
Abstract
Pressure ulcers (PUs) result in part due to ischemia–reperfusion injury to the skin and present frequently in elderly or quadriplegic patients with reduced mobility. Despite the high economic and societal cost of this condition, PU therapy relies primarily on preventive strategies and invasive surgical intervention. A growing body of clinical literature suggests that localized injection of adipose-derived cells can accelerate and enhance the closure of PUs. The current study systematically evaluated the safety of human adipose stromal vascular fraction (SVF) cells isolated using a closed system device when injected into a murine PU injury model. The human SVF cells were characterized by colony-forming unit–fibroblast and differentiation assays before use. Young (2 months) immunocompetent C57BL/6 mice subjected to a magnet-induced ischemia–reperfusion injury were injected subcutaneously with human SVF cells at increasing doses (0.25–2 million cells). The size of the PU was monitored over a 20-day period. Both female and male mice tolerated the concentration-dependent injection of the SVF cells without complications. While male mice trended toward more rapid wound closure rates in response to lower SVF cell concentrations (0.25–0.5 million cells), female mice responded favorably to higher SVF cell concentrations (1–2 million cells); however, outcomes did not reach statistical significance in either sex. Overall, the study demonstrates that human SVF cells prepared with a closed system device designed for use at point of care can be safely administered for PU therapy in an immunocompetent host animal model.
Introduction
Pressure ulcers (PUs) commonly complicate the care of bed-ridden patients including younger individuals with paraplegia or quadriplegia and elderly individuals living in nursing homes [1 –3]. This condition accounts for up to 4% of the health care expenditures in developed countries and costs in excess of $26 billion in the United States alone [4,5]. It is postulated that ischemia–reperfusion episodes account for the causative mechanism of PU injuries, leading to lesions ranging from damage limited to the epidermis (Stage 1) to those involving the epidermis, dermis, adipose tissue, skeletal muscle, and bone (Stage 4) [6]. Currently, clinicians have focused primarily on preventive measures such as frequent turning of patients and the use of foam or liquid supports under body surfaces at risk for damage (heels, elbows, sacrum) to reduce PUs in at-risk populations [7,8]. However, once a PU develops, treatment options rely on surgical interventions such as debridement or negative pressure wound therapy.
A limited number of clinical studies have suggested that cell therapy offers an alternative therapy for PUs and related skin injuries, such as burns and full-thickness wounds [9 –13]. Four recent clinical studies have reported outcomes following treatment of critical limb ischemia with autologous adipose-derived stromal vascular fraction (SVF) cells in a total of 47 patients [14 –17]. The intramuscular or periarterial injection of the SVF cells led to enhance the rate of repair in skin wounds for up to 70% of the patients [14 –17]. While these findings are promising, there remains a need to additional, controlled clinical trials to document the safety and efficacy of adipose-derived SVF cells in the treatment of PUs. In a clinical setting, it will be optimal for the surgical team to use a closed system device designed for the isolation of autologous SVF cells from the patient's own adipose tissue at the point of care [18].
To further develop improved PU therapies, investigators have performed preclinical animal studies to evaluate the utility of cell therapies to accelerate skin wound healing. Stadler et al developed a simple murine PU model that relies on the sequential external placement of magnets across the animal's dorsal skin to create periods of ischemia–reperfusion [19]. Our laboratory and others have employed this murine magnetic-induced PU model to explore the regenerative properties of culture-expanded cells or extracts from adipose tissue or bone marrow as well as growth factor containing scaffolds [20 –24]. In the past, the safety and efficacy of human mesenchymal stem cell (MSC) were examined using immunodeficient nonobese diabetic/severe combined immunodeficiency murine strains [23]. While such an approach avoided the complications due to xenotransplantation, it failed to examine the safety of the cell therapy in the context of a functional and intact immune system. Therefore, the current study has employed an immunocompetent murine PU model to examine the safety of human SVF cells isolated using a closed system device as a potential therapeutic option.
Materials and Methods
Animal purchase and ethics
Studies were performed under a protocol reviewed and approved by the Tulane University Institutional Animal Care and Use Committee (IACUC) (Protocol no. 4313R entitled “Adipose-Derived Stromal/Stem Cell Therapy for Pressure Ulcers”). Male and female C57BL/6 mice (8 weeks old; Charles River Laboratory, Wilmington, MA) were quarantined (1 week) and housed in the Tulane University Department of Comparative Medicine Vivarium (an Assessment and Accreditation of Laboratory Animal Care [AAALAC] International certified facility under the veterinary supervision of Gina Dobek DVM) with ad libitum access to water and chow under a 12-h light:12-h dark schedule. At the end of the study, mice were euthanized by CO2 asphyxiation in accordance with American Veterinary Medical Association (AMVA) guidelines and recommendations.
Reagents
All reagents were purchased and obtained from Thermo Fisher Scientific (Waltham, MA), unless otherwise stated.
Human adipose tissue acquisition (institutional review board)
Study protocols were reviewed and approved by the Western Institutional Review Board (Puyallup, WA) (Study no. 1138160) with inclusion criteria: patients aged ≥18 years, male or female, undergoing elective cosmetic or reconstructive procedures, and exclusion criteria: patients with viral infectious diseases, cancer (other than basal cell carcinoma of the skin), or pregnancy.
Human adipose tissue Icellator processing
Sixty milliliter volumes of tissue was processed in the Tissue Genesis Icellator® (Tissue Genesis, Houston, TX) closed system instrument using the Adipase® enzyme (Tissue Genesis) to yield SVF cells in accordance with the manufacturer's instructions. Briefly, 60 mL of lipoaspirate was obtained from elective liposuction procedures. The Icellator was prepared by loading the disposable kit, enzyme solution, and a 250-mL sterile infusion bag of Ringer's lactate solution (Braun Medical, Bethlehem, PA) as per the manufacturer's instructions (Tissue Genesis). The operator then initiated the Icellator preprogrammed cycle for automated SVF cell isolation. The Icellator operates by incubation of the lipoaspirate with an enzymatic solution, followed by centrifugation and washing of the resultant cell product. At the end of the cycle, SVF cells were available within a syringe for collection in a final volume of 30 mL. The resulting SVF cells were concentrated by centrifugation at 1,200 rpm (300g) for 5 min at room temperature (Sorvall; Beckman Coulter, Indianapolis, IN) and evaluated using a live/dead calcein/ethidium bromide fluorescent assay (LaCell LLC, New Orleans, LA) for viability and concentration before being injected immediately into the murine PU model or cryopreserved in liquid nitrogen for future thawing to allow for culture expansion of adipose-derived stromal/stem cells (ASC) according to published methods [25].
