
Abstract
Pressure injuries/ulcers are frequent complications in elderly, paraplegic, and quadriplegic patients, which account for considerable cost to the international health care economy and remain refractory to current treatment options. Autologous or allogeneic adult stromal/stem cells represent an alternative therapeutic approach. The current study extends prior findings by exploring the safety and efficacy of human adipose-derived stromal/stem cell (ASC) therapy in an established immunocompetent murine skin pressure ulcer model where dermal fibroblast cells (DFCs) served as a control. Human adipose tissue was processed using a closed system device designed for point-of-care use in the operating room and on file with the Food and Drug Administration. Cell characterization was performed using colony-forming unit–fibroblast, differentiation, and immunophenotypic assays in vitro. Wound healing was assessed over a 20-day period based on photomicrographs, histology, and immunohistochemistry. The isolated human ASCs displayed significantly greater colony formation relative to DFCs while both populations exhibited comparable immunophenotype and differentiation potential. Both fresh and cryopreserved human ASCs significantly accelerated and enhanced wound healing in young (2 month) mice of both sexes relative to DFC controls based on tissue architecture and CD68+ cell infiltration. In contrast, while injection of either fresh or cryopreserved human ASCs was safe in older mice, the fresh ASCs significantly enhanced wound closure relative to the cryopreserved ASCs. Overall, these findings support the safety and efficacy of human ASCs isolated using a closed system device designed for clinical procedures in the future treatment of pressure injuries.
Introduction
Pressure injuries or ulcers are a major medical and surgical challenge that burdens health care economies throughout the globe. While the etiology underlying pressure ulcer (PU) development is an area of active investigation, a growing body of evidence has linked the injury to ischemia/reperfusion, the formation of reactive oxygen species, and the onset of a proinflammatory cytokine cascade impacting the extracellular matrix (ECM) [1 –4]. PUs are categorized to range from least severe (Stage 1), involving the superficial epidermis of the skin, to most severe (Stage 4), involving the epidermis, dermis, adipose, muscle, and bone layers. Elderly patients in nursing home environments and paraplegic/quadriplegic patients with spinal cord injuries are at especially high risk for PU development [5 –7]. In developed nations, the cost of PU care can account for up to 4% of all annual medical expenditures [8]. Recent analyses in the United States determined that hospital-acquired pressure injuries occurred in 8.3% of acutely ill-hospitalized patients and accounted for a total cost of $26.8 billion in 2016 dollars. Of this amount, 59% of the costs were attributed to the care of Stage 3/4 patients, representing only 13.2% of the afflicted population [9]. At present, the therapeutic approach to PUs relies heavily on preventive measures, such as frequent turning of patients and the use of beds and chairs designed to reduce friction on vulnerable anatomical sites (elbows, heels, ischium, sacrum). Once initiated, PUs require surgical debridement, negative pressure wound vacuum, skin flaps to achieve repair, and nutritional supplementation to accelerate wound repair [10,11].
Over a decade ago, Stadler et al. developed a simple murine ischemia/reperfusion model of pressure injury by compressing the dorsal skin with externally placed magnets and then releasing for repetitive 12 h cycles over 3 days [12]. Since publication, this elegantly simple in vivo model has been used to evaluate healing of pressure injuries created in young, aged, obese, immunodeficient, and genetically modified mice [2,3,13 –17]. An early study transplanting human mesenchymal stem cells (MSC) intradermally into an immunodeficient non obese diabetic severe combined immunodeficiency (NOD-SCID) PU model failed to observe any acceleration in wound healing [16]. In contrast, numerous subsequent independent studies have reported enhanced regeneration following cell therapy. Injection of primary MSC, fibrocytes derived from human embryonic stem cell MSC, myeloid-derived suppressor cells capable of undergoing fibrocyte differentiation, or adipose-derived stromal/stem cells (ASCs) have all led to improved rates of wound repair [3,13,18 –23], and this body of literature has recently been reviewed [24]. These studies have implicated a number of mechanisms of action including the modulation of TGFβ signal transduction pathways, oxidative damage, and the expression of ECM proteins. Additionally, stromal/stem cells from adipose tissue and bone are known to secrete cytokine/growth factors and micro-RNA containing exosome/microvesicles, which together constitute the “secretome” [25 –29]. Recent evidence suggests that stromal/stem release of these elements locally and systemically underlies a paracrine-based mechanism of wound regeneration and repair [25,28,30]. Consistent with this mechanism, prior studies have documented enhanced regeneration of murine pressure injuries when injected with murine-derived ASCs [3,13]. The current study extends these observations by evaluating the safety and efficacy of human-derived ASCs when injected into the pressure injury model created in immunocompetent mice.
