
Abstract
The pathological processes developing after spinal cord injuries often lead to formation of cysts. Existing surgical and medical methods are insufficient for treatment of post-traumatic spinal cord cysts. One of the emerging tools is cell therapy. Olfactory ensheathing cells (OECs) are perspective cells for cell therapy. In this study, we demonstrated that human OEC transplantation is effective in experimental spinal cysts. For our experiments, we selected animals only at the intermediate stage of recovery with scores from 8 to 13 according to the Basso, Beattie, and Bresnahan (BBB) scale. Cells were transplanted in different quantities (0.75 and 1.5 million) into the fully formed cysts and in the areas of injury without cysts. Improvement of limb mobility after human OEC transplantation into post-traumatic cysts was shown. In the group of rats with cysts, time-dependent increase in the BBB score was observed in subgroups treated with 0.75 and 1.5 million OECs with no statistically significant time-dependent dynamics of BBB values in the control group. When all three subgroups (control and two OEC doses) were compared, the Kruskal–Wallis test showed the presence of differences between subgroups after 1, 3, and 4 weeks of treatment with evidence of divergence increase. There was no statistically significant difference between the two doses of OEC treatment. The human OECs in the experiments without cysts were not effective. It was also shown that PKH26-labeled human OECs survive throughout the experiment and migrate to nearby areas of the cyst. Therefore, it was found that it is effective to transplant human OECs into fully formed cysts. In the future, autologous OECs can be used to personalize the treatment of patients with spinal cysts.
Introduction
The number of patients with spinal cord injuries is increasing every year. A serious problem of neurosurgery is post-traumatic cysts of the spinal cord. Over time, cysts can grow in size, squeeze the spinal cord, and prevent spinal cord regeneration and normal conduction of impulses to the limbs [1]. Post-traumatic cysts represent a great danger to the life of patients. Thus, motor and sensory functions and normal circulation of the cerebrospinal fluid are disrupted. Dysfunction of pelvic organs, respiratory depression, and chronic pain were also observed [2]. It has recently become obvious that the problem of regeneration of the spinal cord after injuries can be solved with the help of cell therapy. It has been shown that cell transplantation can promote axon regeneration and help to replace lost neurons [3].
Different cell types were used for cell therapy of spinal cord injuries: stem cells [4], induced pluripotent cells [5 –7], mesenchymal stem cells [8,9], and Schwann cells [10]. Although improvement of sensory and motor functions of the spinal cord after cell therapy has been shown, in many cases, the application of some types of cells was ineffective or gave rise to side effects such as formation of teratomas [11] or the occurrence of neuropathic pain [12]. In addition, treatment with some cell preparations caused certain methodological and ethical problems. All these problems make it difficult to select cells for transplantation in spinal cord injuries.
The solution to all of the above problems can be transplantation of human olfactory ensheathing cells (OECs). At the same time, obtaining OECs is an easy and nontraumatic procedure for patients with a spinal cord injury. After growing in a cell culture, autologous transplantation is possible. Personalized medicine is an important approach in treating patients.
The lamina propria of olfactory mucosa of the nose can serve as a source of OECs. It has been proved that these cells have regenerative potential after spinal cord injuries [13,14]. These cells simultaneously possess the properties of astrocytes and Schwann cells and express an astrocytic marker—glial fibrillary acidic protein—and oligodendroglial marker—low-affinity nerve growth factor receptor (p75NTR). OECs can participate in remyelinating nerve fibers, such as Schwann cells, and create a microenvironment for neurons and promote the growth of axons, such as astrocytes [15].
A plethora of experimental studies concerning application of OECs have been performed [16,17]. It was found that transplantation of cultured adult OECs into lesions leads to regeneration of axons in long fiber tracts [18,19] and regeneration of dorsal root axons entering the spinal cord [20]. OEC transplants have been shown to improve both motor and sensory functions [21 –25]. However, there are disagreements between different scientific groups regarding application of OECs for spinal cord injury rehabilitation [26,27]. Various treatment protocols have been used for OEC transplantation in spinal cord injuries. They differed in the injury phases when OECs were applied and the location of injuries, in graft types and donor species, numbers and sources of transplanted cells, and usage of antibiotic and immunosuppressive agents. These differences can significantly affect the results.
To summarize studies concerning the influence of OEC transplantation on motor function recovery in animal models, Nakhjavan-Shahraki et al. designed a meta-analysis [27], which analyzed data from 933 animals (control group = 464 and treatment group = 469). It was convincingly proved that OEC transplantation can significantly increase motor function after spinal cord injury. It should be noted that numerous positive effects of these cells were obtained precisely in the acute or subacute phases. OEC transplantation in the chronic phase of spinal cord injury remains poorly understood, and nothing is known about the effects of OECs after transplantation into spinal cysts. The purpose of this work is to determine the efficiency of the human OEC transplantation into spinal cord cysts to improve mobility of hind limbs.