Colony-forming unit–fibroblast assay
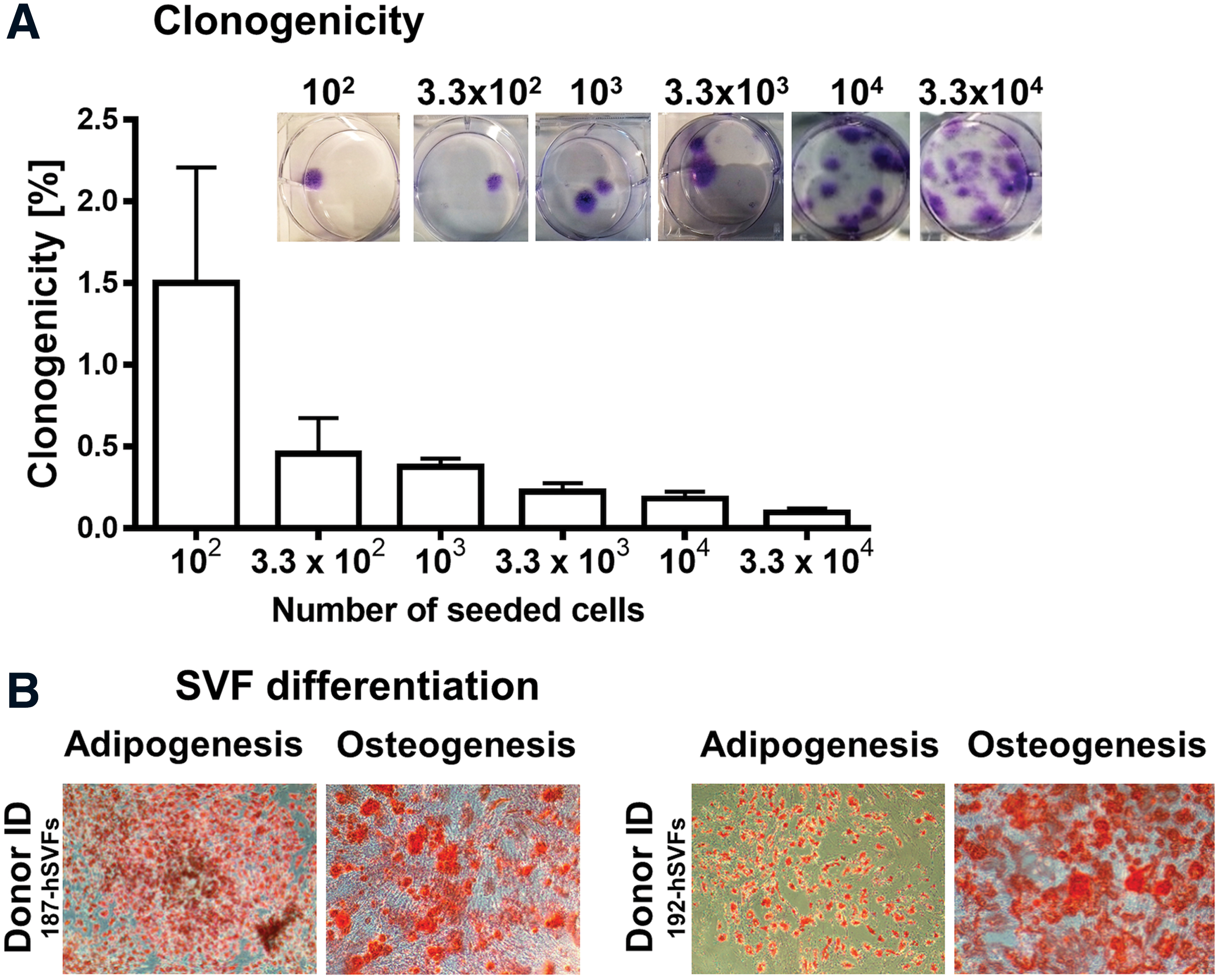
Freshly thawed vials of SVF cells were seeded in duplicate six-well plates at densities of 102, 3.3 × 102, 103, 3.3 × 103, 104, and 3.3 × 104 SVF cells per well (n = 2 donors). Wells were fixed at 12–14 days with 4% formaldehyde, stained with Toluidine blue, and colonies of >50 cells counted, as previously described [26].
Differentiation
At 80%–90% confluence, cells were induced with either AdipoQual™ or OsteoQual™ medium for adipogenesis and osteogenesis, respectively. Representative cultures were fixed and stained for lipid accumulation with Oil Red O (adipogenesis) or with Alizarin Red to depict calcium deposits (osteogenesis). Photomicrographs were obtained using Motic Image 3.0 software.
Flow cytometry
Flow cytometry was performed using cryopreserved SVF cells isolated using the Icellator from a single donor as described previously [27,28].