Materials and Methods
Institutional support approval
The human study protocols were reviewed and approved by the Western Institutional Review Board (Puyallup, WA) (Study no. 1138160). The animal study protocol entitled “Adipose-Derived Stromal/Stem Cell Therapy for Pressure Ulcers” (Protocol no. 4313R) was reviewed for renewal and approved on June 21, 2019, by the Tulane University Institutional Animal Care and Use Committee (IACUC) (Assurance no. A4499-01).
Animal purchase and housing
Male and female C57BL/6 mice (8 week and 22 month old; Charles River Laboratory, Wilmington, MA and NIA Aging Colony) were quarantined (1 week) and housed in the Tulane University Department of Comparative Medicine Vivarium (Gina Dobek DVM) with ad libitum access to water and chow under a 12-h light:12-h dark schedule. In keeping with recent NIH guidelines, study cohorts included equal numbers of both male and female mice [31].
Human adipose tissue donation
Tissue donors were recruited anonymously from consenting patients undergoing elective cosmetic plastic surgery with inclusion criteria: patients aged ≥18 years, male or female, undergoing elective cosmetic, or reconstructive procedures and exclusion criteria: patients with viral infectious diseases, cancer (other than basal cell carcinoma of the skin), or pregnancy.
Human adipose tissue Icellator processing
Lipoaspirates from human adipose tissue were transferred to LaCell's laboratory within 24 h following harvest at ambient temperature while suspended in an isotonic buffered solution in a closed container. Sixty milliliters volumes of tissue was processed in the Tissue Genesis Icellator® (Tissue Genesis, Houston, TX) closed system instrument using the Adipase® enzyme to yield stromal vascular fraction (SVF) cells in accordance with the manufacturer's instructions. The resulting SVF cells were culture expanded to generate ASCs according to published methods [32].
ASC characterization and cryopreservation
ASCs were characterized by differentiation potential, cell surface markers, and colony-forming unit–fibroblast (CFU-F) assays as published [33]. ASCs were cultured to 80%–90% confluence in StromaQual™ (LaCell LLC) and induced with either AdipoQual™ or OsteoQual™ medium for adipogenesis and osteogenesis, respectively. Mature cultures were fixed and stained with Oil Red O (adipogenesis) or with Alizarin Red (osteogenesis) and photomicrographs obtained using Motic Image 3.0 software. Freshly cultured ASCs (Passage 1; P1) were expanded to 80%–90% confluence from Icellator-prepared SVF cells from three different donors, harvested on injection day with 0.25% trypsin/EDTA solution, resuspended in sterile phosphate buffered saline (PBS), and kept on ice until the time of injection. To obtain cryopreserved cells, ASCs (P0) from three different donors were thawed in a 37°C water bath for 60–90 s, were transferred to stromal medium, centrifuged for 5 min at 300g (1,200 rpm), resuspended in stromal medium, and plated on separate T175 flasks. ACSs were maintained by feeding flasks every 3–4 days with fresh StromaQual to 80%–90% confluence, harvested with 0.25% trypsin/EDTA, pooled, and cryopreserved in a frozen medium containing 2% dimethyl sulfoxide (DMSO) and 6% human serum albumin in Dulbecco's modified Eagle's medium (DMEM) in liquid nitrogen for at least 24 h before injection into PUs.
CFU-F assay
The trypsin-harvested ASCs were seeded in six-well plates at densities per well of 50 or 100 ASCs per well. Wells were fixed at 12–14 days with 4% formaldehyde, stained with Toluidine Blue, and colonies of >50 cells counted as previously described [34].
