
Abstract
Although anthracycline (ANT)-based treatment strongly contributes to cancer survivorship, the use of these agents is limited by the risk of cardiotoxicity. For those patients who evolve to heart failure, myocardial regenerative approaches are of particular interest, and a growing body of preclinical studies has been investigating the use of cell therapy for ANT-induced cardiomyopathy (AIC). However, since animal models and modalities of cell therapy are highly heterogeneous between studies, the efficacy of cell therapy for AIC is not clear. Thus, we conducted a systematic review and meta-analysis of experimental studies reporting the use of cell therapy with mesenchymal stromal cells (MSC) or bone marrow mononuclear cells (BMMNC) in animal models of AIC with regard to global cardiac function. The Medline, EMBASE, and Web of Science databases were searched from inception to November 2019. Two reviewers independently extracted data on study quality and the results of left ventricular ejection fraction (LVEF) and fractional shortening (FS) obtained by echocardiography. The quality of outcomes was assessed using the Cochrane, Collaborative Approach to Meta-Analysis and Review of Animal Data from Experimental Studies (CAMARADES), and SYRCLE bias risk tools. Pooled random-effects modeling was used to calculate pooled mean differences (MD) and 95% confidence intervals (CIs). Twenty-two studies comprising 381 small animals (rabbits and rodents) were included. A pooled meta-analysis of all treatments showed that cell therapy increased LVEF by 9.87% (95% CI 7.25–12.50, P < 0.00001) and FS by 7.80% (95% CI 5.68–9.92, P < 0.00001) in small animals with AIC. Cell therapy with MSC/BMMNC is effective to mitigate the deleterious effects of ANT on cardiac function in preclinical models. Nevertheless, due to the small number of studies and considerable heterogeneity, future translational studies must be designed to diminish between-study discrepancies and increase similarity to the clinical landscape.
Introduction
Anthracyclines (ANT) are the most recommended class of antineoplastic agents to treat solid and hematological tumors. Because of its antineoplastic efficacy and low cost [1], doxorubicin (DOX) is the most prescribed ANT and is listed as an essential medication by World Health Organization (WHO) [2]. Regrettably, DOX treatment is associated with a plethora of unwanted effects, including general and organ-targeted toxicities, which range from hair loss to transient myelosuppression and cardiac toxicity [3,4]. ANT-induced cardiotoxicity (AIC) occurs in 9% of patients undergoing oncological treatment [5], ultimately leading to discontinuation of treatment. AIC is associated with multimorbidity with a significant potential to induce heart failure [6,7] AIC is currently considered a clinical dilemma and it represents a major unsolved issue both during and even several years following oncological treatment, mostly because of the growing incidence of cardiovascular disease (CVD) in cancer survivors [8].
ANTs, particularly DOX, exert their antineoplastic effects by several mechanisms, which include DNA intercalation, generation of bulky adducts and topoisomerase 2α (TOP2α) poisoning [9], with subsequent disruption of DNA and RNA synthesis [10]. However, DOX-induced cardiomyocyte death is mostly attributed to the generation of a massive amount of reactive oxygen and nitrogen species due to DOX metabolites and ferric cation (Fe3+) interactions and subsequent mitochondrial and energy metabolism disruption [11,12]. More recently, inhibition of TOP2β was described as a core mechanism of cardiomyocyte cell death [13,14].
With the improvement of cancer survival, the concerns with the risk of CVDs in this population have also increased [15,16]. This phenomenon has been attributed to the overlap between classical risk factors for cancer and CVD [17] and chemotherapy exposure [18]. In fact, cancer therapies, particularly chemotherapy, are now considered the key drivers of heart failure and cardiomyopathy in cancer survivors, and are likely to play a more prominent role than shared risk factors such as tobacco use and high body mass index [18]. In this sense, patients undergoing cancer treatment with a persistent absolute left ventricular ejection fraction (LVEF) decrease of >10% to <50% or >20% from baseline may have indication for cardioprotective therapies, temporary cancer treatment withholding or, if possible, noncardiotoxic second-line cancer treatments [19].