Materials and Methods
Materials
Reagents of analytical grade were received from Sigma-Aldrich and Thermo Fisher Scientific. The reagents and plastic for cell culture were obtained from HyClone and Corning, Inc.
Cell culture
Samples of the human olfactory mucosa (total area 5–25 mm2) from superior nasal meatus were obtained from patients during planned surgical interventions at the Department of Plastic Surgery, University Clinical Hospital No. 1 (I.M. Sechenov First Moscow State Medical University, Moscow, Russia). All patients signed an informed consent form. The experimental protocol was approved by the Ethics Committee of N.I. Pirogov Russian National Research Medical University. During the research, all ethical principles in line with the Helsinki Declaration were followed. The tissue was washed in DMEM/F-12 (1:1). After that human OECs were obtained according to the previously developed method [28].
Modeling of post-traumatic spinal cysts
Animal experiments were carried out according to the principles of the International Laboratory of Animal Care and approved by the Ethics Committee of N.I. Pirogov Russian National Research Medical University. Post-traumatic spinal cysts were modeled in mature female Wistar rats (body weight 200 g) by the method developed at the Department of Fundamental and Applied Neurobiology, V.P. Serbsky National Medical Research Center for Psychiatry and Narcology [29].
Rats were narcotized by intraperitoneal injection of ketamine and diazepam (100 and 5 mg/kg of body weight, respectively), and then a median incision along the spine and partial resection of the muscles on both sides of the spinous processes were perfomed at the Th9–Th10 level. To access the spinal cord, the Th10 spinous process was removed with surgical nippers. Contusion injury was caused using an impactor device with a force of 200 kdyn (Precision Systems and Instrumentation LLC, Fairfax, VA). The rats were injected intramuscularly with cefazolin (300 μL per rat, 1 g cefazolin solution per 4 mL water for the injection) immediately after the operation, the next day, and further once a week. Cyst formation was confirmed by magnetic resonance imaging (MRI) (ClinScan; Bruker BioSpin) 4 weeks after surgery. In our experiments, rats without cysts 4 weeks after surgery were used as a comparison group with chronic spinal cord injury.
We also used MRI to evaluate the cyst volumes before transplantation of different numbers of cells and 4 weeks after transplantation.
Transplantation of human OECs
The 3–4 passages of human OECs were transplanted into the area of spinal cord injury in inoculation doses of 0.75 million cells (rats with cysts n = 10, rats without cysts n = 10) and 1.5 million cells (rats with cysts n = 11, rats without cysts n = 9) in 15 μL of DMEM/F-12 Dulbecco's modified Eagle medium F-12 medium (1:1). In the control group (rats with cysts n = 11, rats without cysts n = 12), the same volume of medium without cells was injected.
The animals were narcotized intraperitoneally with ketamine and diazepam (100 and 5 mg/kg of body weight, respectively) and cells were transplanted at a rate of 40 μL/min with an injector. To eliminate complications associated with inflammatory processes, the rats were injected intramuscularly with cefazolin (300 μL per rat, 1 g cefazolin solution per 4 mL of water for the injection) immediately after cell transplantation.
Basso, Beattie, and Bresnahan test for evaluating the recovery of motor function
The main instrument for evaluating the recovery of motor function is the 21-point open-field scale developed by Basso, Beattie, and Bresnahan (BBB), which allows studying the dynamics of recovery of the musculoskeletal system, considering the early stage (BBB score from 0 to 7), intermediate phase (8–13), and late phase (14–21) of recovery [30]. The motor activity of hind limbs of rats was evaluated before cell transplantation. For further experiments, we selected rats only at the intermediate stage of recovery with scores from 8 to 13 by the BBB scale. After cell transplantation, we evaluated the motor activity of hind limbs of the rats during a period of 4 weeks.
Study of viability of human OECs in spinal cysts
To study the viability of human OECs in the cysts, four passages of PKH26-labeled OECs were injected into the area of spinal cord injury in the inoculation dose of 1.5 million cells in 10 μL of DMEM/F-12 medium (1:1) (PKH26 Red Fluorescent Cell Linker Kit for General Cell Membrane Labeling was obtained from Merck/Sigma-Aldrich). In the control group, the same volume of medium without cells was injected. Four weeks after OEC transplantation, rats were anesthetized with ketamine and diazepam (100 and 5 mg/kg body of weight, respectively) and 4% paraformaldehyde in 0.1 M phosphate buffer was used for perfusion. The sections of the spinal cord with cysts were obtained. The thickness of the sections was 40 μm. Next, the immunofluorescence method was applied [31].