Flow cytometry
Cell surface markers were analyzed on a FACS Aria (Becton Dickinson, San Jose, CA) instrument by suspension of ∼106 ASCs in PBS, stained for 30–60 min with anti-CD29, anti-CD105, anti-CD45, anti-CD34, anti-CD44, anti-CD73, anti-CD90, and isotype control IgG1, washed with PBS, and flow cytometry performed according to published methods [32,33,35].
Dermal fibroblast cell characterization and cryopreservation
Isolated dermal fibroblast cells (DFCs) from human abdominoplasty skin specimens (LaCell Catalog no. DFC-01) were characterized with respect to differentiation, surface antigens, and CFU-F using the methods as described above for human ASCs.
Histology and immunohistochemistry analysis
Skin sections from wounds were stained with hematoxylin and eosin (H&E) and Masson's trichrome. The H&E sections were scanned with PrimeHisto XE Histology slide scanner (Carolina Biological Supply Company) and analyzed for depth of epidermis, dermis, subcutaneous adipose layer, and muscle layer at three different sections of the wounded skin with measurements performed using the ImageJ (NIH, Bethesda, MD) software as previously published [3]. Photomicrographs from Masson's trichrome-stained sections were photographed with a Motic microscope digital camera and analyzed for collagen expression with Cell Profiler (Cambridge, MA) based on blue staining relative to the total photomicrograph tissue area. Immunohistochemistry was performed according to published methods [36]. Briefly, immunohistochemical procedures were performed on formalin-fixed and paraffin-embedded skin sections. The following primary antibody was used: anti-CD68 (1:400, Abcam). Antibody binding was detected using the ABC complex (Vector Laboratories, Inc.). Peroxidase activity was revealed using 3.3-diaminobenzidine (Sigma–Aldrich) as a substrate. Slides were counterstained with hematoxylin.
Statistics
Statistical analyses were performed using GraphPad Prism 8 (San Diego, CA). Comparisons between groups were performed using two-tailed Student's t-test, one-way analysis of variance (ANOVA), two-way ANOVA, and post hoc Tukey's test where appropriate. Values are reported as the mean ± standard deviation (SD) where statistical significance was determined based on P ≤ 0.05.
Results
Characterization of human ASCs and DFCs
Culture-expanded ASCs were characterized based on differentiation and immunophenotype. Based on CFU-F assays, the ASCs had an average cloning efficiency of 32.44% ± 13.34%, whereas the DFCs had an average cloning efficiency of 16.22% ± 10.78% (n = 3 donors, data not shown). Furthermore, both ASCs and DFCs demonstrated a higher capacity to develop lipid droplets and matrix mineralization as a result of adipogenic and osteogenic induction for 12–14 days compared with the uninduced control cultures (Fig. 1A, B). The mean percent expression by flow cytometry for immunophenotypic surface markers is shown in Fig. 1C and is consistent with previously reported findings [33].