Pharmacological cardioprotective strategies, such as dexrazoxane and neurohormonal therapies (β-blockers, angiotensin receptor blockers, angiotensin-converting enzyme inhibitors), have been extensively investigated. Both therapies have been shown to reduce the risk of heart failure and cardiac events as recently reported in two meta-analyses [20,21]. However, while the use of dexrazoxane has been proven to be effective for children and metastatic breast cancer patients requiring a cumulative dose of DOX >300 mg/m2 [22], prophylactic prescription of β-blockers and angiotensin-converting enzyme inhibitors is still under debate [23]. So far, for patients whose cardiotoxicity has evolved to cardiomyopathy and heart failure, clinical management is purely palliative as AIC remains an incurable and life-threatening condition.
Regenerative cell-based approaches have been extensively investigated in preclinical studies to mitigate the deleterious effects of ANTs on myocardial tissue. Mesenchymal stromal/stem cells (MSC) have immunomodulatory, antiapoptotic and antiscarring properties, and harbor the ability to produce cytokines and bioactive factors to mediate healing and regeneration processes [24]. Bone marrow mononuclear cells (BMMNC) include MSC and other cell types, such as hematopoietic and nonhematopoietic stem cells, and have the advantage of minimal manual processing before transplantation [25,26]. The regenerative capabilities of MSC and BMMNC in CVD have been extensively explored in both preclinical and clinical studies for heart failure [27 –29] and ischemic cardiomyopathy [30,31]. The exact mechanism by which stem cells accelerate functional recovery of injury sites and, ultimately, improve cardiac function, remains unclear. However, it is likely that MSC-mediated paracrine effects rather than stem cell differentiation into cardiomyocytes are responsible for tissue and organ recovery [32].
Recently, Bolli et al. published the protocol for the SENECA trial (StEm cell iNjECtion in cAncer survivors, NCT02509156), the first phase I/II, randomized study to access the safety and feasibility of transendocardial MSC injection to treat AIC [33]. The rational for this study is thoroughly supported by previous reports of MSC therapy for myocardial repair in ischemic and nonischemic dilated ischemic cardiomyopathy. Nevertheless, because of the promising potential of this approach derives from evidence from cardiomyopathies with etiologies other than myocardial toxicity, the results from specific AIC preclinical studies are essential for the design optimization of future clinical trials. Thus, to summarize published data and add a higher level of evidence to the literature, we conducted a systematic review and meta-analysis of preclinical studies of AIC models and the effects of MSC or BMMNC therapy on cardiac function.
Methods
Retrieving the literature
This study is registered under the protocol number 5457/17 at Institute of Cardiology/University Foundation of Cardiology, RS, Brazil. This protocol was formulated using the Systematic Review Center for Laboratory Animal Experimentation format [34], and this review agrees with PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.
Types of studies and search strategy
Between August and September of 2019, we conducted an extensive search in Public Medline (PubMed), SCOPUS, and Web of Science for published preclinical/experimental studies with the use of MSC or BMMNC in AIC. The electronic search was comprehensive with terms or correlational terms and used “mesenchymal stem cells,” “mononuclear cells,” and “anthracyclines” as the investigation strategy. The detailed search strategy (keywords for searches in the Medline, SCOPUS, and Web of Science database) is available in Additional File 1.
Eligibility criteria
We included publications from inception to November 2019, without publication date or status limitation. Only studies published in English were included. Animal species were rodents and rabbits, regardless of age and sex and that were submitted to a protocol based on ANT administration to induce cardiotoxicity.
Studies with selected or purified MSC/BMMNC subpopulations and/or differentiated/engineered MSC, inducible pluripotent stem cells, embryonic stem cells, or with transplanted cells in combination with other systemic treatments (eg, carvedilol, platelet-rich plasma) were excluded. Publications reporting only data of cotreatments were excluded. However, these publications were kept for analysis if the experimental design included groups of AIC who received only MSC or BMMNC and vehicle. Studies with labeled MSC (eg, green fluorescent protein, bromodeoxyuridine) were included.
MSC/BMMNC transplantation was the selected intervention, independent of the cell source (bone marrow, adipose tissue, and umbilical cord), whether from animal or human or the chosen administration route (intramyocardial [IM], intravenous, or intramuscular). The outcome of interest was cardiac function, which should have been assessed in vivo and reported as LVEF, %, and/or left ventricular fractional shortening (FS, %).
Study selection
Publications returned from the searches were exported to a single reference manager file (EndNote software). The search and the study selection were performed by two independent reviewers (G.M.L. and P.B.G.). The reviewers deleted duplicated references and screened titles and abstract for assessment of broad inclusion criteria. If there were discrepancies in included titles, consensus was reached through discussion with a third investigator (N.M.L.).
