections showed no significant differences in vascular density or collagen deposition between nASC and dASC groups, but these traits were significantly higher than in the control group. The number of inflammatory cells was significantly lower in the ASC groups than the control group, with the nASC group showing the lowest amount. On day 21, epidermal thickness and accumulation of collagen in the ASC groups were significantly higher than in the control group, with the highest measurement in the nASC group. These results suggest that dASCs had impaired capacity during the process of increasing angiogenesis, modulating inflammation, enhancing re-epithelialization, and accelerating collagen deposition. However, dASCs still had beneficial effects on cutaneous wound healing, especially in the early stage of wound healing; dASCs still promoted angiogenesis and collagen production. Kornicka et al. and Marycz et al. showed that antioxidants reverse the cytophysiological properties of ASCs impaired by metabolic syndrome and age-related deterioration [29,30]. Therefore, we propose that preconditioning dASCs with antioxidants before clinical applications would be reasonable.
Impaired neurological function is considered an important pathophysiological mechanism of pressure ulcers. Neuropathy is a serious complication of diabetes and an important mechanism for the development of diabetic foot. ASCs secrete growth factors or cytokines such as nerve growth factor and brain-derived neurotrophic factor, resulting in the promotion of nerve growth [31]. A previous study demonstrated that dASCs or high glucose-treated nASCs have enhanced expression of pluripotent markers Sox-2, Oct-4, and Nanog [24]. In our study, neuroregeneration seen with S100 immunohistochemical staining showed no significant differences in nerve cell density between the nASC and dASC groups, but more neuroregeneration than the control group. This result may indicate that the neurogenic transdifferentiation potential of ASCs in a diabetic environment is not compromised and may be enhanced. We will further investigate the underlying mechanisms.
On day 21, histological examination revealed denser hair follicles around wounds in the nASC and dASC groups than the control group. Previous studies showed that ASCs are necessary and sufficient to activate follicular stem cells and stimulate hair follicle growth [32,33]. ASC-conditioned medium contains factors that promote hair growth [34]. Therefore, we hypothesize that ASCs may exert their hair growth-enhancing effects through autocrine or paracrine systems.
Conclusion
The expression of cell surface markers and characteristics of MSCs were similar in dASCs and nASCs. dASCs exhibited decreased proliferation and osteogenic differentiation capacity and enhanced adipogenic differentiation capacity. dASC transplantation promoted pressure ulcer healing and improved healing more effectively by modulating inflammation, promoting angiogenesis and neuroregeneration, enhancing collagen deposition, and increasing re-epithelization. dASCs showed beneficial effects on chronic wound healing, although their capacity was impaired. These data may provide a theoretical foundation for further clinical administration of ASCs for chronic wound healing in patients with diabetes.
Footnotes
Acknowledgment
This study was supported by the National Nature Science Foundation of China (no. 81660323, 81801921).
Author Disclosure Statement
The authors have no financial interest to declare in relation to the content of this article.