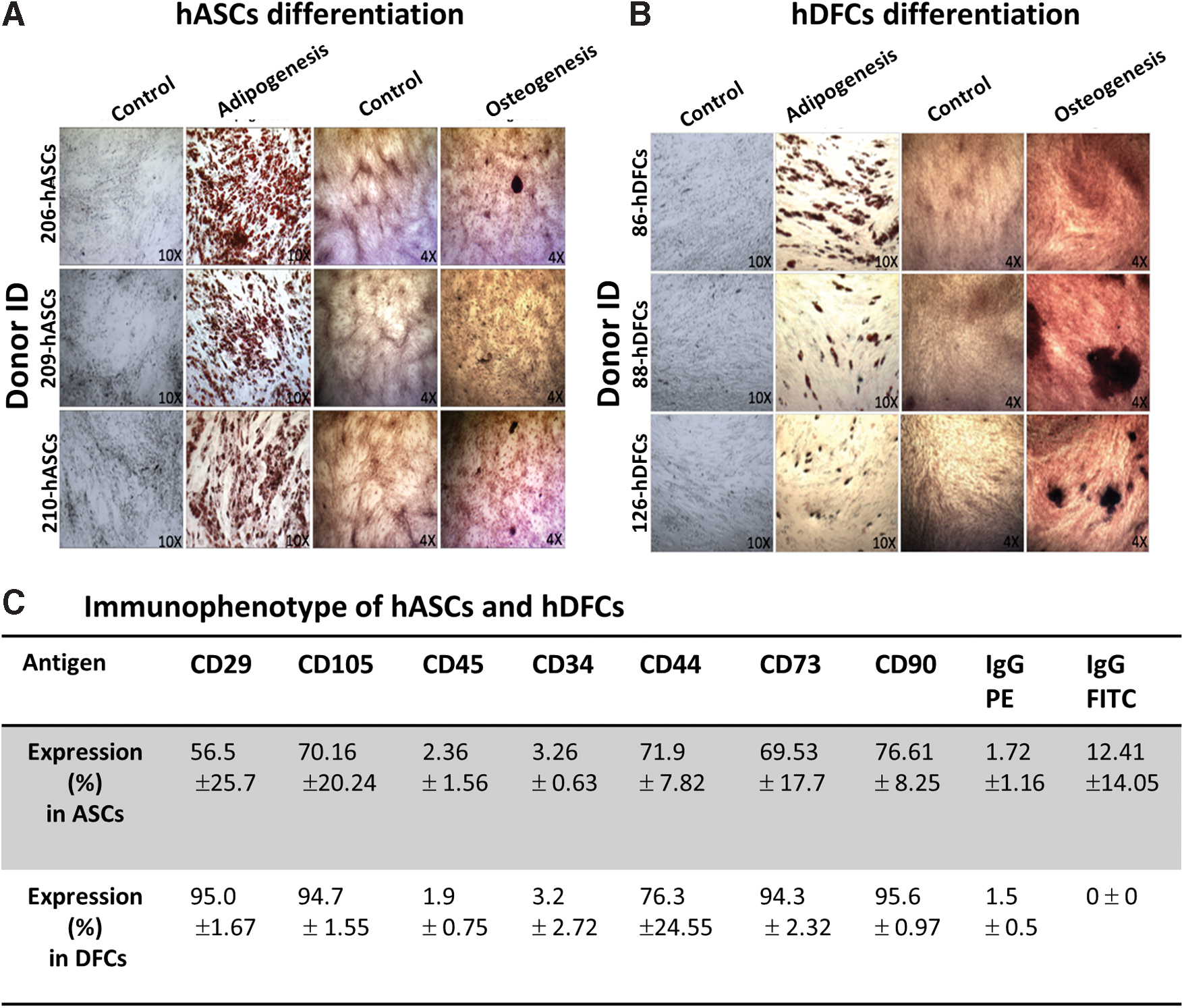
Characterization of culture-expanded human ASCs (passage 1). SVF cells were obtained from human lipoaspirates processed using the Tissue Genesis Icellator instrument and digested using the Adipase® enzyme.
PU healing response to PBS/DMSO controls or DFC therapy in young female and male immunocompetent mice
The percentage of the PU wound remaining open for each day after treatment with PBS/DMSO controls and DFCs was determined relative to the wound size as measured on day 1 (100% openness). Results showed that wounds treated with PBS/DMSO had an accelerated healing rate relative to wounds treated with DFCs. By day 2, wounds treated with PBS/DMSO remained 71.87% ± 18.44% open, whereas wounds treated with DFCs remained 101.31% ± 18.79% open (P < 0.05) (Fig. 2A). This pattern continued at day 4, day 5, day 6, day 8, day 12, day 13, and day 14 (P < 0.05). After day 14, wounds treated with DFCs experienced a steep decrease in the percentage of wound remaining open reaching 0.56% ± 1.01% openness at day 17. In contrast, the percentage of wound remaining open after treatment with PBS/DMSO plateaued from day 15 (14.62% ± 24.36%) until day 20 (13.69% ± 23.90%), indicating that the wounds had not healed completely (0% openness) (Fig. 2A).