To visualize the spinal cord tissue, primary antibodies against the mature neuronal marker b-III-tubulin (1: 300) and secondary antibodies labeled with Alexa Fluor 488 (1: 500; Molecular Probes) were used, visualization of nuclei was performed with 4′,6-diamidino-2-phenylindole. The preparations were analyzed under a laser scanning confocal microscope with a multiphoton module, Nikon A1 MP (Japan). Images were processed using NIS-Elements (Japan). Data were obtained in three independent experiments.
Statistical analysis
Statistical analysis was performed using Statistica 6.0 (StatSoft) and Microsoft Excel 2007 (Microsoft). The data are presented as mean ± standard deviation. Because of the sample sizes, we preferred nonparametric tests. The time dependence of BBB score dynamics in different groups (ie, control and two doses of OECs) was studied with the Friedman test. For multiple comparisons at given time points, we used the BBB score normalized to the initial BBB value. Comparisons were made with the Kruskal–Wallis test and Dunn's test adjusted for rank ties. For graphic representation, we also subtracted the BBB scores at given time points from initial BBB values and then also normalized the difference to initial BBB values. The data of two experiments (rats with cysts and rats with no cysts) were calculated separately.
Results
Modeling of post-traumatic spinal cord cysts
Post-traumatic spinal cord cysts were modeled in the mature female Wistar rats by the approach developed at our Department. Formation of cysts in the rat spinal cord was proved by MRI 4 weeks after postcontusion injury (Fig. 1, upper). In rats without cysts 4 weeks postsurgery, the area with the spinal cord injury is exhibited (Fig. 1, lower).
