
Abstract
Several therapeutic strategies are currently in development for severe periodontitis and other associated chronic inflammatory diseases. Guided tissue regeneration of the periodontium is based on surgical implantation of natural or synthetic polymers conditioned as membranes, injectable biomaterials (hydrogels), or three-dimensional (3D) matrices. Combinations of biomaterials with bioactive factors represent the next generation of regenerative strategy. Cell delivery strategy based on scaffold–cell constructs showed potential in periodontitis treatment. Bioengineering of periodontal tissues using cell sheets and genetically modified stem cells is currently proposed to complete existing (pre)clinical procedures for periodontal regeneration. 3D structures can be built using computer-assisted manufacturing technologies to improve the implant architecture effect on new tissue formation. The aim of this review was to summarize the advantages and drawbacks of biomimetic composite matrices used as biomaterials for periodontal tissue engineering. Their conditioning as two-dimensional or 3D scaffolds using conventional or emerging technologies was also discussed. Further biotechnologies are required for developing novel products tailored to stimulate periodontal regeneration. Additional preclinical studies will be useful to closely investigate the mechanisms and identify specific markers involved in cell–implant interactions, envisaging further clinical tests. Future therapeutic protocols will be developed based on these novel procedures and techniques.
Introduction
Periodontitis affects 20%–50% of the world population [1] and is associated with various systemic conditions, such as cardiovascular disease, diabetes, respiratory disease, chronic kidney disease, and other chronic inflammatory diseases such as rheumatoid arthritis [2]. Therefore, researches on novel periodontitis treatment procedures are currently in development. Periodontal therapy is complex, aiming the structural and functional regeneration of the periodontium, which involves formation of cement on the root, attachment of the periodontal ligament to cement, and the newly constituted alveolar bone. There are several techniques and products for periodontal regenerative therapies used in clinics (Table 1).
Commercial Products for Advanced Periodontitis Treatment and Surgical Techniques for Regenerative Periodontal Therapy in Clinics
GTR, guided tissue regeneration.
Guided tissue regeneration (GTR) is a basic treatment applied to patients with periodontal disease and uses membrane barriers that prevent epithelial cell proliferation and stimulate selective repopulation of the periodontal defect [8]. GTR can be used only in some clinical cases, such as intraosseous defects and class II fissure defects. Development of several types of GTR membranes with improved physicochemical, mechanical, and biological properties aimed an increase of bone growth while protecting the gingival tissue, but a whole product for periodontal regenerative therapy is still lacking [9].
The periodontium consists of two soft tissues (gingival tissue and periodontal ligament) and two hard tissues (cementum and alveolar bone), which undergo competitive regeneration processes [10]. Conventional treatment techniques failed to regenerate this complex structure.
As a result, other therapeutic strategies were developed for periodontal regeneration (Fig. 1). Surgical implantation of biomaterials is the first-generation approach for periodontal tissue engineering under controlled conditions [11]. Several polymers were used for spatially and temporally guiding of periodontal regeneration in clinical tests [12,13]. The combination of cell therapy and biomaterials containing bioactive molecules represents a strategy of second- and third-generation approaches used in periodontal regenerative medicine [14]. Complementary to existing clinical procedures, fourth- and fifth-generation therapies have evolved for bioengineering periodontal tissue analogs based on constructs of biomaterials and cell sheets or genetically modified stem cells [15]. However, the risk and long-term efficiency of new bioimplants based on cell–scaffold constructs have to be evaluated in controlled clinical trials. Induced pluripotent stem (iPS) cells and embryonic stem cells allow personalized cell therapy and can improve periodontal tissue regeneration [16,17], but their use is limited by laws in force regarding ethics and genetically modified cells [18]. In addition, there are uncertainty areas in iPS cell biology and their use as bioimplants is proposed to be first applied in clinical tests on dental bone or periodontal defects, where they can be easily followed in long-term studies [19]. Recently obtained, immortalized, human periodontal cells are proposed to replace embryonic tissues in periodontal tissue regeneration [20]. Evolving tissue analogs fabricated by three-dimensional (3D) cell printing technologies target similarities to in vivo tissue characteristics and theranostic applications, but they are currently limited by deficient functionality [21].