Wound healing rates in young and old immunocompetent mice.
PU healing response to fresh ASCs relative to controls in young immunocompetent mice
To investigate the response of PU wounds to different stem/stromal cell treatments relative to controls, young mice (8-week-old both female and male) were treated with fresh ASCs (n = 17) or DMSO/PBS controls (n = 8 for each treatment). Wounds treated with fresh ASCs showed an accelerated wound healing rate relative to the controls at day 8, where the percentage of wound remaining open after treatment with fresh ASCs was significantly lower (38.86% ± 15.24%, P < 0.05) than the percentage of wound remaining open after treatment with controls (47.6% ± 11.02%) (Fig. 2A). The wounds treated with fresh ASCs continued to show a statistically significant accelerated healing relative to the control wounds from day 10 to day 14 (Fig. 2A), reaching an openness of 2.95% ± 5.57% versus 18.43% ± 25.39% at day 14 (Fig. 2A). Finally, treatment with fresh ASCs induced a significantly accelerated healing rate in PU wounds relative to treatment with fresh DFCs. By day 2, wounds treated with fresh ASCs reached an openness of 63.26% ± 20.87% (Fig. 2A). In contrast, by day 2, wounds treated with fresh DFCs increased in size reaching an openness of 101.31% ± 18.79% (Fig. 2A).
PU healing response to cryopreserved ASCs relative to controls in young immunocompetent mice
A similar healing effect was seen in wounds treated with cryopreserved ASCs relative to wounds treated with DMSO/PBS or DFC controls. By day 2, wounds treated with cryopreserved ASCs reached an openness of 64.16% ± 19.08% compared with DFC treatment with an openness of 101.31% ± 18.79% (Fig. 2A). At day 11, the percentage of wound remaining open after treatment with cryopreserved ASCs was significantly lower (17.07% ± 9.12%, P < 0.05) relative to those treated with DMSO/PBS (33.6% ± 20.46%) (Fig. 2A). This pattern was repeated between wounds treated with cryopreserved ASCs versus PBS/DMSO controls at day 13 and day 14, reaching an openness of 2.73% ± 3.41% versus 18.43% ± 25.93% at day 14.
PU healing response to fresh or cryopreserved ASCs relative to controls in older immunocompetent mice
The response of stem/stromal cell treatment in PU wounds was also investigated in older mice (22-month-old both female and male). Older mice were treated with fresh ASCs (n = 9), cryopreserved ASCs (n = 7), and PBS/DMSO control (n = 4) and monitored daily for up to 20 days to determine the percentage of wound remaining open on a daily basis. Wounds treated with fresh ASCs showed a statistically significant faster healing rate relative to treatment with cryopreserved ASCs at day 2, day 5, day 8, and from day 10 to day 13. By day 13, wounds treated with fresh ASCs reached an openness of 26.16% ± 12.78% compared with an openness of 43.62% ± 21.24% reached by wounds treated with cryopreserved ASCs (Fig. 2B). Overall, by the completion of the study period, neither the fresh nor cryopreserved ASCs accelerated wound closure in older mice significantly faster relative to the PBS/DMSO controls.
Histological determination of tissue architecture in young immunocompetent mice exposed to fresh or cryopreserved ASCs relative to controls (PBS/DMSO) or DFCs
Histological analyses of tissue architecture on day 7 and day 20 post-injections were performed on skin samples harvested from young mice (8-week-old). Results of these analyses show that in young mice, wound treatment with PBS/DMSO promoted a more effective wound healing effect during the first 7 days post-injection relative to treatment with DFCs. Histological analyses at day 7 showed that, relative to the DFC treatment group, the PBS/DMSO control group displayed significant hypertrophy of the hypodermis (subcutaneous adipose) layer, consistent with expansion or regeneration of adipose tissue (Fig. 3A). Additionally, at day 7 post-injection, the PBS/DMSO control group showed a significant hypertrophy of the epidermal layer and a significant reduction of the muscle layer relative to the DFC treatment group (Fig. 3A). However, a different pattern was seen in the results of the histological analysis of tissue architecture at day 20 post-injection. At this time point, the DFC treatment group showed an increased depth within all layers, whereas the PBS/DMSO control group showed little change relative to day 7 results (Fig. 3B). Additionally, in the PBS/DMSO control group, the size of the epidermal, dermal, and muscle layer was significantly reduced relative to the corresponding layers in the DFC treatment group (P > 0.05). The same effect was evident in the hypodermis layer; however, the values did not reach statistical significance (Fig. 3B).