PU model
PU injuries were created on the dorsal skin of immunocompetent C57BL/6 mice (2 months old, male and female) using externally placed magnets (Master Magnetics Inc., Castle Rock, CO) as previously described [20 –22]. Freshly isolated human SVF cells prepared from individual donors (0.25–2.0 × 106 cells suspended in a volume of 100 μL) were injected subcutaneously using a 22-gauge needle into the base of each individual PU wound approached from the intact skin at the edge of the lesion through a single injection site; the injection site was sealed immediately with Vetbond Tissue Adhesive (3M, Maplewood, MN) to prevent leakage (Fig. 1). Wound size dimensions were monitored daily for up to 20 days as described previously [3 –5]. After 20 days, mice were euthanized by CO2 asphyxiation. The skin and underlying tissue in and around the PU wound sites were resected surgically and divided into two equal halves vertically along the anterior/posterior axis. One half of each tissue was placed in a cassette for formalin fixation, paraffin embedding, and subsequent sectioning and staining. The second half of each tissue was placed in a sealed tube and stored at −80°C for future isolation and processing.
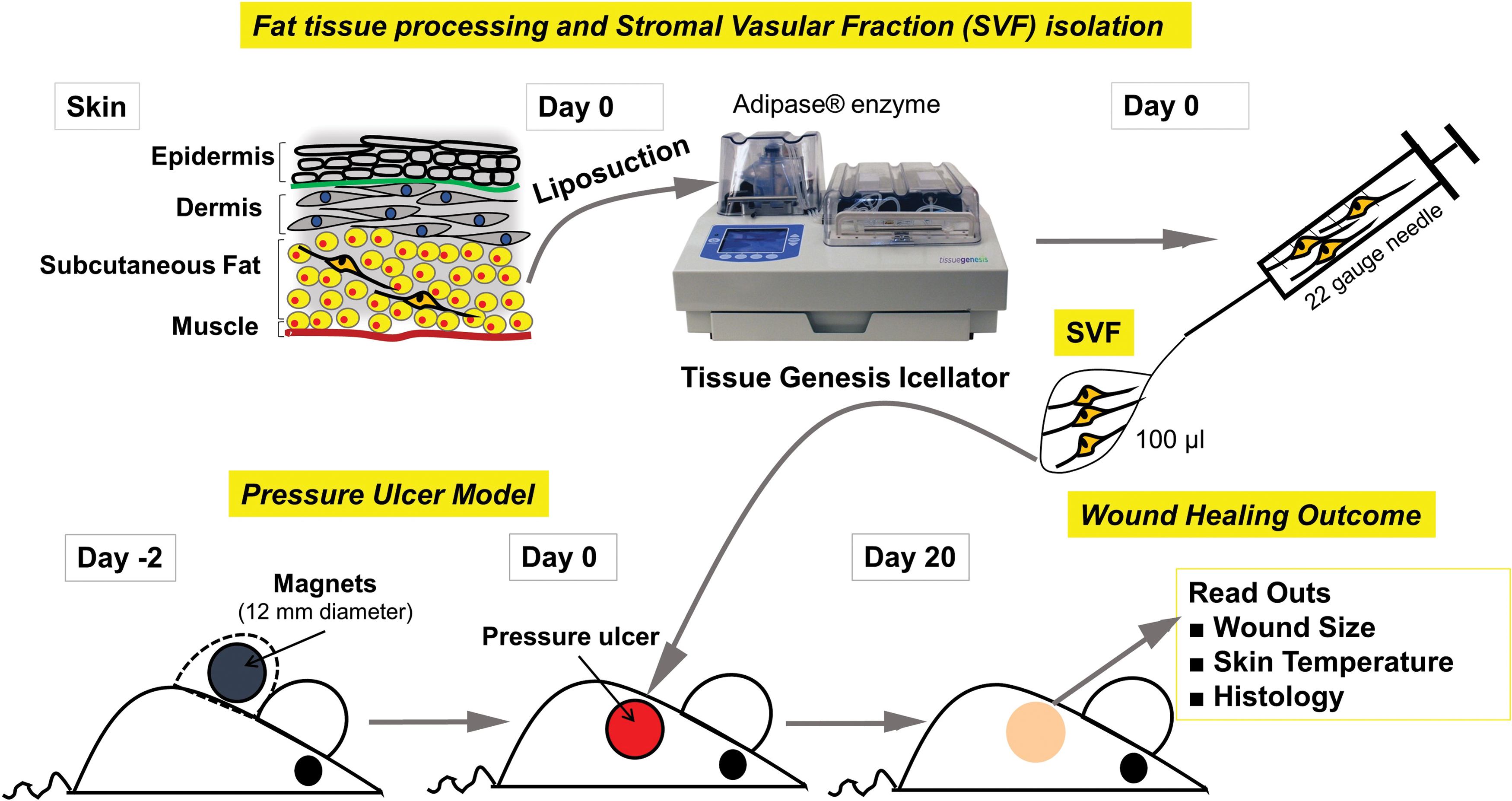
Experimental protocol. Freshly isolated SVF cells were injected subcutaneously into the PU injuries in young and old mice of both sexes and monitored daily for wound size and temperature over a 20-day period. PU, pressure ulcer; SVF, stromal vascular fraction. Color images are available online.
Histology analysis
Skin sections from wounds were stained with Masson's trichrome (ScyTek Laboratories, West Logan, UT). The Masson's trichrome sections were scanned with PrimeHisto XE Histology slide scanner (Carolina Biological Supply Company, Burlington, NC) and analyzed for depth of epidermis, dermis, subcutaneous adipose layer, and muscle layer at three different sections of the wounded skin with measurements performed using the ImageJ (NIH, Bethesda, MD) software as previously published [20]. Photomicrographs from Masson's trichrome-stained sections were photographed with a Motic microscope digital camera (Hong Kong, China) and analyzed for collagen expression with Cell Profiler (Cambridge, MA) based on blue staining relative to the total photomicrograph tissue area. Immunofluorescence was performed according to published methods [29].
Immunofluorescence analysis of CD68
Immunofluorescence procedures were performed on formalin-fixed skin specimens embedded in paraffin, sectioned, and processed using the primary antibodies against CD68 (AbCam, Cambridge, MA) at the concentrations 1:400. Secondary antibodies labeled with Alexa Fluor 594 (Life Technologies, Carlsbad, CA) were used, and nuclei were counterstained with ProLong® Gold antifade reagent with 4′,6-diamidino-2-phenylindole (DAPI) (Life Technologies). Confocal images were scanned and digitalized using an F10i-LIV Laser Scanning Microscope integrated with OLYMPUS CellSens Dimension Desktop 2.2. Software (Olympus, Center Valley, PA).