Evolution of therapeutic strategies for periodontal regeneration. Material-based strategy provides tissue protection against infection and mechanical stress. Tissue engineering of complex constructs of biomaterial–bioactive factors–stem cells aims at osteoinduction and new tissue formation.
A suitable biomaterial for periodontal tissue engineering and/or cell therapy should mimic the native tissue environment. Unlike natural polymers, for example, collagen, chitosan, and synthetic polymers, for example, polyglycolic acid (PGA), polylactic acid (PLA), polyethylene glycol (PEG), polyvinyl alcohol (PVA), and poly (lactic-co-glycolic acid) (PLGA), copolymers present good stability, degradability, and suitability for fabrication of macro- and microstructures with certain architecture [18]. Nondegradable synthetic materials, such as metals, ceramics, glasses, and carbon, which fulfill at least one property of osteoconductive, osteoinductive, or osteostimulative activity, were used as alveolar bone grafts [22,23]. These biomaterials were conditioned as membranes, hydrogels, or 3D matrices, loaded or not with bioactive factors or cells to obtain valuable constructs for periodontal regeneration. Biomaterials have the potential to enhance the beneficial effects shown by cell therapy, while reducing the risk of grafting failure in human intrabony defects [24]. They lead to better control of cell delivery and decrease of lost cell numbers at the target site. Used as carriers, they allow the delivery of biological agents (growth factors and bioactive compounds) that improve interaction with the host tissue and the cell differentiation process.
This article discusses advantages and limitations of natural and synthetic polymers used for fabrication of biomaterials during evolution of periodontal tissue engineering. It describes their use per se or as composites conditioned as two-dimensional (2D) or 3D scaffolds using conventional or emerging technologies. Recently developed tissue analogs are reviewed as promising future therapeutic procedures.
Membranes for GTR
There are two types of materials used as barriers in clinical research applications, nonresorbable and resorbable membranes [25].
Nonresorbable membranes
Nonresorbable membranes used in GTR are made of polytetrafluoroethylene (PTFE) or titanium. They have several advantages, such as efficiency, biocompatibility, mechanical strength, easy to manipulate, and low risk in long-term clinical applications [26]. Their behavior as effective barriers is more predictable than that of resorbable membranes due to their stable structure, space-maintaining properties, and tailorable porosity [27]. The disadvantages of nonresorbable membranes are the need for a second surgical intervention for their removal, high exposure rate increasing the risk of bacterial colonization, and incomplete isolation of the defect due to their stiffness [26,27].
PTFE, known as Teflon®, is a polymer comprising repetitive fluorocarbon subunits, extensively studied for fabrication of several graft types [28]. Depending on its structure, PTFE is classified as follows: Expanded PTFE presenting two microstructures: a coronal border and an occlusive area [25]. The coronal border with open microstructure facilitates clot formation and adhesion of collagen fibers for membrane stabilization; its internodal distance is 25 μm. The occlusive area allows circulation of nutrients and prevents infiltration of other cell types; its internodal distance is 8 μm. The commercial membrane Gore-Tex®, based on expanded PTFE, is presently tested in clinical periodontal treatments. Implantation of the expanded PTFE membrane together with autogenous bone graft could stop ridge resorption and stimulate the process of bone regeneration [29]. High-density PTFE, obtained for the first time in 1993, was successfully used in bone regeneration. The membrane is very thick, with a small pore size (0.2 μm) that prevents bacterial infiltration within the bone defect in a better way than expanded PTFE membranes [30]. The commercial material Cytoplast™ protects the affected tissue and is easily removed from the tissue due to poor adhesion.