Treatment effects on tissue architecture. Skin samples from each treatment group were harvested at day 7 and at day 20, fixed, sectioned, and stained with hematoxylin and eosin.
Moreover, results from day 7 post-injection showed that cell treatment had no significant effects, relative to the PBS/DMSO control group or to each other, in the tissue architecture of wounds. The only effects seen at day 7 were a significant hypertrophy of the hypodermis layer in wounds treated with cryopreserved ASCs relative to wounds treated with fresh ASCs and DFCs and a significant reduction of the muscle layer of wounds treated with fresh ASCs and cryopreserved ASCs relative to DFC-treated wounds (P < 0.05) (Fig. 3A). However, at day 20 post-injection, both the fresh and cryopreserved ASC groups showed a significant reduction in depth within all layers relative to the corresponding layers in the DFC group (P < 0.05) (Fig. 3B). Differences relative to the PBS/DMSO control group were noted as a reduced epidermal layer in fresh and cryopreserved ASC-treated wounds (Fig. 3B). Otherwise, there was no significant difference in architecture between fresh and cryopreserved ASC treatments at day 20 post-injection.
Histological determination of tissue architecture in old immunocompetent mice exposed to fresh or cryopreserved ASCs relative to controls (PBS/DMSO)
Histological analyses of tissue architecture in old mice (22-month-old both female and male) demonstrated that at day 7 post-injection the depth of the epidermal and muscle layer in wounds treated with fresh ASCs was significantly reduced relative to the corresponding layers in wounds treated with the control treatment (Fig. 3C). Additionally, wounds treated with cryopreserved ASCs showed a significant decrease in epidermal layer thickness relative to the control treatment and a significant hypertrophy of the muscle layer relative to that of wounds treated with fresh ASCs (Fig. 3C). In contrast, at day 20, wounds treated with fresh ASCs showed a significant hypertrophy of the epidermal, dermal, and muscle layer relative wounds treated with the control treatment (Fig. 3D). In the case of wounds treated with cryopreserved ASCs, the depth of the epidermal and dermal layers was significantly reduced relative to wounds treated with the control treatment (Fig. 3D). Finally, the only differences between cell treatments were a reduction of the depth of the dermal layer in wounds treated with cryopreserved ASCs relative to wounds treated with fresh ASCs (Fig. 3D).
Collagen deposition in young and old immunocompetent mice exposed to fresh or cryopreserved ASCs relative to controls (PBS/DMSO or DFCs)
Collagen deposition was determined based on Masson's trichrome staining using CellProfiler. Results of these analyses in young mice showed that there was no significant effect of cell treatment on the amount of collagen present in wounds relative to wounds treated with PBS/DMSO control. Significant effects on collagen deposition in young mice were only seen in comparisons between DFC treatments relative to either PBS/DMSO control treatments or cryopreserved ASC treatments (P < 0.05) (Fig. 4A). In contrast, these analyses showed no significant change in collagen deposition between any of the treatments in wounds of old mice (Fig. 4B).

Collagen deposition in pressure ulcer skin wounds. Skin samples from each treatment group were harvested, fixed, section, and stained with Masson's trichrome. Collagen deposition was determined by measuring the ratio of blue-stained area to the total photomicrograph tissue area.