Statistics
Statistical analyses were performed using GraphPad Prism Version 6.02 software (San Diego, CA). Comparisons were performed between groups using two-tailed Student's t-test. Values are reported as the mean ± standard deviation (SD) where statistical significance was determined based on P ≤ 0.05.
Results
Characterization of human SVF cells
Processing of 60 mL of human adipose tissue lipoaspirate yielded a mean of 36.0 ± 20.3 million total SVF cells (n = 3 donors) with a mean viability of 64.5% ± 11.4% (Table 1). These isolated SVF cells were further characterized based on differentiation and colony-forming unit–fibroblast (CFU-F). The SVF cells (n = 2 donors) were seeded at different initial densities to generate single cell-derived CFUs (Fig. 2A). The CFUs comprised two types of colony: large, densely packed or smaller, loosely arranged. The large colonies containing >50 cells were considered to display high proliferation capacity derived from a single SVF cell, and they were employed to estimate cloning efficiency (CE) determined from the formula CE (%) = (number of colonies/number of cells seeded) × 100. The CE of human SVF cells was 1.5% ± 0.70%, 0.45% ± 0.22%, 0.38% ± 0.05%, 0.23% ± 0.05%, 0.18% ± 0.04%, and 0.09% ± 0.02% for initial cell densities of 102, 3.3 × 102, 103, 3.3 × 103, 104, and 3.3 × 104 per well, respectively (Fig. 2A). Moreover, to investigate human SVF cell multipotency manifested by the capacity to differentiate into mesenchymal lineages, cells were cultured in adipogenic or osteogenic differentiation–induction media for 14 days (n = 2). The SVF cells demonstrated lipid accumulation and mineralization based on Oil Red O (Fig. 2B) and Alizarin Red (Fig. 2B) histochemical staining, respectively. Flow cytometry analysis performed on cryopreserved SVF cells from a representative donor demonstrated expression of the following surface antigens: CD29 (90%), CD34 (75%), CD44 (33%), CD45 (44%), CD73 (41%), CD90 (78%), and CD105 (50%).
Characterization of culture-expanded human adipose-derived SVF cells.
Overview on the Efficiency of Stromal Vascular Fraction Isolation by Using the Tissue Genesis Icellator
SVF, stromal vascular fraction.
Impact of human SVF cells on PU healing in young immunocompetent mice
Initial studies evaluated the effect of human SVF cells on PU wounds in young (2 months old) immunocompetent female and male mice. In keeping with the recent NIH guidelines regarding sex as a biological variable, all treatment groups included equal numbers of female and male mice [30]. As controls, wounds were treated with sterile phosphate-buffered saline (PBS) and monitored daily. Both female (n = 7) and male (n = 7) control cohorts demonstrated gradual wound closure between post-treatment days 0 and 8 with wound size reductions of 55.54% ± 16.32% (P < 0.0001) and 55.18% ± 11.40% (P < 0.0001), respectively (Fig. 3). Interestingly, females showed faster scab removal than males. This process started in females at post-treatment day 8, whereas males delayed scab shedding until post-treatment day 10 (Fig. 3). From days 10–11, the ratio and the pattern of wound closure were comparable between female and male control cohorts and resulted in complete closure at post-treatment day 20 (P < 0.0001, for both sexes). To assess the therapeutic dose of human SVF cells favorable for the healing of PUs, young (2 months old) female (total of n = 19) and male (total of n = 19) mice were injected with different concentrations of freshly isolated SVF cells: 2.5 × 105, 5.0 × 105, 1.0 × 106, and 2.0 × 106 cells per wound (n = 3–5 mice per SVF cell treatment subgroup) (Fig. 4). Following injection of cells, PUs were daily monitored. Female mice treated with high SVF cell doses (1.0 × 106 and 2.0 × 106; Fig. 4C, D, respectively) demonstrated a trend toward accelerated wound closure relative to PBS administration; however, the data did not reach statistical significance. The enhancement of wound healing was manifested by more rapid wound contraction and closure after scab removal during post-treatment days 8–12 (Fig. 4C, D). Delivery of low SVF cell doses (2.5 × 105 and 5.0 × 105; Fig. 4A, B, respectively) had no effect on PUs healing in female mice. In contrast to females, male mice treated with low doses of SVF cells (2.5 × 105 and 5.0 × 105; Fig. 4A’, B’, respectively) showed a trend toward accelerated wound closure. Indeed, the trend to SFV cell-enhanced reduction of wound size was evident by post-delivery day 10 (24.57 and 37.44 mm2; for the cell dose of 2.5 × 105 and 5.0 × 105; respectively; Fig. 4A’, B’) when compared with PBS-injected wounds. This accelerated healing continued until complete wound closure at day 13 (Fig. 4A’). In contrast, the highest SVF cell concentration (2.0 × 106 cells/wound) in male mice resulted in significant inhibition of PU closure at post-treatment day 12 (P < 0.05; Fig. 4D’) relative to PBS-administrated tissues. Overall, these data underscore sex-related discrepancies between female and male mice in the context of human SVF cell effectiveness, particularly stressing the impact of cell dosage on therapeutic outcomes.

The differences in PU healing between young male and female immunocompetent mice treated with PBS alone. PU wounds were formed on the dorsal skin of young (2 months old) female (n = 7) and male (n = 7) mice and were further administrated with PBS. Macroscopic evaluation of wound healing presented as the morphometrical measurements of the wound closure (mm2). The results are shown as the mean ± SD. The asterisk indicated significant differences between day 0 (initial wound size) and post-treatment days 8 and 20 in a group of females, ****P < 0.0001. Hashes indicated significant differences between day 0 (initial wound size) and post-treatment days 10 and 20 in a group of males, #### P < 0.0001. PBS, phosphate-buffered saline. Color images are available online.