Titanium membranes are widely used in reconstruction of bone defects during various surgical procedures due to their strength and thermal and corrosion resistance. The low density of titanium provides mechanical strength and low weight to dental biomaterials [31]. Several studies envisage surface modifications of titanium implants for enhanced osseointegration [23].
Resorbable membranes
The most commonly used materials for bioengineering resorbable membranes are natural polymers (collagen and chondroitin sulfate, etc.) and synthetic polymers (PGA and PLA, etc.) in different combinations that allow development of membranes with a wide range of structural, chemical, and mechanical properties. On the market, there are products based on natural polymers, such as Paroguide® containing a mixture of collagen and chondroitin sulfate [32] and BioMend® based on cross-linked bovine type I collagen [33], which have the advantage of being biocompatible, easy to use, and reducing the intervention time and patient's discomfort. Their main advantage is easy absorption, thus avoiding a second surgery for their extraction. Biocompatibility is an important feature of a barrier membrane and its lack could lead to the irreversible destruction of periodontal tissue. Resorbable membranes are usually used in periodontal defects due to their capacity to decrease the intraosseous defect depth with variable efficacy [34]. Their disadvantage is the rapid degradation in inflammatory conditions, leading to decrease of the membrane's functionality [25]. Their initial capacity of a spatial barrier is lost during resorption and the process of tissue reconstruction is affected, including implant placement [30]. Cross-linked resorbable membranes attained soft tissue healing [35] and presented a degree of bone formation similar to that induced by nonresorbable membranes [34].
Comparative clinical studies on nonresorbable PTFE membranes and cross-linked collagen resorbable membranes for guided bone regeneration of atrophic posterior mandible reported bone formation and vertical bone gain in both treatment groups [31]. Membrane association with bone grafts significantly improved the treatment of grade II furcation defects of mandibular molars, and in addition, horizontal bone fill was better in case of using resorbable membranes [26].
Hydrogels for Periodontal Regeneration
Recent development of injectable systems is explained by their widespread applicability as delivery systems in tissue engineering and regenerative medicine [36]. Injection of biodegradable hydrogels has great advantages, such as the ability to efficiently and homogeneously encapsulate cells of interest before their solidification at the targeted situs and noninvasive in situ implantation. Hydrogels concentrate cell suspension in the desired area, stimulating cell proliferation and differentiation [18]. They can be fabricated from natural polymers (collagen, chitosan, alginate, and agarose) and their degradation by-products were shown to influence growth factor secretion, cell behavior, and stem cell differentiation [37]. Moreover, the mechanical properties of natural polymers could be improved by cross-linking with synthetic polymers (PEG, PVA, and polyacrylamide). Other soft materials such as preformed gels were used to protect injected cells during surgical implantation and showed stimulation of the initial phase of periodontal tissue repair, providing beneficial therapeutic effects [38]. Several soft biomaterials were used in preclinical studies for periodontal regeneration [18]. A hydrogel of biodegradable PEGylated fibrin was used for dental stem cell encapsulation and transplantation in mice, where it stimulated cell proliferation and led to dental pulp regeneration in periodontal defects [39]. Fibrin was used in cell transplantation owing to its degradability and cell proliferation stimulation, inducing bone regeneration of periodontal defects [40]. Sodium alginate gel mixed with plasma was tested in musculoskeletal and periodontal regeneration [18]. Despite numerous advantages, the use of hydrogels is limited due to their low mechanical and bioinert properties. To obtain hydrogels with proper mechanical strength, their network structure, the gelation process, and cross-linking are important tunable factors, which must be taken into account to improve tissue regeneration [41].
3D Matrices for Periodontal Regeneration
For use in periodontal regeneration, the structure and mechanical properties of 3D porous matrices must be tailored, taking into account the complex structure of the periodontium. Moreover, total porosity of biomaterials and pore size are essential to avoid the absence of nutrients in the central region of the scaffold, leading to cell necrosis [18].