CD68 expression upon delivery of fresh or cryopreserved ASCs and PBS/DMSO in young and old immunocompetent mice
To evaluate immune responses associated with injection of fresh or cryopreserved ASCs relative to PBS/DMSO, the localization and abundance of CD68 were determined as a general macrophage marker (Fig. 5). Immunohistochemical detection of CD68 showed the accumulation of the cell signal (brown reaction product) throughout the dermal part of the skin and in the vicinity of blood vessels and adipocytes (Fig. 5). Comparison of the macrophage presence in ASC-treated wounds at different stages of healing determined a stronger CD68 expression during the inflammatory phase at day 7 (Fig. 5A) relative to the remodeling phase at day 20 post-injection (Fig. 5B) regardless of sex. Analysis of skin tissues at day 7 showed strong CD68 signal within the dermis, blood vessels, and adipose tissues, whereas at day 20, majority of macrophages were detected predominantly in blood vessels (compare Fig. 5A and B). With regard to CD68 expression in the context of sex, the histological detection demonstrated the abundant presence of tissue macrophages in the skin sections from females treated with fresh ASCs at day 20 post-injection (Fig. 5C), whereas in males, macrophages were located predominantly around vessels (Fig. 5D). Interestingly, the most robust CD68 staining was detected in tissues treated with DFC (Fig. 5E), regardless of sex or day after injection (day 7 vs. day 20). DFC-injected wounds showed strong CD68 expression spread throughout the entire dermis and located to blood vessels and adipocytes (Fig. 5E). In contrast, the weakest CD68 signal was detected in control tissues administrated with DMSO (Fig. 5F) or PBS (Fig. 5G) where CD68 signal was localized around blood vessels.

Immunohistochemical detection of CD68 in the pressure ulcer skin wounds. Skin specimens collected from male
Discussion
This laboratory previously showed that culture-expanded syngeneic murine ASCs accelerated pressure injury wound healing in young female immunocompetent mice [3,13]. Transgenic green fluorescent protein-tagged murine ASCs integrated within the adipose and dermal layers of regenerated skin [3]. The current data extend these observations by providing proof-of-principle evidence supporting the following conclusions regarding the use of human adipose-derived cells isolated using a closed system device designed for clinical translation: Culture-expanded human ASCs implanted safely into pressure-injured young or old immunocompetent mice of both sexes. The use of DMSO as a cryoprotective agent was tolerated by young and old immunocompetent mice. Freshly cultured and cryopreserved human ASCs significantly accelerated pressure injury wound repair in young male and female immunocompetent mice relative to untreated or DFC-treated controls. Freshly cultured and cryopreserved human ASCs significantly accelerated pressure injury wound repair in older immunocompetent mice relative to untreated controls at intermediate time points but displayed no significant effect by the conclusion of the study period (day 20). Cell therapy increased CD68+ cell infiltration into the wound site during the early (day 7) in the inflammatory phase, particularly within the adipose layer; however, cell therapy reduced CD68+cell infiltration later (day 20) during the remodeling phase.
These outcomes have potential relevance for the use of allogeneic culture-expanded ASCs as an off-the-shelf product. Additionally, these findings are consistent with a report on the effect of a lyophilized human microvascular tissue when applied topically or injected into the murine pressure injury model [37]. Both delivery approaches of the microvascular tissue-derived therapeutic accelerated wound healing comparably to human or murine ASC injection [3,37]. Similarly, a recent study demonstrated that transplantation of autologous ASC in a rat soft tissue wound model significantly accelerated skin healing [38]. Likewise, an independent study previously evaluated the application of human ASCs in the form of a three-dimensional spheroid to a full-thickness skin wound model in young immunocompetent mice. The ASC spheroid therapy was found to improve regeneration in diabetic, but not control, mice, presumably through the dose-dependent paracrine release of anti-inflammatory cytokines [28].