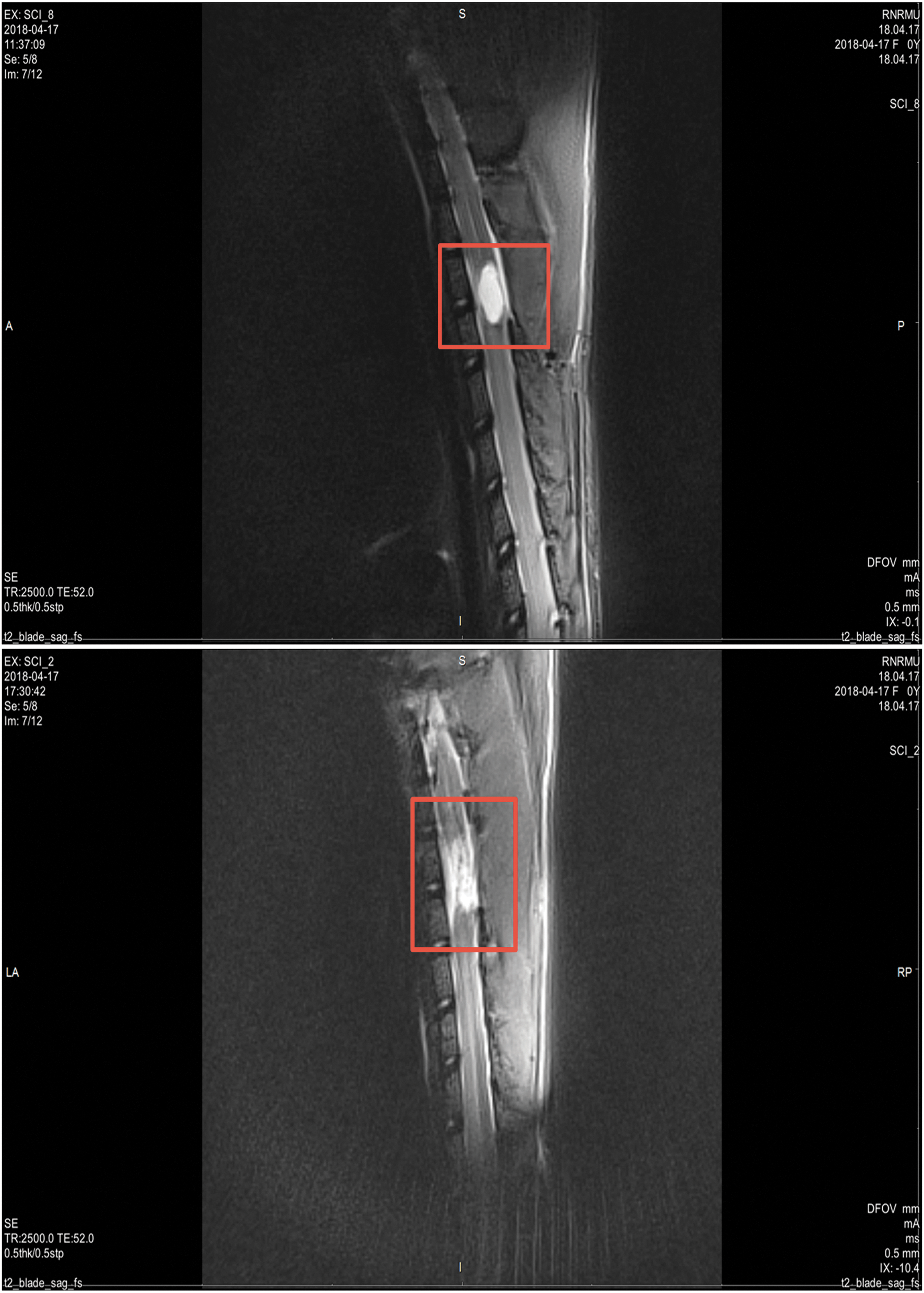
Areas of post-traumatic injury (marked in red). Upper: the post-traumatic cyst of spinal cord 4 weeks postsurgery, cyst is a white oval formation, MRI, lower: the spinal cord injury without cyst 4 weeks postsurgery, MRI. MRI, magnetic resonance imaging.
The study of the efficiency of human OEC transplantation into spinal cysts
For further experiments, we selected rats with the presence or absence of cysts that had severe disturbances in hind limb movements only at the intermediate stage of recovery with scores from 8 to 13 according to the BBB scale.
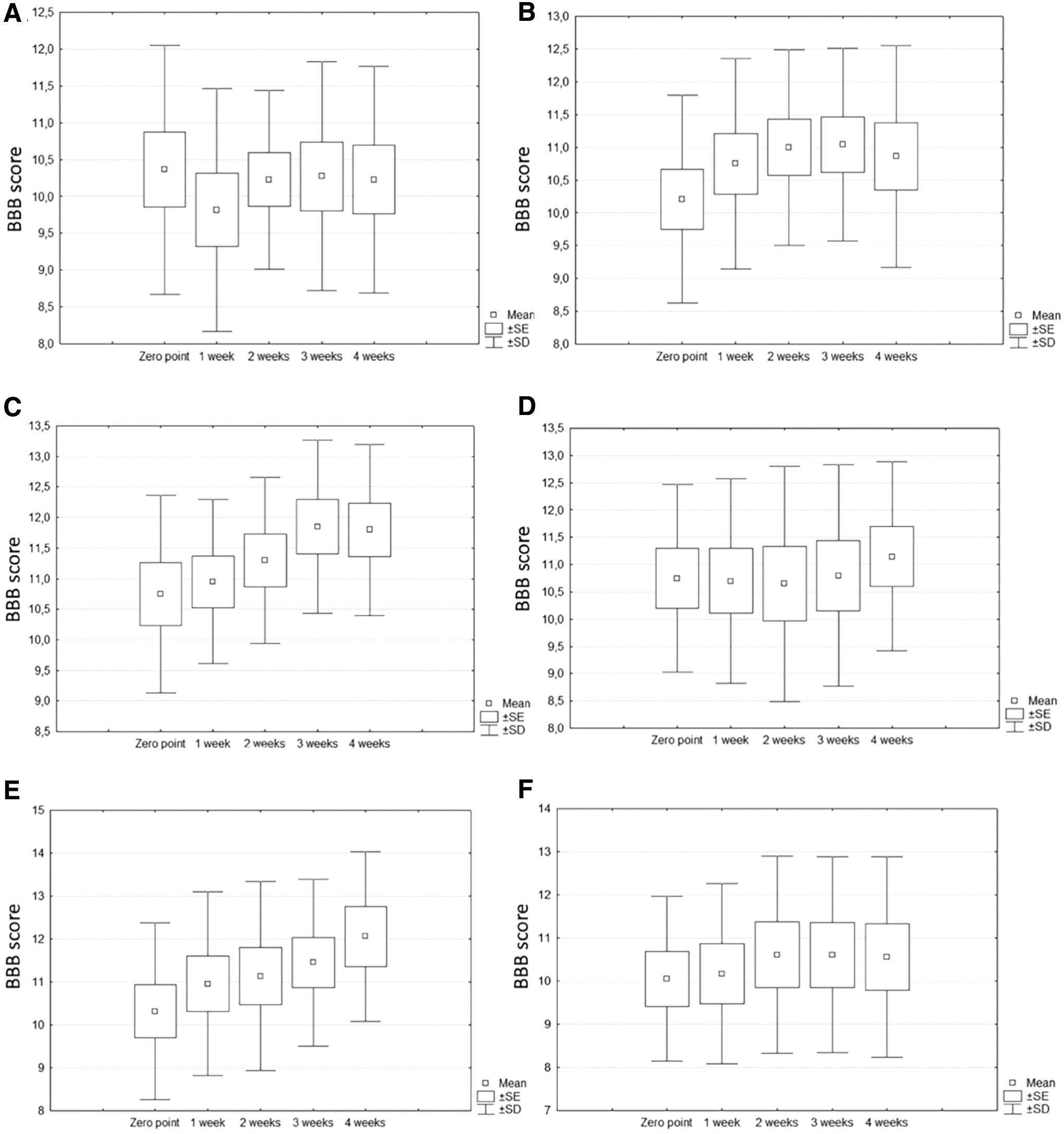
In the group of rats with cysts, the time-dependent increase in BBB score was shown in subgroups treated with 0.75 million OECs (χ 2 = 17.5, P < 0.01) and 1.5 million OECs (χ 2 = 13.93, P < 0.01), respectively, with no statistically significant time-dependent dynamics of BBB values in the control group ( χ 2 = 3.69, 0.25 < P < 0.45). In the second experiment (rats without cysts), we could not find any time-dependent changes in BBB scores of rats, regardless of being injected with OECs or sham treated (Fig. 2).
Dynamics of BBB status in rats with cysts
As mentioned above, the presence of positive BBB dynamics in rats with cysts could afford us the opportunity to suggest a positive effect of OEC injections. When all three subgroups (control and two OEC doses) were compared, the Kruskal–Wallis test showed the presence of differences between subgroups after 1 week (H = 6.79, P < 0.05), 3 weeks (H = 6.23, P < 0.05), and 4 weeks (H = 8.75, P < 0.05) of treatment with evidence of divergence increase. There was no difference after 2 weeks of