
Abstract
Stem cell-based therapies have the potential to heal burn wounds, but thus far have had limited success in clinical practice. This study aimed to test and improve the therapeutic effects of adipose-derived stem cells (ASCs) on burn wound healing in a rat model. We also explored the role of ASCs in burn wound healing We first isolated the autologous ASCs of each Sprague–Dawley rat used in this experiment and expanded them in vitro. Then, a 2-cm2 burn wound was made on the dorsal skin of each rat using a specialized heating iron. The treated rats received either one or three injections of 2 × 106 green fluorescent protein-labeled autologous ASCs, and the control rats received injections of the same volume of phosphate-buffered saline. A digital camera was employed to capture images of the wound area. We explored the role of ASCs in burn wound healing by cell tracing, evaluation of blood vessel number, analysis of a rat cytokine array panel, and cell proliferation in vivo. Multiple injections of autologous ASCs accelerated the wound healing process more efficiently compared with that observed in the control treatment. A rat cytokine array test showed that transplanting ASCs led to significantly elevated expression of VEGF. Therefore, angiogenesis was significantly improved in ASC-treated rats, as more microvessels were observed in the wound skin of the experimental rats than in that of the control rats. Transplanted ASCs not only survived in the wound bed but also participated in the blood vessel regeneration process. ASCs also accelerated the wound healing process by increasing the rate of cell proliferation in the wound skin. Our data suggest that autologous ASCs transplantation accelerated the burn wound healing process and promoted blood vessel regeneration. ASCs could potentially be used in burn wound healing treatment.
Introduction
As the largest organ of the body, skin performs several functions, including secretion of sweat, excretion of wastes, maintenance of body temperature, and prevention of pathogen invasion [1]. The main structure of the skin is composed of epidermis, dermis, and subcutaneous tissue. Deep skin injuries caused by fire, hot water, or steam are very commonly observed in the clinic. These patients are vulnerable to infection and metabolic imbalances, which sometimes lead to amputation or even death [2]. Therefore, it is very important to find an effective solution to close such wounds as quickly as possible.
The wound healing process includes four phases: hemostasis, inflammation, proliferation, maturation, and remodeling [3]. The proliferation phase is crucial for wound healing. It is composed of epithelialization, angiogenesis, and granulation tissue formation. This phase is characterized by further extracellular matrix (ECM) deposition, wound contraction, and scar formation. In deep burn wound patients, epithelialization is initiated by keratinocytes presenting on the wound edge. Stimulation by EGF, TGF-β, PDGF, FGF, and VEGF rapidly promotes the recruitment and proliferation of keratinocytes and fibroblasts. The fibroblasts release collagen and fibronectin, and replace the initial fibrin matrix with the new ECM. The fibroblasts are also thought to contribute to angiogenesis during wound healing by decreasing matrix metalloproteinase activity [4]. Re-epithelialization then occurs as the epithelial cells at the wound edge proliferate and migrate to the center of the wound. Re-epithelialization can also be initiated by the proliferation of stem cells from dermal appendages, such as hair follicles, sweat glands, and sebaceous glands [4]. However, this healing process is much more difficult in deep burn wound due to the damage of dermal appendages. Wound healing is a highly active metabolic process that requires increasing amounts of nutrients and oxygen [5]. Therefore, new blood vessel regeneration and augmented angiogenesis are of crucial importance for wound healing, since they enable the transport of nutrients, immune cells, and oxygen.
Burn wound care is increasingly common in clinical practices, with available treatments, including skin grafting, skin substitutes and wound dressings. Delayed healing, infection, pain, and scarring continue to confound burn treatment [6]. Slow wound healing may result in pain and infection, and places a large financial burden on the health care system. However, while contraction is necessary for wound closure, excessive contraction can eventually lead to the formation of a hypertrophic scar. The incidence of such scars has been reported to range from 32% to 94% [7,8]. Hypertrophic scars can be associated with significant pain and limited movement when present over joints.
Innovations in stem cell studies provide additional therapeutic options for treating burn wounds. Many studies have shown the efficacy of stem cells in promoting burn wound healing [9]. Mesenchymal stem cells (MSCs) are multipotent cells capable of self-renewal and can differentiate into tissue-specific cell types. Many types of stem cells have been used in clinical trials for wound healing, but none have been approved yet [10]. It is well known that stem cell-based therapy for skin regeneration requires a sufficient number of cells, which means that they must have the ability to be easily expanded in vitro. Among various sources of stem cells, embryonic stem cells and induced pluripotent stem cells are limited in clinical situations because of safety concerns and ethical considerations [11]. Bone marrow-derived MSC isolation involves an invasive and painful procedure. Adipose-derived stem cells (ASCs) are abundant and can be easily obtained from subcutaneous adipose tissue isolated through liposuction in the clinic. Therefore, ASCs have been considered an attractive cell source for cell transplantation therapy in regenerative medicine.
In numerous studies, ASCs have been shown to secrete the factors TGF-β1, TNF-α, PGE2, GM-CSF, VEGF, bFGF, HGF, IGF-1 and HIF-1α, and interleukins 6, 7, 8, and 11 [12]. According to many studies, ASCs can promote the secretion of angiogenic and antiapoptotic factors to cure ischemic limb disease or increase skin graft survival [12]. However, Franck, C. L. treated burn wound rats with allogeneic ASCs [13], and demonstrated that no difference was found between the groups in relation to the number of blood vessels.
Therefore, more research into the role of ASCs in burn wound treatment is required. Although some researchers have investigated the role of stem cells in wound healing, they have focused on young animal models [14] and allogeneic transplantation [15]. This study used 1-year-old rats and autologous transplantation to explore the efficacy of ASCs in burn wound healing.