Likewise, an emerging body of literature has examined the safety and efficacy of adipose tissue grafting, alone or supplemented with SVF cells and/or platelet-rich plasma, in the treatment of burns and scars [39,40]. While these studies indicate benefits, which are attributed in part to the regenerative properties of the SVF cells, the study designs have been limited to case–control or case report analyses and there remains a need for randomized controlled trials [39,40]. Nevertheless, more recent studies in human subjects lend support to a potential therapeutic role for adipose-derived cells and products in the treatment of pressure injuries and related disorders. In a nonrandomized clinical study performed in Nicaragua, 10 patients with severe peripheral vascular disease in the presence of amputation or PU were injected into the afflicted limb intramuscularly and periarterially with autologous SVF cells [41]. In four of six subjects with associated PUs, the wounds healed spontaneously over an 8- to 10-month period [41]. In a similarly designed Lithuanian clinical study, 15 patients with peripheral vascular disease were treated with autologous SVF cells [42]. Within the subcohort of six patients with PUs, five displayed healing [42]. Likewise, clinical trials performed in France (7 patients) and South Korea (15 patients) used culture-expanded human ASCs to treat patients with critical limb ischemia [43,44]. The PUs displayed quantitative evidence of healing in 71% (France) and 66% (South Korea) of the afflicted patients [43,44]. While the mechanism of action for the human SVF cells and ASCs remains to be determined, the positive outcomes to date have been correlated with paracrine action of the injected cells [43,44]. Consistent with this, a recent randomized, controlled clinical trial treated diabetic foot ulcer patients (n = 114) undergoing minor amputations with either autologous microfragmented adipose tissue or standard-of-care therapy. While only 48% of the standard-of-care patients healed within 6 months, the healing rate reached 80% in the microfragmented adipose-treated cohort [45]. This published body of work, along with the current findings, lends support for continued clinical translational efforts exploring the use of adipose-derived cell therapy in ischemic pressure injuries.
While the current studies were designed to maximize the significance of the outcomes while reducing the need for in vivo animal studies, several limitations need to be acknowledged. First, the skin architecture varies between male and female mice and neither is identical to human skin. Consequently, it remains to be determined how well the histology observed in the murine PU model will predict the outcomes in human pressure injuries subsequent to adipose cell therapy. Indeed, the overall differences between the species may interfere with the accuracy of clinical translation from findings derived in the mouse when extrapolated to the human with respect to cell therapy. Nevertheless, the rodent model provides a logical starting point for investigation. While large animal models such as the pig may resemble human skin architecture more closely, such species will likewise face challenges with respect to human clinical translation due to biochemical, biomechanical, and genetic differences. Second, the contribution of sex as a biological variable warrants additional attention. Third, the current proof-of-principle study was performed using a cell dose modeled on prior analyses establishing the optimal efficacy using 106 murine ASC injection per wound site [3]. Further studies will be necessary to examine both the dose dependency and frequency of the human ASC therapy. Finally, there remains a need to further explore the adipose cell-derived factors (cytokines, exosomes, microRNA) responsible for the paracrine mechanisms promoting wound regeneration and repair.
Conclusions
This work demonstrates the safety and potential efficacy of fresh and cryopreserved human ASCs injected into an immunocompetent murine pressure injury model. The findings suggest that delivery of allogeneic ASCs culture expanded and cryopreserved under a current Good Manufacturing Practices (cGMP) methodology will have utility in the treatment of human patients with pressure injuries refractory to current standard of care. These findings are paralleled by studies from our laboratory demonstrating the safety of human SVF cells prepared with the closed system device when employed in the identical murine PU model [46]. Further clinical trials performed in accordance with U.S. Food and Drug Administration guidelines will be necessary to translate these findings from the laboratory to the patient.
Footnotes
Acknowledgments
The authors thank Dr. James Wade (Baton Rouge LA), his patients, and staff for their informed consent to donate tissue in support of this project.
Author Disclosure Statement
A.A.U. is an employee of LaCell and Obatala Sciences. J.M.G. and X.W. are co-founders and co-owners of LaCell and Obatala Sciences as well as members and executives of LaCell. T.F. is co-founder, co-owner, and President/CEO of Obatala Sciences and a former LaCell employee. P.K. is an executive at Tissue Genesis LLC. All other authors declare no conflicts of interest.
Funding Information
Funding for the study was provided by the National Institute of Aging Phase II SBIR R44AG042904 “Adipose-Derived Stromal/Stem Cell Therapy for Pressure Ulcers.” J.B. visit to the Tulane University was funded by a postdoctoral fellowship from the KNOW Consortium “Healthy Animal—Safe Food,” MS&HE Decision No. 05-1/KNOW2/2015.