treatment (H = 3.43, P = 0.18). The latter fact could be explained by transient efficacy of OECs in the beginning of treatment. As for Dunn's test, the strongest evidence of difference was shown between the group of 0.75 million OECs and the control group after 4 weeks of treatment (Q = 2.75, P < 0.05).
Although a higher dose of OECs also showed some apparent efficacy, there was only a tendency, although almost reaching statistical significance (Q = 2.2, critical value of Q = 2.24). There was no statistically significant difference between the two OEC treatment regimens (Fig. 3, upper).
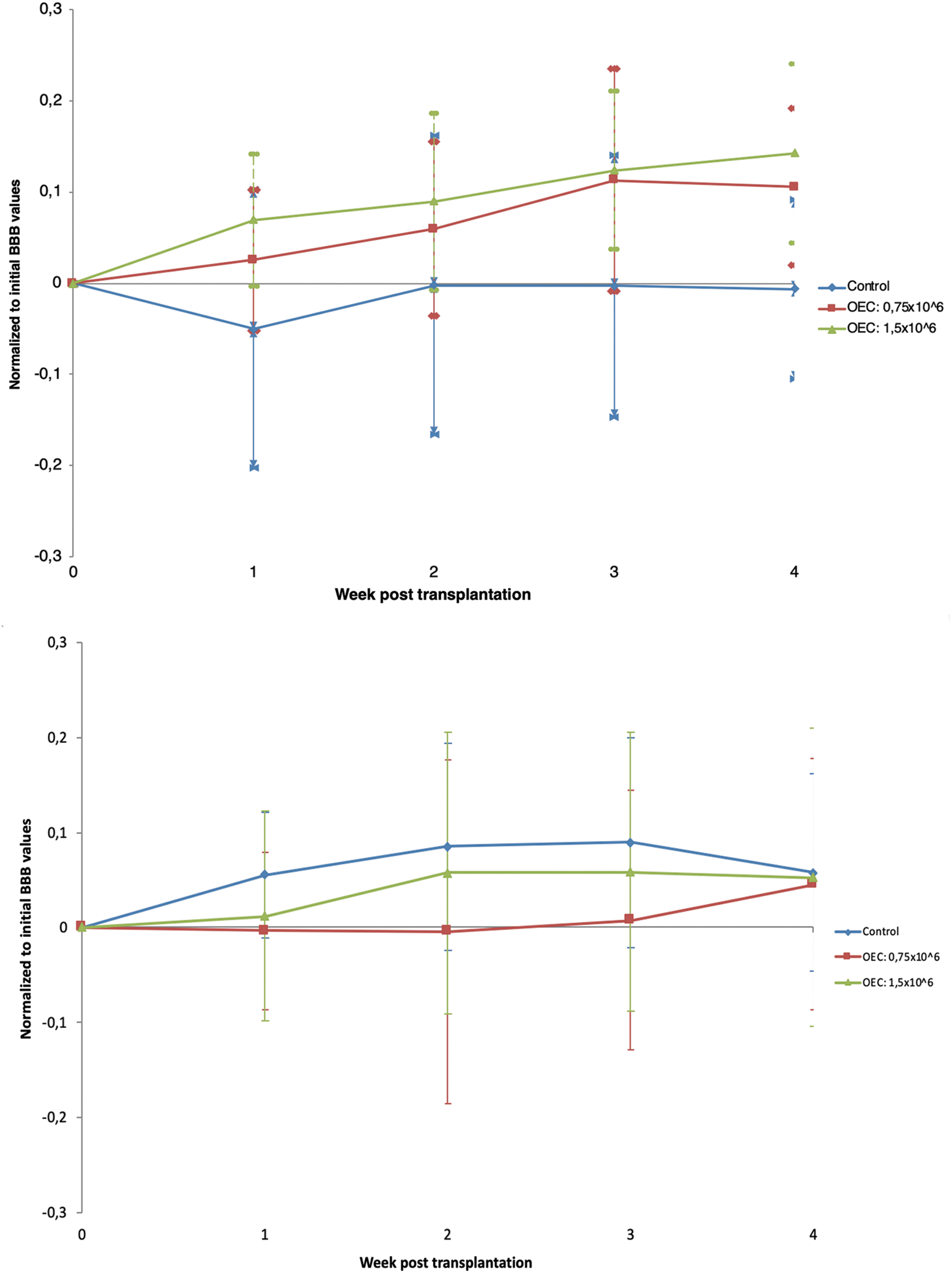
The time-dependent changes in BBB status normalized to initial BBB values. Upper: rats with cysts: the differences are shown between control and OEC treatment groups (0.75 and 1.5 million OECs) after 1 week (H = 6.79, P = 0.034), 3 weeks (H = 6.23, P = 0.045), and 4 weeks (H = 8.75, P = 0.0126) of treatment. The strongest evidence of difference is shown between the group of 0.75 million OECs and the control group after 4 weeks of treatment (Q = 2.754, P < 0.05). There was no statistically significant difference between the two OEC treatment doses. Lower: rats without cysts: there was no statistically significant difference between control and OEC treatment groups.
In the second experiment (rats without cysts), there was no difference between control and OEC treatment groups according to the Kruskal–Wallis test, which showed a mild tendency toward significance after 2 weeks (H = 5.01, P = 0.08). Interestingly, in this experiment, the BBB score in control groups tended to be higher than in OEC groups, with the most powerful (although not significant) Dunn's test values