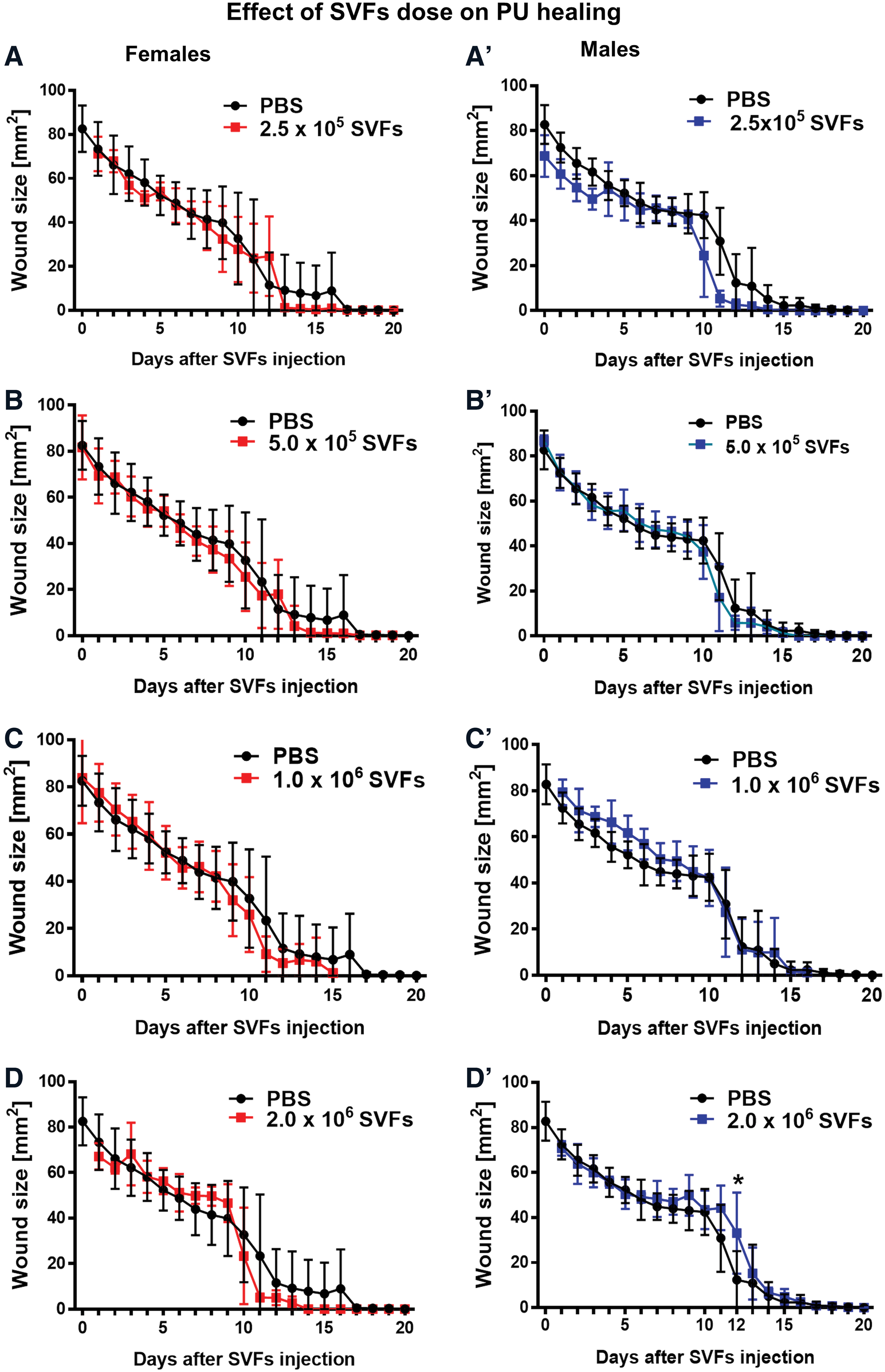
Female and male recipient response to human SVF cell injection. PU wounds created on the dorsal skin of young (2 months old) female (total of n = 19) and male (total of n = 19) mice were injected with different concentrations of SVF cells.
Wound site tissue sections were stained with Masson's trichrome to assess the skin histological architecture as a function of SVF cell therapy (Fig. 5). Regardless of the SVF cell concentration delivered to wounds, no effects were observed in terms of the thickness of individual skin layers (epidermis, dermis, hypodermis) for either female or male cohorts (Fig. 5A–D). Only a single histological site responded to SVF cell treatment with respect to its thickness; specifically, the SVF cell administration at a dose of 5.0 × 105 to the site of injury increased the thickness of the subdermal muscle layer in female but not male mice (P < 0.05) at post-treatment day 15, relative to PBS-treated wounds (Fig. 5D). These data suggest that human SVF cells contribute to PU healing in female mice predominantly by their contribution to the muscle restoration and skin tissue contraction, the primary mechanism driving subcutaneous wound healing in rodents.