Various biomaterials, including bioactive ceramics, biodegradable polymeric composites, allografts, and autografts, are available for periodontal regeneration, but it is important to develop matrices biomimetic to native composition of the extracellular matrix (ECM) from oral tissues. Our group has vast experience in ECM biomimetic matrices based on collagen, fabricated with variable porosity, depending on the polymer concentration and freezing temperature used for lyophilization [42]. Thus, a proteic–polysaccharidic matrix with interconnected pores was prepared as a 3D scaffold for infiltration and proliferation of dental pulp stem cells (Fig. 2A) [43]. Structural and ultrastructural analyses of a biomimetic scaffold comprising collagen, chondroitin sulfate, and fibronectin revealed a heterogeneous distribution and close interaction between polymeric components [44].
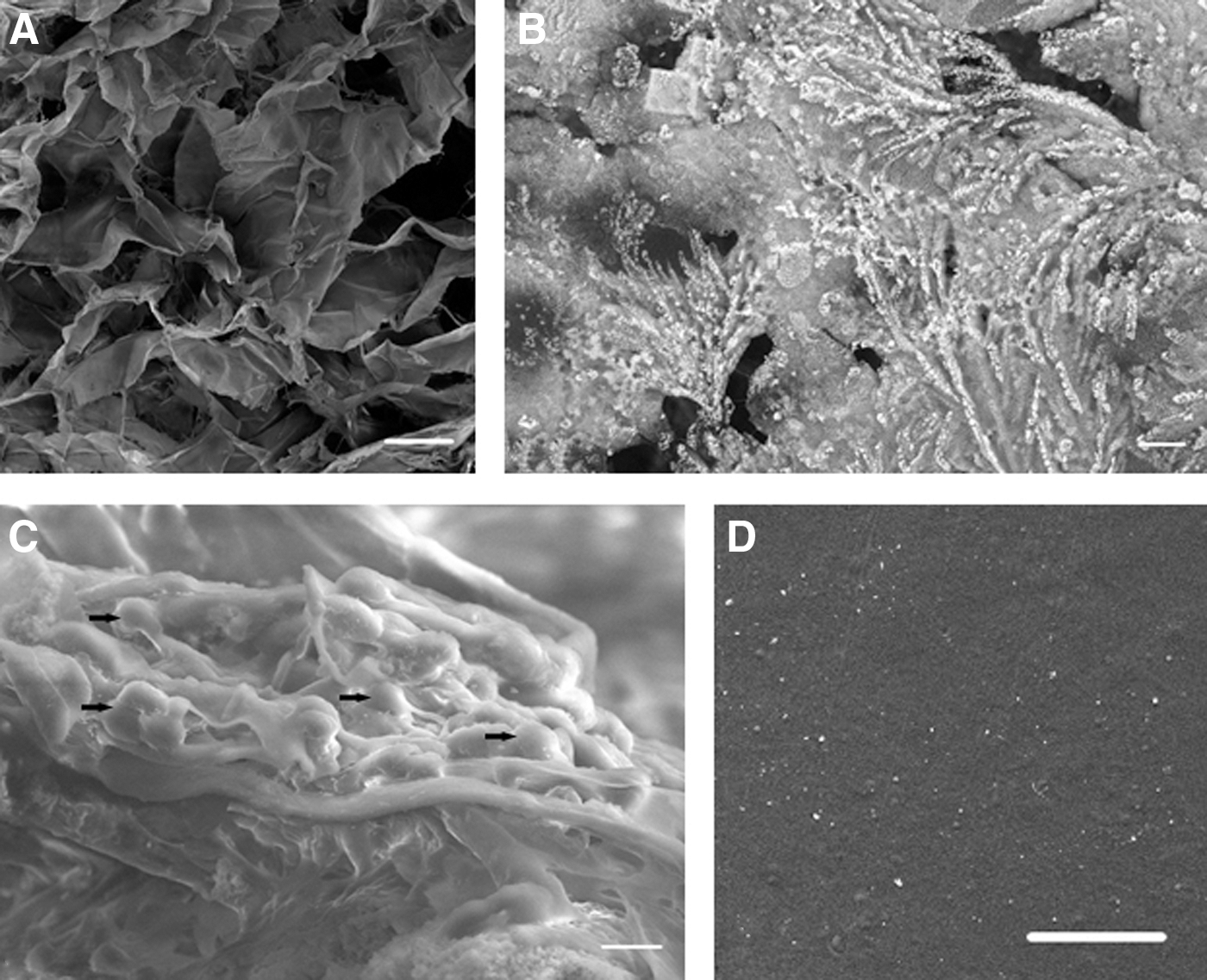
Scanning electron micrographs of biomaterials designed for periodontal tissue engineering.