Materials and Methods
Animals and burn wound model
Adult male Sprague-Dawley rats were purchased from SLAC Laboratory Animal Co. Ltd. (Shanghai, China) and were used to create a rat model of burn wounds. All rats were maintained on a 12-h light cycle in the animal facility of the Animal Unit of Tongji University. When the rats were 1-year old, they were anesthetized by intraperitoneal injections of pentobarbital sodium (2%, 50 mg/kg). Then, a 2-cm2 burn wound was created on the dorsal skin of each rat using a temperature-controlled desktop scalding instrument (YLS-5Q, Jinan, China). The third-degree burn wound was created on the back of rat by putting the head of the iron (100°C) onto the skin for 10 s. The pressure of the iron head was 1000 g. All animal procedures were reviewed and approved by the institutional animal care and use committee (IACUC) of Tongji University. The approval number is TJLAC-016-027.
Isolation and culture of autologous adipose-derived stem cells
One month before generating the burn model, autologous ASCs were isolated from the inguinal fat pad (∼1.5 cm3) of each male adult Sprague-Dawley rat according to the method of Zografou [16]. In brief, the fat pad was washed with sterilized phosphate-buffered saline (PBS) three times, minced with sterile scissors, and digested with 0.1% type 1 collagenase (17100-017; Gibco) at 37°C for 1.5 h, during which time the tube was shaken every few minutes. The cell suspension was centrifuged at 300 g for 3 min. Then, the supernatant was discarded, and the pelleted stromal vascular fraction (SVF) containing ASCs was resuspended in complete medium and filtered through a 70-μm mesh filter. The cell suspension was centrifuged again, and the cell pellet was resuspended in Dulbecco's modified Eagle's medium/F12 (DMEM/F12) media (Gibco) supplemented with 10% fetal bovine serum (Gibco). These cells were transferred to a 10-cm culture dish and cultured at 37°C in a humidified incubator supplemented with 5% CO2. The medium was carefully changed after 24 h. The culture medium was changed every 3 days after that, until the cells reached a confluence of 80% to 90%. The cells were enzymatically dissociated with 0.05% trypsin-EDTA for subculture.
Transfection and transplantation of ASCs
In brief, transient cotransfection of HEK293T cells was employed to produce lentiviral vectors; the plasmids used were VSVG, delta89, and CD513B (puromycin resistance and expressing GFP). The lentivirus-containing supernatants were harvested 48 h after transfection, then they were centrifuged, filtered, and added to the ASCs (passage 1), which were at 70% confluence. Three days after transfection, the infection efficacy was detected using a fluorescence microscope.
In this study, a third-degree burn wound model was successfully established in 27 rats, which were divided into 3 groups. Each rat was subcutaneously injected with 500 μL fresh GFP-labeled ASCs or PBS into the wound bed using a 1-mL syringe. The injection site includes the wound center and the area 0.2 cm from the wound edge. A digital camera (EOS M2, Canon, China) was used to obtain images of the wounds. The timeline of the experiment is shown in Fig. 1A. The rats described in Figs. 1B and 4 were not included in this group of 27 rats.
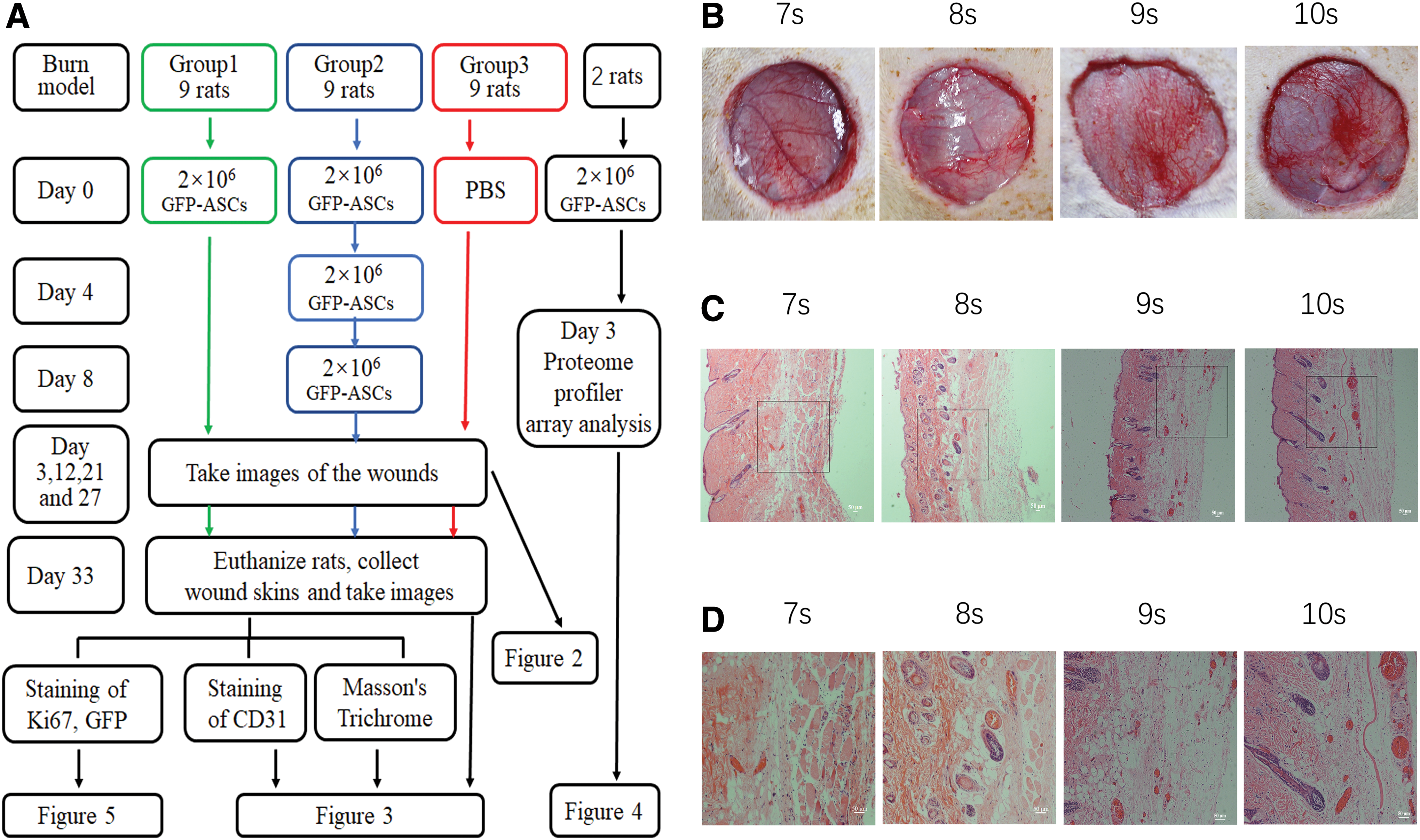
The timeline of the experiment and the determination of optimal burn time.