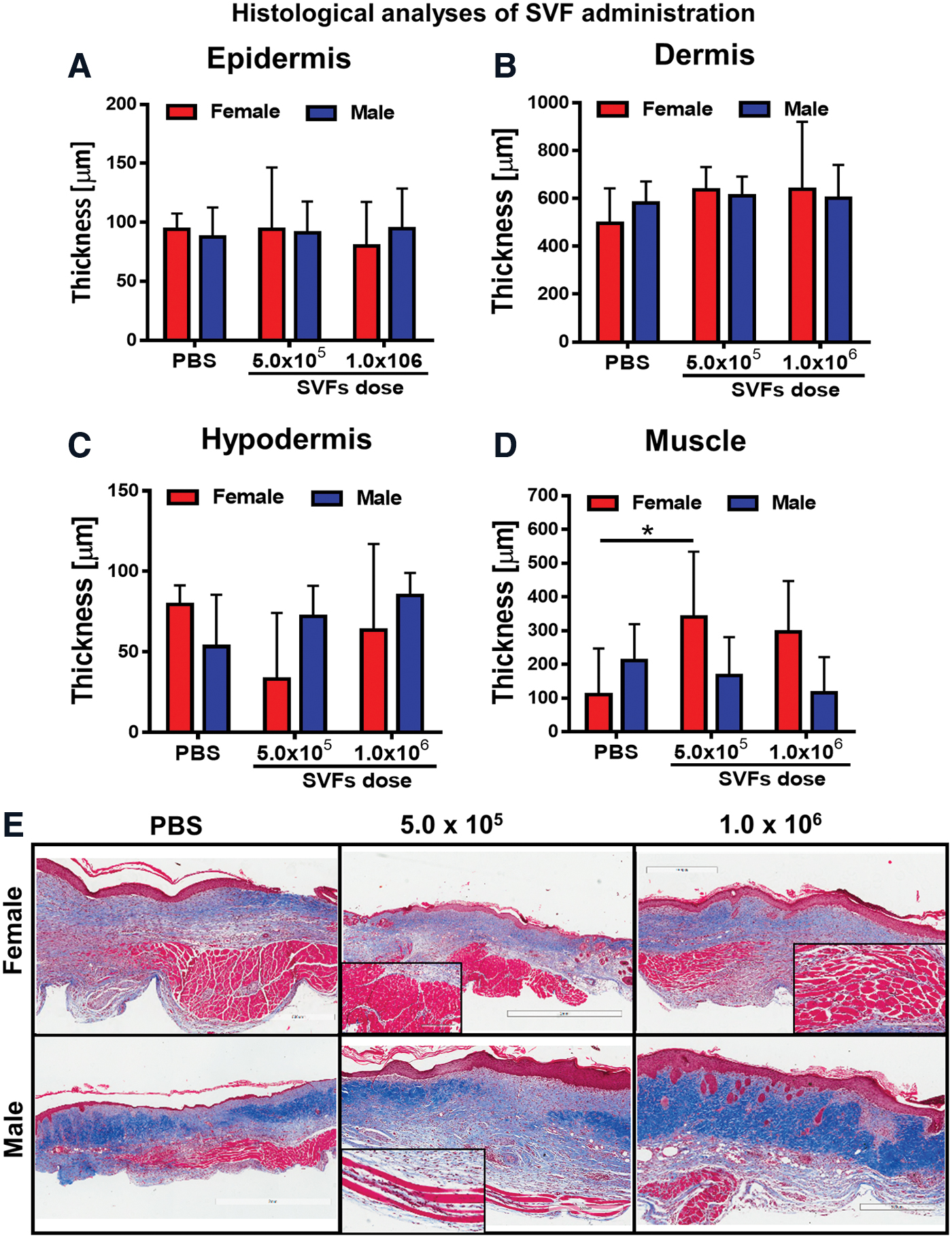
Human SVF cells affect post-injured skin architecture. PU wounds created on the dorsal skin of young (2 months old) female (n = 9) and male (n = 9) mice were injected with different dose of SVF cells 5.0 × 105, 1.0 × 106, and PBS (used as control). Wounds were collected (n = 6 wounds per group) after 15 days. Morphometric analysis of skin sections demonstrates thickness of
Collagen content analysis measured using Masson's trichrome staining revealed a significant increase in the protein deposition in tissue sections collected from males relative to females (P < 0.0001 for PBS administration, P < 0.05, P < 0.0001 for 5.0 × 105 and 1.0 × 106 SVF cells injected, respectively, Fig. 6A, B). Treatment with SVF cells has no effect on collagen deposition and its arrangement in PU wounds either in females (Fig. 6B, upper panel) or in males (Fig. 6B, lower panel) when compared with PBS-treated group. However, regardless of the type of treatment (PBS or SVF cells), there were substantial differences in collagen amount and its arrangement between the sexes (Fig. 6C). In male wounds, the tissue displayed an abundant collagen amount with wide and disoriented bundles. In contrast, thicker and well-oriented collagen fibers were found in specimens collected from female counterparts (Fig. 6C). Together, these data indicate that the level of subcutaneous collagen deposition, consistent with fibrosis, is greater in male relative to female mice but is not significantly impacted within the wound sites as a function of SVF cell therapy. This sex-dependent histological difference is accompanied by the increased presence of subdermal capillary vasculature in male skin relative to female skin.