Besides the polymeric matrix, a major challenge was to mimic the mineralized-phase synthesis [45]. First, it was observed that dense crystalline hydroxyapatite (HA) with good strength, high solubility, and bioactivity could initiate protein adsorption, cell osteogenesis, bone formation, and remodeling [46]. Then, bone ECM proteins, such as collagen, fibronectin, osteopontin, and osteocalcin, were used as scaffolds and suffered in vivo HA mineralization after implantation and interaction with cells [47,48]. Therefore, collagen and fibronectin were incorporated into polymeric or ceramic biomaterials used as grafts [49]. For bone tissue engineering, our group designed 3D composite matrices consisting of both organic compounds (collagen and chondroitin sulfate) and inorganic mineral crystals (HA, tricalcium phosphate—TCP) that promoted higher adhesion of osteoblasts (Fig. 2B, C) [50,51]. A fibronectin–osteocalcin electrospun composite was fabricated to accelerate adhesion of bone marrow derived-stem cells (via fibronectin) and to stimulate osteogenesis and mineralization due to osteocalcin affinity for HA and regulation of crystal growth [52]. In addition to bone repair, construction of a biomineralized cement-like layer was also attempted using amelogenin peptides. These peptides could control HA mineralization and formation of a mineralized layer that allowed adhesion of stem cells from the periodontal ligament [53].
Besides composition, the structure and anatomy of periodontal tissue were lately mimicked in developed biomaterials. An important factor in the development of these biomatrices is related to surface properties because the cells initially recognize surface features and choose a specific pathway, for example, bone formation [54]. There are nanofibrillar matrices designed as scaffolds for cells and/or cell-stimulating proteins [55]. Studies have shown that nanofibrous structures stimulate periodontal and stem cells from alveolar bone or periodontal ligament to synthesize new ECM and contribute to its maturation, even stronger than the microfibrous structure [47]. In addition, our group designed hybrid materials based on natural polymers with surfaces covered by silver nanoparticles for antimicrobial activity against pathogens involved in periodontitis infection (Fig. 2D). We have used positively charged silver nanoparticles prepared in nondenatured collagen, as a reducing and stabilizing agent, which facilitated optimal interaction with negatively charged bacterial cells [56].
3D porous matrices can also be used as scaffolds for transport and delivery of cells of interest. After implantation, the biomaterial–cell constructs stimulate new tissue formation while maintaining proper tissue integrity. Grafts of dental pulp stem cells injected in collagen matrices yielded valuable results in human mandible bone repair [57].
Carrier Matrices
Matrices for bioactive factor delivery
At present, more complex biomaterials are designed to incorporate biologically active factors such as bone morphogenetic proteins (BMPs), enamel matrix derivatives (EMD), and growth factors as a new strategy for therapeutic applications. Both controlled release and protection of biomolecules during the repair process are essential in vivo. The simplest way of fabrication is by compound attachment to the biomatrix surface [58]. This method is effective when rapid release of biomolecules is desired, leading to direct contact with cells and their activation [59]. A method that seems to have even more advantages is incorporation of biomolecules into matrices, but the process efficiency depends on the conditioning type. A combination of micro/nanoparticles encapsulating biomolecules and polymeric biomatrices has been developed as a general method of bioactive compound incorporation [60]. Thus, alginate microspheres encapsulating BMP-6 were incorporated into porous chitosan matrices that allowed controlled release of the biological active compound and stimulation of stem cell osteogenesis in periodontal regeneration [61].