observed after 2 weeks of treatment when comparing the control and 0.75 million OEC treatment (Q = 2.23, critical value of Q = 2.24). Therefore, in control rats without cysts and animals receiving 0.75 and 1.5 million cells, the dynamics of locomotor recovery did not significantly differ. The therapeutic effect of the human OEC transplantation was therefore not observed. There was an improvement in all three groups apparently associated with the self-regeneration capacity of the spinal cord (Fig. 3, lower).
It is interesting to note that some animals with cysts show decrease of the cyst area at the fourth week after 0.75 million human OEC transplantation (Fig. 4C, D) and some animals show the disappearance of cysts at the fourth week after 1.5 million OEC transplantation (Fig. 4E, F). However, when reliable average values of cyst volumes in the entire sample of animals were accessed, differences in the sizes of cysts before and after cell transplantation were not detected (data not shown). Apparently, it is possible to speak only of the individual abilities of rats to regenerate when in some animals after the cell transplantation cysts decrease in size or even completely disappear.

Visualization of post-traumatic spinal cord cysts by MRI before
The study of viability of human OECs in cysts
To study the viability of transplanted human OECs in cysts, cells were labeled with PKH26. We found that human OECs survive in the spinal cord 4 weeks after transplantation. The labeled cells were found in tissues of the spinal cord near the cyst area (Fig. 5). In the control group, staining in the red channel was not detected (Fig. 6).

Viability of human OECs at the fourth week after cell transplantation.