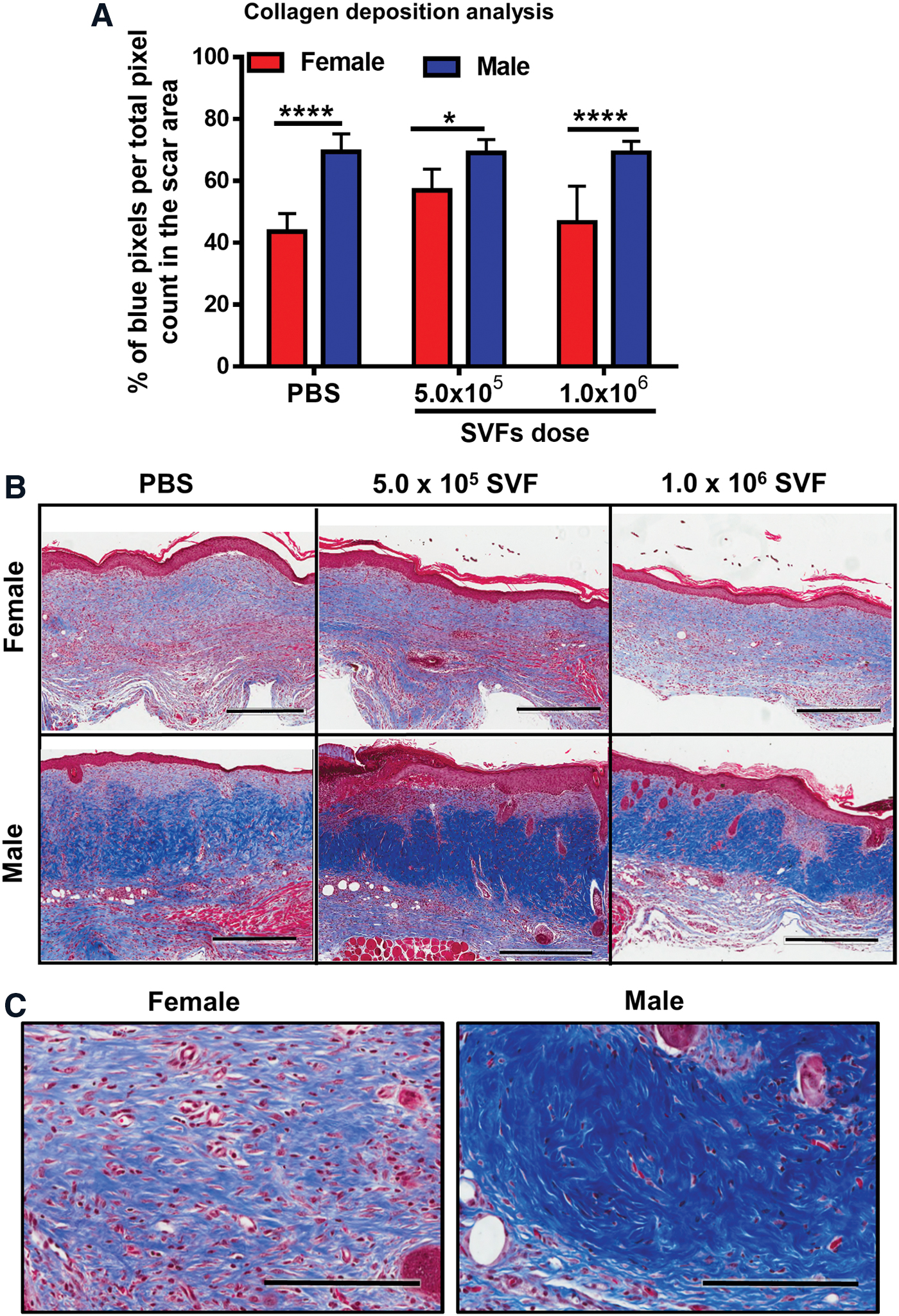
Collagen content and its arrangement in scar tissue of PUs.
CD68 expression upon delivery of SVF cells in young immunocompetent mice
To evaluate immune responses associated with injection of SVF cells (Fig. 7), the level of CD68 was determined as a general macrophage marker. Twenty days after treatment, immunofluorescent analyses revealed evidence of CD68+ cell infiltration into the dermis of control PBS-treated mice. While the level of CD68+ cell infiltration was comparable at lower (0.5 million) SVF cell treatments, the CD68+ cell presence was reduced at higher SVF cell levels (1–2 million) in both female and male animals.
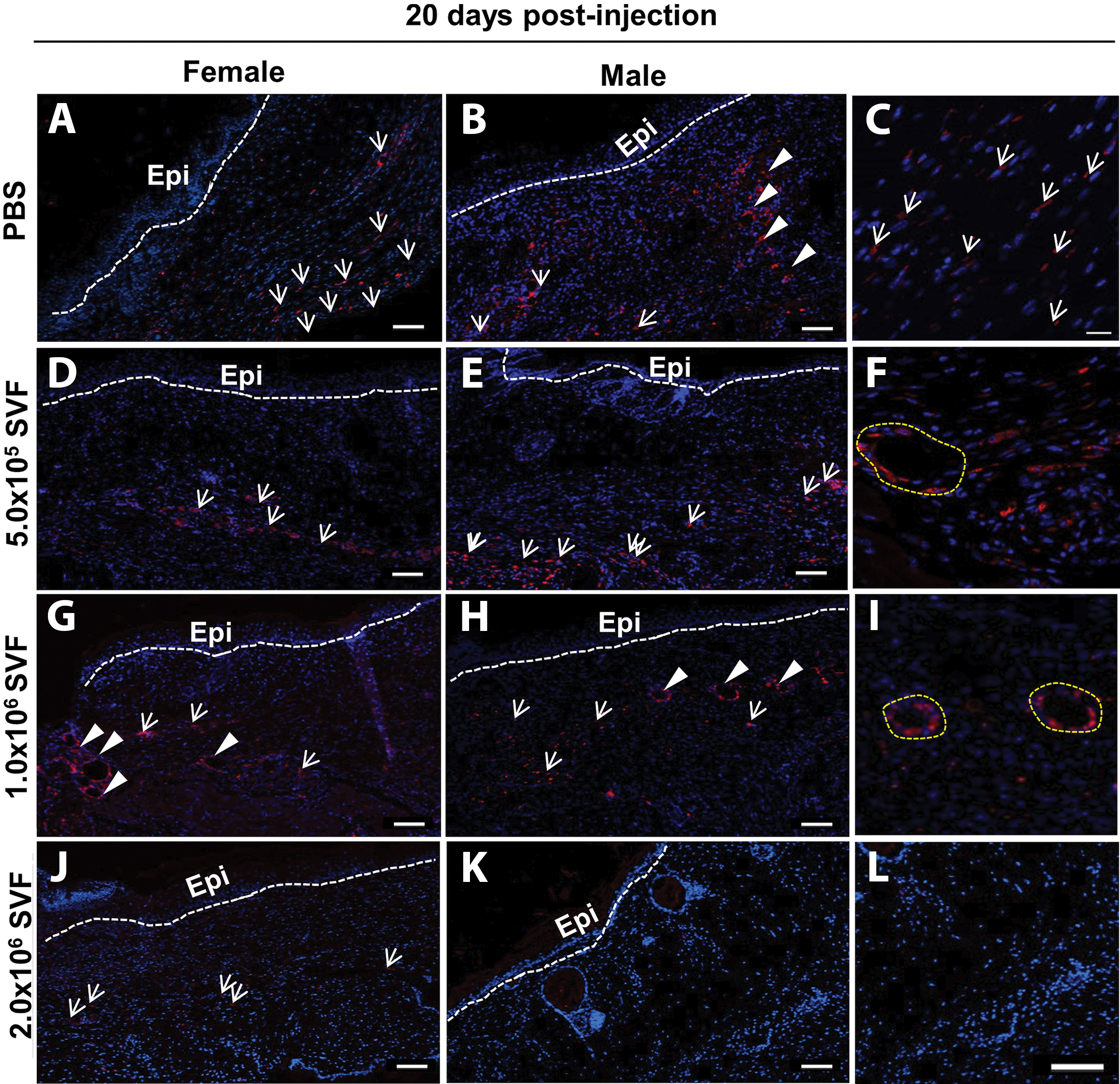
Immunofluorescent detection of CD68 in the PU skin wounds. Representative skin specimens collected from female or male mice injected with PBS
Discussion
The current study has determined that female and male C57BL/6 mice with intact immune systems tolerated the subcutaneous injection of increasing concentrations of human SVF cells. The human SVF cells were isolated using a closed system device designed for use at point of care. The resulting SVF cells displayed characteristics and viability consistent with recommendations for clinical applications [31]. Together, these data document the safety of human SVF cells in a preclinical PU model and lay a foundation for advancing adipose-derived cell therapies in patients.