For group 1, the model of a third-degree burn wound was successfully established in nine rats. After a 2-cm2 burn wound was made on the dorsal skin, 2 × 106 GFP-labeled ASCs (resuspended in 500 μL PBS, passage 3) were injected subcutaneously into the wound bed on day 0 (4 h after wound modeling).
For group 2, the model of a third-degree burn wound was successfully established in nine rats. Three doses of 2 × 106 GFP-labeled ASCs (resuspended in 500 μL PBS, passage 3) were injected subcutaneously into the wound bed on day 0 (4 h after wound modeling), days 4 and 8.
For group 3, the model of a third-degree burn wound was successfully established in nine rats. As the control group, each rat was subcutaneously injected with 500 μL PBS.
Blood vessel number assessment
The rats were euthanized on day 33. The regenerated skin from each rat was carefully cut off and divided into two parts. Half of the wound skins were fixed in 4% phosphate-buffered paraformaldehyde for 24 h. Then, they were embedded in paraffin, and 4 μm sections were produced. Masson's trichrome staining was performed in accordance with the protocols of the manufacturer (Biosciences Inc.). The collagen fibers were stained blue, and the nuclei were stained black. The other structures were stained red. For a small blood vessel definition, we used the following criteria: (1) tubular structure with thick intima, (2) tubular structure with thin intima but containing many erythrocytes inside of it, or (3) >15 μm. The number of small blood vessels was quantified from randomly photographed images (magnification: 100). Forty-five fields were evaluated for each group (five fields per rat). The means ± standard deviation (SD) and statistical significance were assessed by GraphPad Prism.
The number of microvessels in the wound skin was determined by immunohistochemical staining using anti-CD31 antibodies. In brief, after fixing, embedding in paraffin, and dewaxing, antigen retrieval was performed and was followed by 3% H2O2 blocking. Then, the tissue sections were blocked with 5% normal goat serum for 30 min. The sections were then incubated with a primary antibody against CD31 (1:300 dilution, sc-53526; Santa Cruz) for 15 h at 4°C, followed by incubation with goat anti-mouse IgG (secondary) for 1 h at room temperature. After washing with PBS, diaminobenzidine was used to produce a brown precipitate. After hematoxylin staining, tissue sections were washed and then dehydrated with ethanol, treated with dimethylbenzene, and sealed for microscopic analysis. For microvessel counting, CD31-positive vessels were quantified from randomly photographed images (magnification: 200). Forty-five fields from each group were evaluated (five fields per rat). The mean ± standard deviation (SD) and statistical significance were assessed by GraphPad Prism.
ASC tracing and proliferation assessment by immunohistochemistry (frozen tissue)
The other part of the wound skins not used for blood vessel assessment was immersed in O.C.T. compound and quickly frozen by placing in liquid nitrogen for 10 s. These samples were stored at −80°C until cryosectioning. The 10-μm sections were cut, washed with PBS, and incubated with primary antibodies against GFP (1:500 dilution, ab1218; Abcam) and Ki67 (1:500 dilution, PA5-19462; Invitrogen), followed by incubation with a secondary antibody (1:1,000 dilution) for 1 h at room temperature. The secondary antibodies used were as follows: donkey antirabbit IgG H&L, Alexa Fluor 488 (A-21206; Invitrogen), and donkey antirabbit IgG (H+L), Alexa Fluor 568 (A10042; Invitrogen).
Proteome profiler array analysis
Two rats were prepared for proteome profiler array analysis. After anesthetization by intraperitoneal injections of pentobarbital sodium (2%, 50 mg/kg), two burn wounds (2 cm2) were made on the dorsal skin of each rat. Four hours later, 500 μL PBS was injected subcutaneously into the left wound, and 2 × 106 GFP-labeled ASCs (resuspended in 500 μL PBS, passage 3) were injected subcutaneously into the right wound.
The wound skin from each rat was excised on day 3 after generating the wound model. Each skin was washed with sterile PBS and mixed with a protease inhibitor cocktail (Promega, Madison, WI). Each skin was cut into pieces and homogenized to test for cytokine factors by a proteome profiler array according to the manufacturer's protocol (Rat Cytokine Array Panel A, ARY008; R&D Systems). Total proteins were extracted, centrifuged, and resuspended in sample application buffer containing a protease inhibitor cocktail (Promega). The kit instructions were strictly followed to perform the proteome profiler array analysis. The relative levels of cytokines were quantified using ImageJ.