Tissue regeneration is a complex process involving the activity of several growth factors and cytokines. Thus, incorporation of multiple biofactors in biomatrices and their delivery in concentrations higher than physiological ones were achieved for development of efficient therapies of bone regeneration [62]. Administration of two different factors requires individual incorporation into micro/nanoparticles to allow their simultaneous release. Thereby, biomaterials incorporating microspheres containing BMP-2 and insulin-like growth factor-1 (IGF-1) were obtained to facilitate the independent release of growth factors in time [63]. Alternatively, micro/nanocarriers with different release kinetics are used for each biofactor of interest based on variable biodegradability, size, porosity, and permeability of the transporters. It was reported that the use of two types of nanocapsules, consisting of poly (beta-hydroxybutyrate-co-beta-hydroxyvalerate) and PLGA, which resulted in the controlled release of BMP-2, followed by BMP-7, positively influenced bone regeneration [64]. The combination of a nanotransporter for one growth factor with a biomatrix incorporating another growth factor was also tested to rapidly release one factor, while the other one had a long-term release. This approach can be successfully used in periodontal regeneration for the initial delivery of anti-inflammatory mediators, followed by molecules involved in regeneration or angiogenesis, and finally of osteogenic mediators [65].
Autogenic biomatrices
Autogenic biomatrices consisting of bone autografts supplemented with platelet-rich plasma (PRP) and platelet-rich fibrin (PRF) were first used in 1998 to reconstruct bone defects [66]. PRP is defined as a small volume of autologous plasma with a high concentration of platelets and represents an important source of growth factors [67]. In dental clinics, PRP is used as such or combined with bone substitutes for reconstruction of mandibular bone and treatment of periodontal defects and dental alveoli after tooth extraction [47]. Improved results were obtained in continuity defects, sinus lift augmentation grafting, horizontal and vertical ridge augmentation, and ridge preservation grafting [68]. PRP injections were also used for the musculoskeletal system treatment, to promote muscle healing of acute muscle injuries [69] and knee osteoarthritis [70], to allow earlier implants in osteoporotic bone, and to enhance soft tissue mucosal and skin healing [68], but clinical trials are necessary to validate these applications in terms of efficacy.
PRP is a low-cost product, highly available and stable for 8 h when mixed with anticoagulant. Its mechanic strength is low, which makes it hard to manipulate during implantation. The growth factors are quickly released and this might limit the degree of bone regeneration stimulation [71]. There are many studies on the positive effect of PRP in periodontal regeneration [72,73] and reports on its limited effect [74], but the latter could be due to the quality of the used PRP. The positive effect of PRP on bone regeneration is believed to be due to growth factors, such as IGF-1, platelet-derived growth factor, transforming growth factor-β, fibroblast growth factor, epidermal growth factor, vascular endothelial growth factor, and blood proteins (fibrin, fibronectin, and vitronectin), acting as osteoconductive adhesion molecules [71].
PRF was first obtained in 2001 [75] and is considered the second generation of platelet concentrate, useful for stimulation of tissue repair [76]. It is a natural biomaterial of fibrin enriched with platelets, containing besides the growth factors from PRP, the tumor necrosis factor α and cytokines such as interleukin-1β, interleukin-6, and interleukin-4. Its advantages over PRP are the availability, easy to obtain and apply, low cost, and lack of anticoagulant need. PRF can be used as a clot or membrane and manipulation is easy due to its elasticity and strength [71]. Bone regeneration was observed after using PRF and an allograft of demineralized bone matrix (DBM) [77] or PRF in combination with bioactive glass for root cysts [78]. PRF was also shown to stimulate proliferation of osteoblasts, cells of periodontal ligament, and gingival fibroblasts, indicating its ability in periodontal regeneration [79]. A dense matrix made of PRF was used as a membrane in GTR to protect and stabilize the bone graft at the implant situs and positive results were obtained in the treatment of intrabony defects [80 –82].