The murine PU model was first developed by Stadler et al. and subsequently has been adopted as a simple yet effective pathophysiological representation of ischemia–reperfusion injury [19]. The model is applicable to hairless (nude), hirsute, and obese mice, and the length of the healing period is reported to be extended by prior exposure to low-dose irradiation but not to diabetes [23,32,33]. Multiple investigators have employed the PU model to evaluate the safety and efficacy of cell therapy. Studies by de la Garza-Rodea et al. reported short-lived survival and limited in situ differentiation of human MSC in a nude mouse PU model [23]. In contrast, Yoon et al. reported improved healing and enhanced vascularity following injection of human embryonic stem cell-derived MSC into PU lesions through a mechanism attributed to fibrocyte differentiation [34]. Similar outcomes have been reported in work using murine-derived primary cells. Motegi et al. found that dermal injection immediately after PU injury of syngeneic murine bone marrow-derived MSC reduced wound area size and increased vascularity in immunocompetent (C57BL/6) mice [35]. Similar outcomes were reported by Strong et al. in the C57BL/6 PU model following injection of syngeneic ASC [20,21]. The current work examining the safety and efficacy of human SVF cells confirms and extends the prior body of literature involving the murine PU model.
While not designed explicitly to compare the SVF cell response between the sexes, the cohorts in the current study included both female and male mice in accordance with the recent NIH guidelines [30]. In this context, it is noteworthy that the skin architecture differs between females and males. The dermal and skeletal muscle layers were thicker in the age-matched male mice relative to female mice. The trend in the wound closure outcomes suggests that the dose dependency of SVF cell therapy varies between female and male mice whereby females respond more robustly to higher SVF cell concentrations relative to males; however, the sample sizes were insufficient to achieve statistically significant results. Further studies focusing directly on the impact of host animal sex on the PU response to SVF cell therapy will be necessary. It must be noted that the logistics of coordinating fresh human adipose tissue acquisition with the timing of the PU induction process will be a considerable technical challenge for such a study design.
The current findings are relevant in the context of recent publications reporting potential benefits from autologous SVF cell injection on wound healing in patients with critical limb ischemia. Investigators in Lithuania used SVF cells to treat 15 peripheral vascular disease patients and noted healing in 5 of the 6 subjects with an existing PU or skin wound [15]. Likewise, investigators in Nicaragua treated a comparable cohort of 10 patients and noted healing of chronic skin wounds within 8–10 months in 4 of the 6 subjects with this complication [14]. Additional studies using culture-expanded ASC or microfractured adipose tissue grafting have documented similar improvements in wound healing [16,17,36]. The studies evaluating human adipose-derived cell therapies limited their design to a single treatment cohort and did not evaluate an equal number of randomized controls receiving current standard of care therapy [14 –17]. In contrast, the study evaluating microfractured fat therapy included both a control and treatment arm with a total enrollment of 114 subjects [36]. While these findings are promising, additional and larger randomized controlled studies advancing the quality of medical evidence will be necessary to substantiate safety, efficacy, and economy of adipose-derived cell therapy in PUs and related conditions [37]. Consistent with these clinical reports, the current study validates the feasibility of isolating human SVF cells using a closed system device, thereby yielding a product that can be safely injected into a preclinical PU model in an immunocompetent host. These findings complement parallel observations in the same animal model using culture-expanded human ASC prepared from SVF cells isolated with the closed system device [27]. It is anticipated that work will be extended in a future randomized, controlled clinical trial to evaluate the safety of autologous SVF cell therapy in patients with advanced PUs (n = 21 total), which has been allowed by the U.S. Food and Drug Administration.
Footnotes
Acknowledgments
The authors thank Dr. James Wade (Baton Rouge, LA), his patients, and staff for their informed consent to donate tissue in support of this project. The authors also thank Ms. Marilyn Dietrich at the Flow Cytometry Core Facility of the Louisiana State University School of Veterinary Medicine for her assistance.
Author Disclosure Statement
A.A.U. is an employee of LaCell LLC and Obatala Sciences, Inc. J.M.G. and X.W. are co-founders and co-owners of LaCell and Obatala Sciences as well as members and executives of both companies. T.F. is co-founder, co-owner, and President/CEO of Obatala Sciences and a former employee of LaCell. P.K. is an executive at Tissue Genesis LLC. All other authors declare no conflicts of interest.
Funding Information
Funding for this study was provided by the National Institute of Aging Phase II SBIR R44AG042904 “Adipose-Derived Stromal Stem Cell Therapy for Pressure Ulcers.” J.B. was funded by a postdoctoral fellowship from the KNOW Consortium “Healthy Animal—Safe Food,” MS&HE Decision No. 05-1/KNOW2/2015.