Statistical analysis
A two-way ANOVA with Tukey's multiple comparisons test was performed for multiple group comparison using the program GraphPad Prism, and the results are shown in Fig. 2. Statistical analysis for Fig. 3 was performed by multiple t tests. Data are presented as the mean ± standard deviation (SD), and differences were considered significant when P < 0.05. * denotes P < 0.05, ** denotes P < 0.01, and *** denotes P < 0.001.
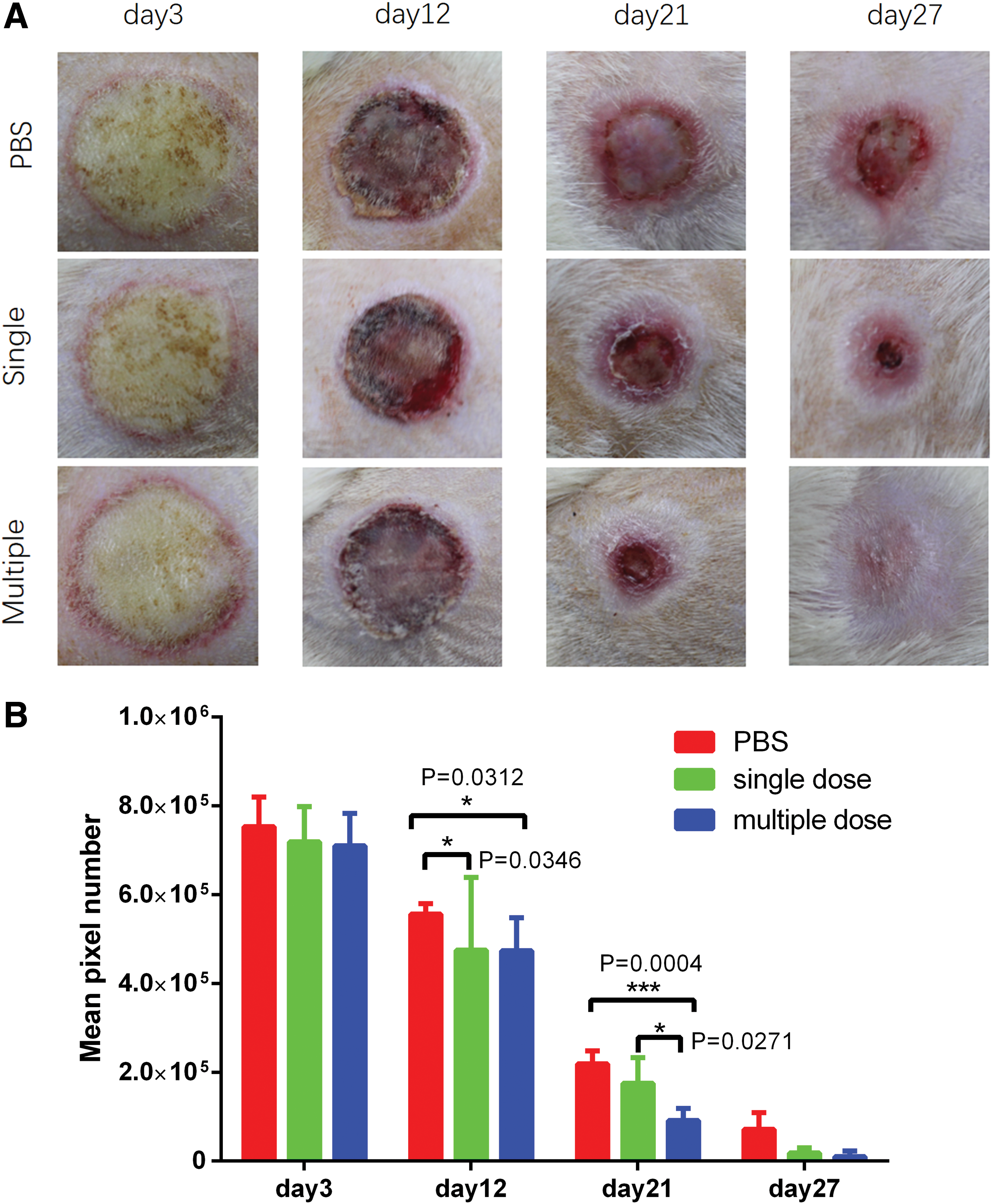
Multiple injections of autologous ASCs efficiently accelerated the wound healing process. The rats in the single dose group were injected with autologous ASCs (2 × 106 cells/rat) into the wound bed subcutaneously on day 0. The control group received the same volume of PBS (500 μL). The rats in the multiple dose group were injected with autologous ASCs (2 × 106 cells/rat) into the wound bed subcutaneously on days 0, 4, and 8. The wound size of each rat was reduced in the treated groups compared with the PBS group. Differences between experimental groups were assessed by Student's t test.
ASCs improve angiogenesis by regeneration of blood vessels.
Results
Creation of third-degree burn wound model
A special machine was employed to create a rat model of third-degree burn wounds. A series of scald times were tested to determine the optimal modeling procedure. The full-thickness skins were removed carefully to observe the integrity of the subcutaneous tissue. As shown in Fig. 1B, the blood vessels were injured when scalded for 10 s. The burn wound degree was confirmed by HE staining; typical images are shown in Fig. 1C and D. The dermal layer of the skin was completely destroyed, and the blood vessels were injured when scalded for 10 s. The H&E staining results confirmed that the dermal layer of the skin was completely destroyed. The third-degree burn wound was successfully generated with 10 s of scalding. Therefore, we generated burn wound models using 10 s of scalding in this study.