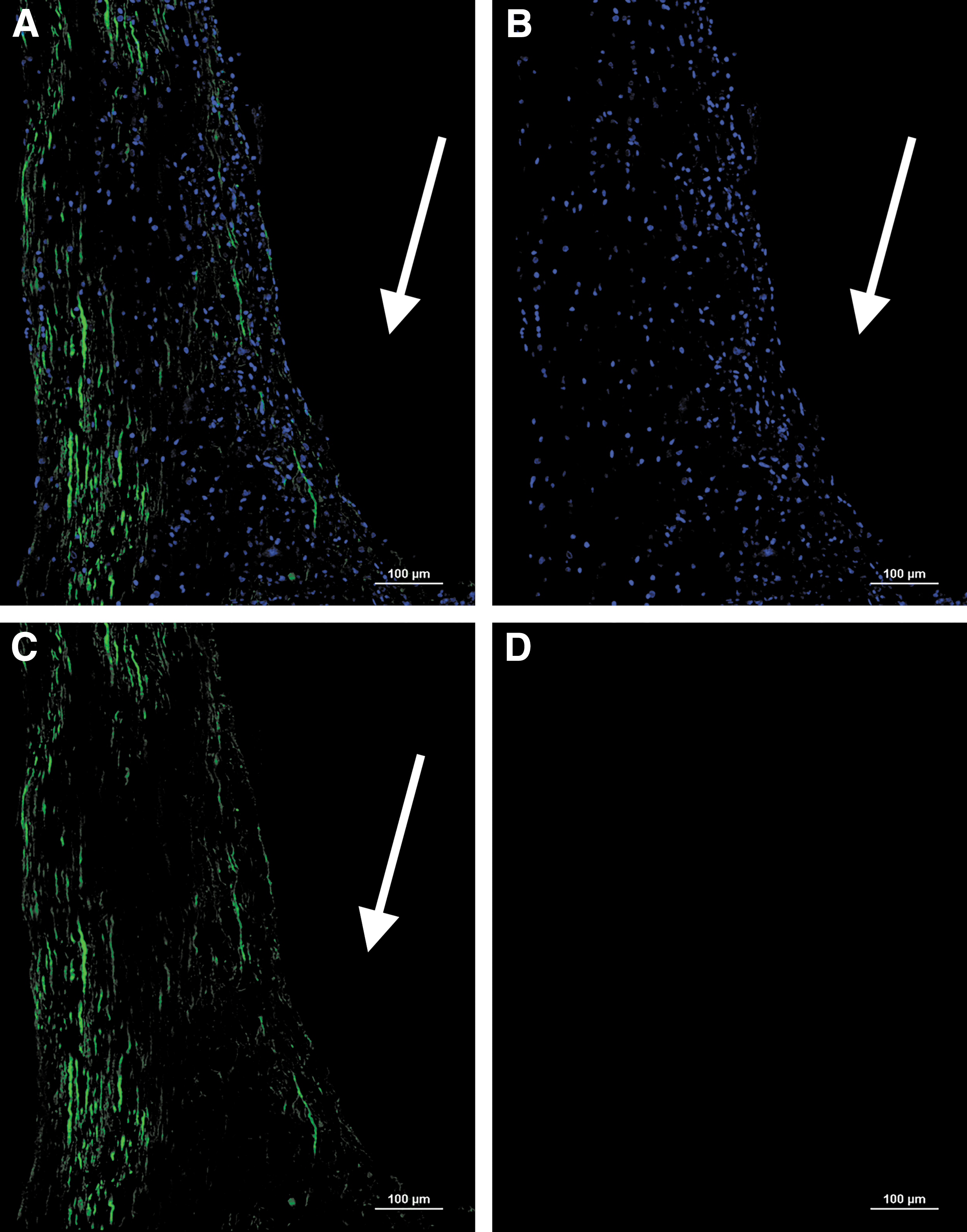
In the control group without cells, staining in the red channel was not detected.
Discussion
In this study, we first showed the efficiency of transplantation of human OECs into experimental spinal cysts. To achieve this result, we optimized the existing protocols of obtaining OECs from the human and rat olfactory mucosa [18,32,33] to obtain more pure culture of human OECs in amounts sufficient for further cell therapy [28]. Efficacy of OEC transplantation varies between researches. The main reason for this variability is the purity and phenotype of transplanted cells [26,34]. Development of methods for obtaining pure OEC cultures is necessary for correct evaluation of their effectiveness. It should be noted that the number of passages of cell cultures is a critical parameter for obtaining effective cell preparation [35]. In our previous study, it was shown that the 3–4 passages of human OECs are especially enriched by OECs [28].