Demineralized bone matrix
DBM was tested in preclinical and clinical studies for osteoconductivity, osteoinductivity, and ability to form bone tissue [83]. At present, DBM is frequently used in periodontal treatments for bone regeneration. Commercial DBM in combination with EMD, BMP-2, PRP, and PRF was successfully tested in periodontal regeneration [47]. Similarly, demineralized dentin was shown to stimulate proliferation and differentiation of periodontal ligament cells due to growth factors. Demineralized dentin in combination with exogenous growth factors, such as BMP-2, resulted in cement formation, stimulating periodontal regeneration [84].
Cellular Biomatrices
Stratified cellular biomatrices
Fabrication of cell monolayers represents a technique of great potential among tissue engineering strategies, developed as an alternative to cell injection [85]. Cell monolayers are prepared on the temperature-responsive surface of culture plates, which allow their noninvasive takeover along with the synthesized ECM or by techniques involving magnetic forces or polyelectrolytes [86,87]. Due to their fragile structure and challenging periodontal implantation, cell monolayers were associated with biomaterials or used as multistratified structures. Thus, a biomatrix of β-TCP and multiple cell sheets of periodontal ligament cells had osteoblastic/cementoblastic differentiation abilities in vitro and positive clinical results of periodontal regeneration in a three-wall intrabony defect in a dog [88]. A trilayered composite made of a bone component enriched with calcium phosphate and a periodontal component made of electrospun polycaprolactone (PCL) conferred stability to multiple cell sheets of osteoblasts, which adhered, filled scaffold pores, and secreted mineralized matrix after 3 weeks of cultivation in osteogenic induction medium [89]. The composite presented high osteoinductivity in vitro and the combination with cell sheet technology improved bone mineralization, vascularization, and periodontal adhesion to dentin in vivo [90]. Stratified cellular biomatrices were tested on animal and human periodontal defects to analyze both their safety and efficiency in preclinical studies (Table 2).
Stratified Cellular Biomatrices and Preclinical Studies on Periodontal Regeneration
3D, three-dimensional; HA, hydroxyapatite; MSC, mesenchymal stem cell; PCL, polycaprolactone; PLA, polylactic acid; PLGA, poly (lactic-co-glycolic acid); PRF, platelet-rich fibrin; TCP, tricalcium phosphate.
Mechanically stimulated cellular biomatrices
Recently, the potential of mechanical stimuli on tissue repair and regeneration was reported, including periodontal tissue. Mechanical forces affect functions of the periodontal ligament and alveolar bone, activate tissue remodeling, and lead to bone resorption [47]. In vitro studies showed that mechanical stress stimulated osteogenic differentiation of stem cells derived from dental pulp, alveolar bone, or periodontal ligament [103]. Due to its complex structure, periodontal tissue regeneration depends on controlled activation and integration of stem cell function to the local milieu. Several studies on mechanical stimulation of stem cells showed major differences between 2D and 3D cultures [104]. They indicate the need for additional analyses to investigate interactions between cells under mechanical stress in an environment similar to native tissue. For this, stem cells loaded in biomimetic matrices were mechanically stimulated and differentiated before implantation and the results recommended this procedure as the next level in periodontal tissue engineering [47]. Besides, stimulation of human mesenchymal stem cells (MSCs) with low-intensity pulsed ultrasound treatment increased cell colonization of composite materials [105] and in vivo osteogenic differentiation in a rabbit bone–tendon fracture microenvironment, at 16 weeks postoperative [106]. Shear stress and cyclic hydrostatic pressure applied to human MSCs isolated from bone marrow promoted cell differentiation and obtaining of functional cells for tissue engineering [107].