Autologous ASCs accelerate the burn wound healing process in a rat model
In group 1, the results showed that a single injection of 2 × 106 autologous ASCs could improve the wound healing efficacy to a certain degree in comparison with that in the PBS group. Representative images for the two groups on days 3, 12, 21, and 27 post-treatment are presented in Fig. 2A.
In group 2, the result showed that multiple injections of 2 × 106 autologous ASCs improved the wound healing process more efficiently than that observed in the control group. Representative images of the three groups on days 3, 12, 21, and 21 post-treatment are presented in Fig. 2A. The wound size of the treated group on day 21 was significantly smaller than the wound size in the PBS group. The mean wound size was quantified by calculating the mean pixel number of the wound areas. Quantification analysis of the mean wound size at different time points (Fig. 2B) showed that the period from days 12 to 21 is critical for wound repair.
In conclusion, the efficacy of ASC promotion of wound healing was associated with injection times, and multiple injections of ASCs accelerated the wound healing process more efficiently than single injections.
ASCs improve angiogenesis by elevating local VEGF levels
It has been reported that MSCs play a therapeutic role by providing immunomodulation and paracrine effects. Therefore, we decided to test whether ASCs promote burn wound healing in this manner. We used a rat cytokine antibody proteome profiler array system to assess the inflammation-related cytokines and chemokines. To eliminate individual differences, the control skin and ASC-treated skin were dissected from each rat on day 3 after the injection of ASCs. We chose day 3 as our time point of testing cytokines based on the published article. At this time point, changes induced by ASCs are strong enough to be detected. Two rats were prepared for this experiment. The results showed that multiple cytokines, such as CINC-1, CINC-2α/β, CINC-3, slCAM-1, IL-1α, IL-1ra, LIX, L-Selectin, CCL3, CXCL7, TIMP-1, and VEGF, were changed (Fig. 4). Comparing the results of these two rats, we found that VEGF levels were significantly upregulated in the wound skin of both rats. VEGF has been widely recognized as the most effective and specific growth factor that can promote vascular regeneration. A high level of VEGF indicates that angiogenesis may play an important role in wound healing.
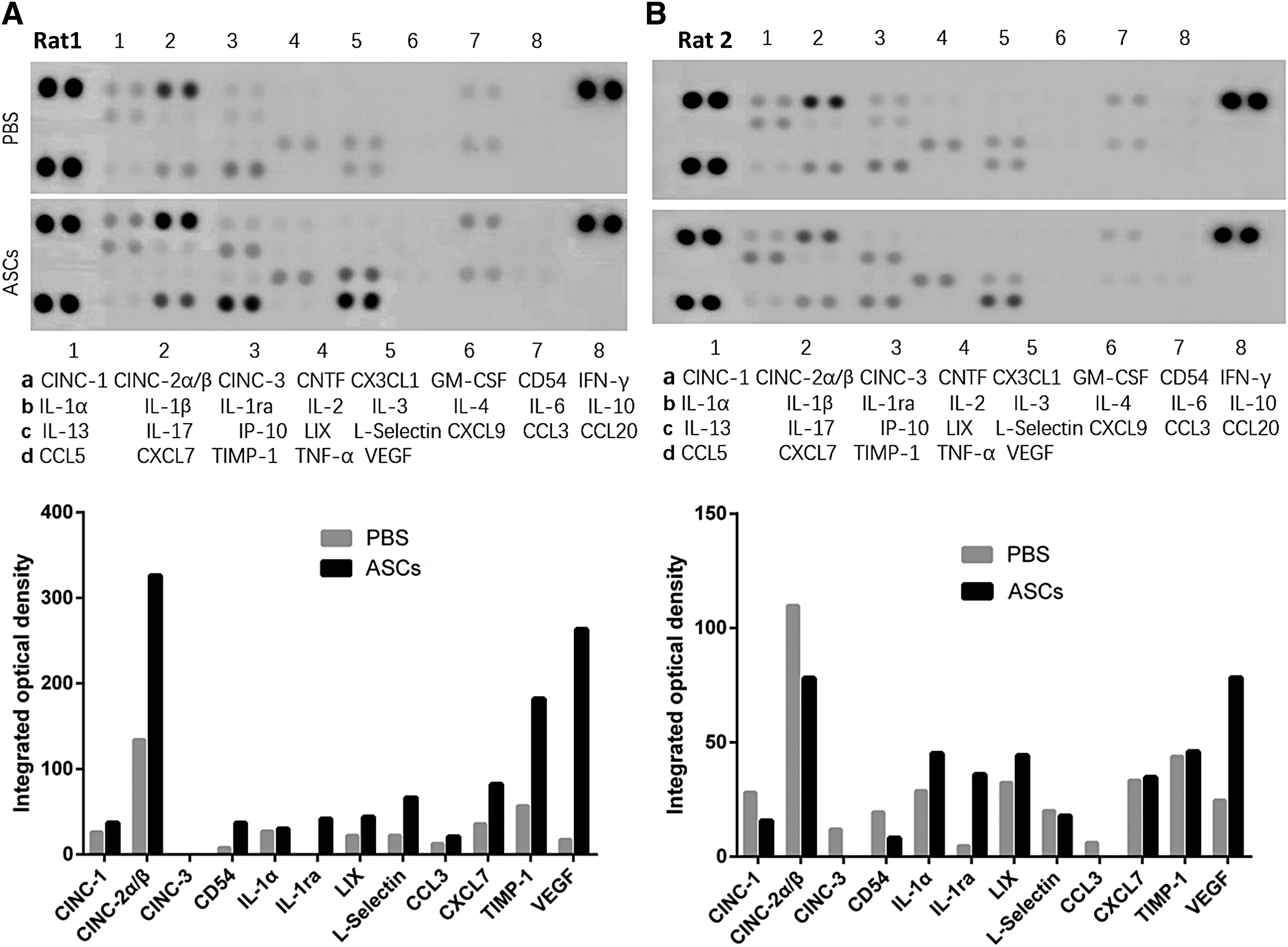
Rat cytokine array analysis confirmed that ASCs elevated VEGF levels in the wound skin bed and consequently promoted blood vessel formation. The R&D Systems Rat Cytokine Antibody Proteome Profiler Array System was used to screen for inflammation-related cytokines and chemokines in wound skin tissues on day 3 after ASC treatment. Four spots on the left and two spots on the right are used as references. The pair of duplicate spots represents each cytokine. Quantification of positive cytokines and chemokines was illustrated by integrated optical density. VEGF levels were significantly upregulated in the ASC-treated wound skin of both rats. Other cytokines, such as CINC-2α/β and TIMP-1, changed significantly, but the trend for the change was inconsistent. The reason for this may be due to individual differences.