Many authors in their experimental works show that axonal regeneration, remyelination of nerve fibers, and reduction of the area of damage occur during transplantation of OECs [36,37]. Numerous positive effects of OECs were obtained in acute and subacute phases of the spinal cord injury. In the chronic phase of injury, the use of cell therapy is not so effective [38 –40]. We performed cell transplantation at the fourth week after spinal cord injury. In this period after a rat spinal cord injury, the chronic phase starts [17]. The cell therapy performed in the chronic phase of the spinal cord injury without cysts was inefficient. There is an improvement in all three groups (ie, control and transplantation of 0.75 and 1.5 million cells), which may occur due to self-regeneration of the spinal cord. Neural stem/progenitor cells have been found in the spinal cord of adult mammals, which can provide such regeneration [41].
Mostly, human OECs were assessed in clinical studies on patients with spinal cord injury. The use of human OECs in spinal cord injuries is safe [42] and effective for patients [43,44]. There are a number of studies of human OECs in rat experimental models. Therefore, it was shown that human OECs can affect transplant-mediated remyelination of axons after demyelinating lesions [45,46]. OECs from human olfactory mucosa were similar to rat nasal OECs in proliferation, survival, and migration after transplantation into the rat spinal cord [47]. OECs from human olfactory mucosa had a therapeutic effect after transplantation into the transected rat spinal cord [18,21]. Six weeks after human OEC transplantation in rats with acute spinal cord injury, there was a greater functional improvement in the hind limbs than in control groups, and histological analysis showed a decrease in lesion volume and cavities inside the lesion [48].
Since the rat model of spinal cord injury reflects the main aspects of damage of the human spinal cord, studies of human cells in a rat model are relevant. We believe that as in other areas of regenerative medicine, the work on experimental models with human cells is extremely important since this approach makes it possible to move quickly from preclinical studies to clinical trials. In our work, the efficiency of human OEC transplantation in rat spinal cysts was first shown. In animals receiving 0.75 and 1.5 million cells, there is a positive dynamic in the recovery of motor activity after 1, 3, and 4 weeks.
Spinal cord post-traumatic cysts are filled with a cerebrospinal fluid containing various cell elements and debris and are surrounded by a glial capsule at the chronic stage [49]. The positive observations that we obtained may be related to the phenomenon that the transplanted cells were surrounded and therefore protected by a capsule of a cyst. The cyst capsule creates an additional physical barrier whereby the immune response decreases and the survival of transplanted cells improves. To date, there are many publicly available studies that involved encapsulation of transplanted cells into the immunoprotective barriers. Encapsulation relies on a physical barrier between the graft and host for immunoprotection and therefore may be most suitable for host health and graft function [50].
The human OECs survive during the whole experiment and their migration from the cyst cavity is possible. As known, transplanted OECs can migrate through the glial scar and thus facilitate axonal growth during regeneration [51]. The positive dynamics of recovery of motor activity in hind limbs of rats can reflect regenerative processes in the spinal cord after transplantation of OECs into the region of post-traumatic cysts. So far, the main mechanisms were proposed to explain how OEC therapy can stimulate regeneration of the nerve tissue such as remyelination of nerve fibers restoring nerve conduction in the site of injury and neuroprotective effects of neurotrophic factors secreted by transplanted cells. Overall, these soluble factors promote survival of neurons, growth of their axons, neural plasticity, and regeneration of the spinal cord [16].
In this and previous studies, we have shown that OEC transplantation into experimental spinal cysts improves mobility of the hind limbs of rats. We obtained our data using xenogeneic cell transplantation. Perhaps autologous OECs from patients will have an even more pronounced effect on spinal cysts. Further research in this area will help to develop a combined use of cell therapy with surgical and therapeutic strategies for the treatment of spinal cysts.
Footnotes
Acknowledgments
The study was supported by the Russian Science Foundation (grant no. 17-15-01133: Study of the therapeutic effect of neural stem/progenitor and olfactory ensheathing cells from the olfactory mucosa in experimental spinal cord injury). The authors thank Dr. E.V. Voznykovskaya (Department of Basic and Applied Neurobiology, V.P. Serbsky National Medical Research Center for Psychiatry and Narcology, Moscow, Russia) for the care and veterinary monitoring of the animals and Dr. P.A. Melnikov and PhD student D.A. Vishnevskiy (Department of Basic and Applied Neurobiology, V.P. Serbsky National Medical Research Center for Psychiatry and Narcology, Moscow, Russia) for the support in microscopy.
Presented at the International Congress Biotechnology, State of the Art and Perspectives, February 26-27, 2019, Moscow, Russia.
Author Disclosure Statement
No competing financial interests exist.