3D Printed Biomatrices for Bone Grafting
Development of the rapid prototyping technique allows creation of 3D printed matrices customized for each osseous defect [108]. Computed tomography scan of the periodontal defect generates an image that is converted to a digitalized format using computer-aided design. Architecture of the scaffold such as precise external shape and properties such as porosity and pore size can be tailored to improve the implant effect on new tissue formation using computer-assisted manufacturing technologies. Printers based on several techniques [109] place polymeric biomaterials of variable viscosities, layer by layer, to build 3D structures [110]. PCL is mainly used for printing constructs with applications in periodontal tissue regeneration [111]. These 3D printed matrices with controlled physicochemical characteristics showed promising results in space preservation, control of tissue infiltration, and cell homing compared with random porous scaffolds [112].
The major challenge in periodontal regeneration is now the hierarchic formation of multiple interfaces for alveolar bone maturation, periodontal ligament orientation, and tissue integration. Thus, multiphasic matrices were fabricated by 3D printing based on PCL and HA with a 100-μm microchannel compartment for dentin cement, 600-μm microchannel compartment for the periodontal ligament, and 300-μm microchannel compartment for alveolar bone [113]. Its ectopic implantation in mice for 4 weeks, together with encapsulated bioactive cues and dental pulp stem cells, resulted in integrated tissues. Biphasic, solid porous biomaterials were achieved by fused deposition modeling [89]. They were designed with β-TCP as the bone component and PCL microfibrous membrane as the periodontal component to allow simultaneous transport of two cell types (stem cells and osteoblasts) for regeneration of the alveolar bone–periodontal ligament complex. In vitro studies showed that the bone compartment stimulated osteoblast growth and mineralization of the ECM, while the periodontal compartment was cultivated with multiple sheets of periodontal ligament cells. A 3D printed scaffold of PCL was combined with a flexible electrospinning membrane of osteoconductive calcium phosphate and cell sheet technology [90]. After implantation, using an ectopic rat model, the biphasic scaffold led to alveolar bone formation and periodontal attachment.
A space-oriented periodontal ligament has an important role in exercising its mechanical function over occlusal or masticatory forces. 3D printing technology has made possible the design of a biomaterial mimicking the periodontal ligament structure, which allows dental roots to anchor in the alveolar bone and successfully guides the perpendicular and oblique orientation of the connective tissue regenerated fibers [114]. Its implantation resulted in bone tissue formation, periodontal ligament orientation, and cementogenesis on the root surface, as well as functional regeneration of the periodontal complex. Synthetic copolymers of PCL-PGA were used to fabricate scaffolds with perpendicular microchannels by the additive manufacturing procedure to allow in vivo functional orientation of the periodontal ligament [115].
Future Research and Applications
All these encouraging results require further development of complex tailored biomaterials for periodontitis treatment and their testing in numerous in vitro and in vivo preclinical studies. Additional studies for composition–structure optimization and tailoring new biomatrices for dentistry applications are necessary before clinical tests on humans. The designed composite materials are useful for development of bioactive implants, containing dental cells, for periodontal tissue engineering. Future studies regarding osteoblast activity and differentiation and synthesis of ECM components using in vivo experimental models are required to examine the bioactive implant's ability to induce bone defect repair. In addition, more biotechnological researches on fabrication of bioactive implants and their inflammatory reaction after implantation are needed. All these novel procedures and techniques promise development of future therapeutic protocols.
Footnotes
Acknowledgments
This work was supported by the Ministry of Research and Innovation, CNCS-UEFISCDI, project no. PN-III-P4-ID-PCE-2016-0715 within PNCDI III. The authors thank Prof. Dr. Cristian Matei from the University Politehnica of Bucharest, Faculty of Applied Chemistry and Materials Science, for scanning electron microscopy (SEM) image acquisition.
Author Disclosure Statement
All authors disclose that there are no commercial associations that might create a conflict of interest in connection with this article. No competing financial interests exist.