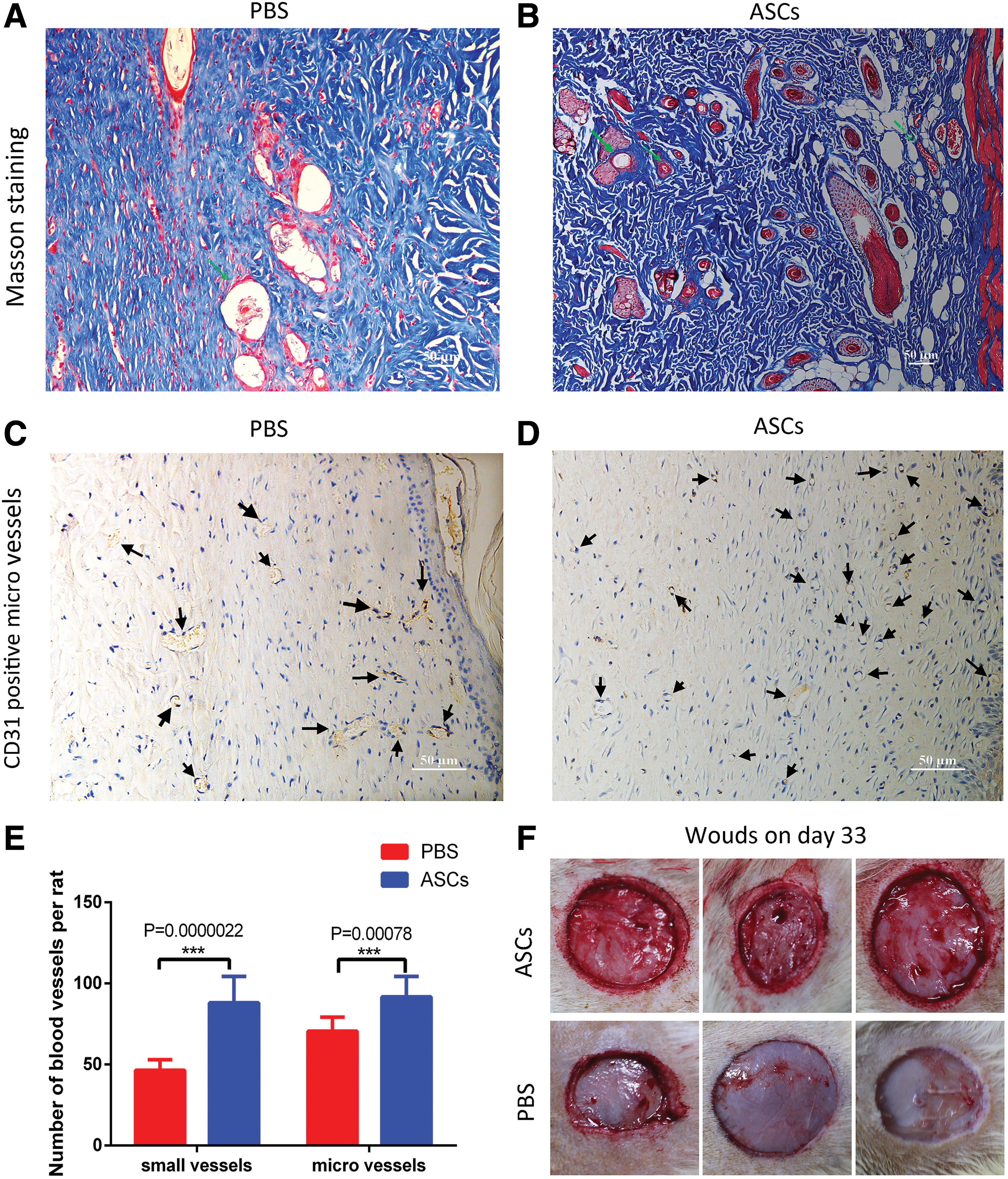
ASCs improve angiogenesis by the regeneration of blood vessels
Because a high level of VEGF was found in the wound skin of ASC-treated rats, the vascularity of wound tissue was evaluated. Specifically, we evaluated the subcutaneous vascularity (Fig. 3F). On day 33, when all the wounds were completely repaired, we carefully excised the skin and captured images using a digital camera. The vascularity status of the ASC-treated group was significantly better than that of the PBS group, indicating that transplanted ASCs could increase the number of blood vessels and consequently accelerate the wound healing process. Masson's trichrome staining was performed to confirm the number of small blood vessels in wound skin. As shown in Fig. 3A and B, we found many more small blood vessels in the wound skin of ASC-treated rats. Furthermore, immunohistochemistry staining of CD31 showed more microvessels in the ASC-treated rats than in the PBS-treated rats (Fig. 3C, D). The mean number of blood vessels in each group was statistically analyzed according to the method described above (Fig. 3E). Taken together, transplantation of autologous ASCs significantly promoted blood vessel regeneration.
ASCs participate in the process of blood vessel and dermis regeneration
To determine the role of ASCs in the wound healing process, GFP-labeled autologous ASCs were traced by immunofluorescent staining. As shown in Fig. 5, GFP-labeled ASCs participated in the process of blood vessel and dermal regeneration. This result showed that autologous ASCs could differentiate into vascular endothelial cells in vivo. However, the major ASCs were fibroblast-like cells, which did not differentiate into skin appendages. Furthermore, most of the ASCs were found in the inner part of the wound skin, demonstrating that ASCs failed to regenerate the epithelial layer effectively.
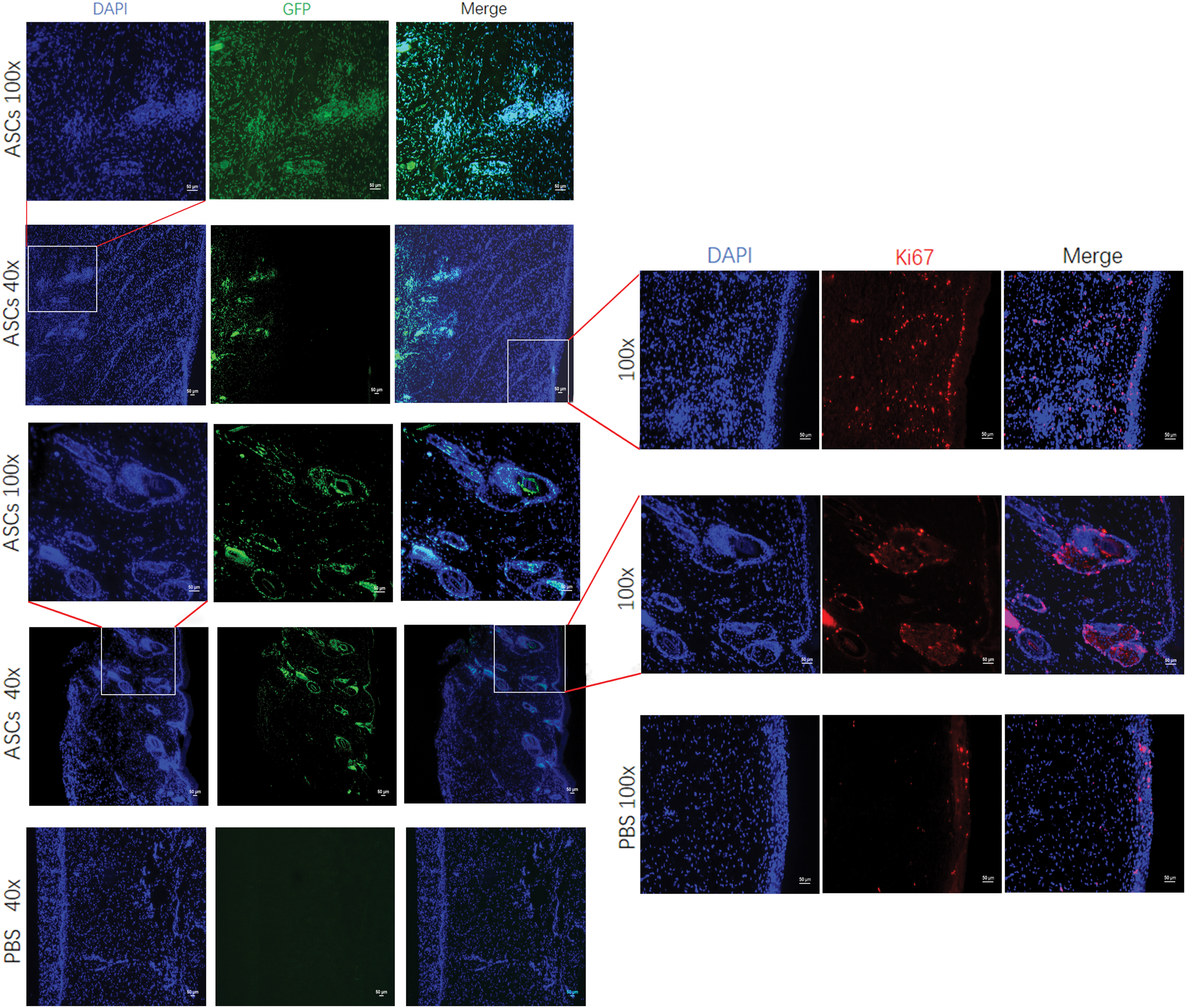
ASC tracing and proliferation testing further demonstrated that ASCs may contribute to the wound healing process by participating in blood vessel formation and improving cell proliferation. GFP-labeled ASCs participated in the process of blood vessel and dermal regeneration. The results showed that autologous ASCs could differentiate into vascular endothelial cells in vivo. Furthermore, the number of Ki67-positive cells was significantly higher in the ASC-treated group than in the PBS-treated group. In addition, more Ki67-positive cells were found in the dermis of the ASC-treated group than in the PBS-treated group, suggesting that ASCs may improve the proliferation of dermal cells to consequently accelerate the wound healing process. Color images are available online.
However, ASCs must have many other mechanisms to promote wound healing. We only tested the expression of Ki67, which is a proliferation marker. Increasing amounts of Ki67 expression indicated that more cells will be generated, which will accelerate the wound healing process. In our study, the number of Ki67-positive cells was significantly higher in the ASC-treated group than in the PBS group. In addition, more Ki67-positive cells were found in the dermis, suggesting that ASCs may improve the proliferation of dermal cells and accelerate the wound healing process.
Discussion
ASCs can be easily acquired in great quantities that require only minimally invasive procedures [17]. The proportion of cells that are MSCs is 500 times higher in adipose tissue than that found in the bone marrow [18]. Therefore, a large number of cells can be obtained without many cell passages, lowering the chance of chromosomal abnormality-induced senescence. Therefore, we chose ASCs as the basis for this study.
Allogeneic stem cells are convenient and can be prepared in advance of treatment. However, the short survival time of allogeneic stem cells makes them unable to treat long-lasting wounds. This cannot be overcome by multiple injections because of strong immune rejection induced by immune memory [19]. It has been reported that injected allogeneic cells in lung vessels have a half-life of ∼24 h. New technologies for prolonging stem cell survival are still in development [20]. In contrast, the use of autologous ASCs has been reported in articles on many topics, such as liver transplantation [21], skin grafts [16], swine hypertrophic burn scars [22], and spinal cord injury [23]. The only use of autologous ASCs in burn wound healing was published in 2018 [24]. Therefore, our study provides insight into the mechanisms of ASCs and their long-term fate in wound healing.
The freezing and thawing rates of cryopreservation can affect the physicochemical and biophysical reactions of a cell, altering the survival rate and proliferation ability [25]. Furthermore, cryopreserved MSCs have lower immunomodulatory and blood regulation effects directly after thawing, resulting in faster complement-mediated elimination after blood exposure [26,27]. A better understanding of the chemistry and biology behind freezing and thawing will be necessary for finding the safest and most effective cryopreservation method to use in the future [25]. Therefore, we used fresh ASCs to treat skin wounds.
In our study, a single injection of ASCs was not enough to restore the burn wound skin. Multiple injections of ASCs accelerated the burn wound healing process significantly. Very few studies have focused on multiple injections of MSCs [28], and even fewer studies have focused on ASCs. The mechanism responsible for the improved efficacy of multiple injections is still unclear. One possible hypothesis is that most ASCs lose their high proliferative capacity in the wound microenvironment. Therefore, multiple injections of ASCs are needed during the wound healing process. Our findings may provide new insight into the field of clinical application of stem cell therapy.
The wound cannot be completely healed in the absence of re-epithelialization [29]. To accelerate re-epithelialization, keratinocyte transplantation was advanced [30]. The restoration of the dermis is important for skin wound healing. The dermis provides space for regeneration of microvessels and for facilitating adherence of the new or transplanted epidermis [31]. A major disadvantage of this technique is the long time (3 weeks) interval between biopsy and grafting [32]. Furthermore, limitations such as a high risk of recurrent open wounds, contamination, long-term fragility, and increased rate of scar contraction have been reported [33 –35]. However, in our study, ASCs did not differentiate into keratinocytes, but they were still able to accelerate re-epithelialization. This may be due to their strong effect on angiogenesis and dermis regeneration. The relationship between ASCs and epithelial cells or keratinocytes may be of great importance for the treatment of wound healing in the future.
The immunosuppressive properties of MSCs have attracted much attention from immunologists, stem cell biologists, and clinicians. Several factors and molecules secreted by MSCs have been linked to the immunoregulatory function of these cells. These molecules include IL-1ra and IL-10 [36]. In our study, we found that the expression of many inflammatory factors was very low, such as IL-1α, IL-1β, IFN-γ, IL-2, IL-3, IL-4, and IL-6. IL-1α was slightly upregulated in ASC-treated rats, but the anti-inflammatory factor IL-1ra was obviously upregulated compared with that in control rats. This finding confirmed the immunosuppression property of ASCs in our study. The expression levels of CINC-2α/β and TIMP-1 fluctuated greatly between the 2 rat groups. This may be due to individual differences. However, VEGF was significantly upregulated in both rat groups, which was consistent with our other findings. It is noteworthy that the low expression of inflammatory factors observed in our study indicated that the immunosuppression properties of ASCs may not be very active during the wound healing process.
ASCs transplanted into compromised tissue might have therapeutic properties, rejuvenating the damaged tissues [37]. However, the biological and functional characteristics of ASCs may be positively correlated with age [38]. In our study, 1-year-old rats were used in the burn wound model. The regenerating ability of the rats declined with age, mimicking the true status of adult and elderly burn wound patients. Consequently, the wound healing time of rats in our study was longer than that of young rat models in another study [14]. We believe that the quantity of autologous ASCs derived from old rats is still able to meet the need for stem cell therapy.
In conclusion, this study demonstrates that multiple injections of ASCs accelerated the wound healing process more efficiently than the untreated control. Both small blood vessels and microvessels were significantly regenerated in ASC-treated rats. We also found significantly elevated expression of VEGF in the ASC-treated rats. Furthermore, autologous ASCs directly participated in the regeneration process of blood vessels. These results suggested that ASCs accelerated the burn wound healing process at least partially by promoting angiogenesis and accelerating re-epithelialization. However, more evidence is required to solidly prove this conclusion. Furthermore, ASC treatment promoted the wound healing process by promoting cellular proliferation. More Ki67-positive cells were found in the ASC-treated group than in the PBS-treated group. This finding indicated that ASCs may promote proliferation by secreting specific factors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by The National Major Scientific and Technological Special Project for “Significant New Drugs Development” (2018ZX09201002-005); the National Natural Science Foundation of China (31471029, 31671055, 81461138037); and Xu Jun's expert work station (2017IC025).