Data extraction
Studies meeting the inclusion criteria had their data extracted to a standard data table with the following information: last name of the first author and year of publication, animal and lineage model, sex, age and/or weight, pharmacological scheme for ANT cardiac toxicity induction, cumulative dose of ANT (mg/kg), ANT route of administration, cell type and source, cell dosage (total number of administered cells), frequency of cell therapy administration, route of administration/delivery of cells, timing of cell transplantation according to the establishment of the experimental model, and timing of cardiac function assessment.
The number of animals, LVEF and/or FS mean and standard deviation (SD) of control (ANT only or ANT + vehicle or sham), and intervention (ANT + cell therapy) groups were extracted from every included study. If LVEF/FS was reported as mean and standard error of the mean or if only graphical representations of mean were presented, we calculated SD and extracted valued data using GetData Graph Digitizer software [35,36]. If the full text was not available online or if essential data for the analysis were not clearly reported in the original article, supplementary material, or references, we contacted the corresponding authors by e-mail. Studies of authors who did not answer or refused to send the required information were excluded from the analysis.
To investigate to what extent some variables could interfere with the main outcome, we performed the following prespecified subgroup analyses: animal species (rodent or rabbit), model of cardiomyopathy (ANT cumulative dose), type and source of cells, cumulative number of transplanted cells, and the route by which cells were delivered.
Methodological quality of the studies and assessment of risk of bias
The methodological quality of the studies included in the meta-analysis was assessed by three methodological checklists. The first methodological checklist was the recommended Cochrane Collaboration criteria based on the following parameters: random sequence generation, concealment allocation, blindness of evaluators, intention-to-treat analysis, and description of losses and exclusions [37]. We also used Systematic Review Center for Laboratory Animal Experimentation's (SYRCLE) risk of bias tool, adjusted for animal studies from the Cochrane tool of risk of bias [38]. For both of these tools, the possible answers for each question were: Y (yes, low risk of bias), N (no, high risk of bias) and U (unclear, without specification details to measure the risk).
The second methodological checklist was adapted from Collaborative Approach to Meta-Analysis and Review of Animal Data from Experimental Studies (CAMARADES) with minor modifications [35]. The items in this checklist was as follows: (1) peer-reviewed publication, (2) presence of randomization, (3) assessment of dose–response relationship, (4) blinded assessment of outcome, (5) monitoring of physiological parameters, (6) sample size calculation, (7) statement of compliance with regulatory requirements, (8) use of analgesic, (9) statement of potential conflicts of interest, and (10) use of accurate/suitable/adequate animal models.
Statistical analyses
The analyses were conducted in Review Manager Software, version 5.3, and Comprehensive Meta-Analysis Software, version 3 (Biostat, NJ, USA). The main outcomes of interest were LVEF and FS (both reported as %) at follow-up between control and treated animals. We calculated mean differences (MD) with the 95% confidence interval (CI). We reported the P value for the comparison among groups, and P ≤ 0.05 indicated statistical significance. We used random effects models for pooled-effect estimates due to significant heterogeneity between models of AIC and MSC or BMMNC transplantation protocols. Next, we conducted subgroup analyses. Between-study heterogeneity was explored by the chi-squared test (P ≤ 0.1) and quantified with the inconsistency measure (I 2). Heterogeneity was considered significant at P < 0.10. I 2 values <25%, 50%, and over 50% indicate low, moderate, and high heterogeneity, respectively [39].
To identify outliers and the possible independent predictors of MSC therapy success regarding cardiac function, sensitivity analyses were performed for animal model (species, sex, and cumulative dose of ANT), cell therapy (cell type, route of delivery, number of injected cells, timing of cell therapy in relation to end of ANT protocol), and timing of outcome assessment (in relation to AIC establishment and cell therapy). Next, to identify the sources of heterogeneity, we first omitted the outliers studies from overall meta-analyses, and then one study at a time. Finally, publication bias was calculated using Egger's regression test. A power analysis for future studies in ANT-induced cardiomyopathy (AIC) was also performed.
Results
Study selection process
Figure 1 depicts the flow chart of the study selection process. We identified 4,730 records after searching on the PubMed, EMBASE, Scopus, and Web of Sciences databases, and 4,114 publications remained after the exclusion of duplicated references. We screened 4,114 records, and, after title and abstract screening, we excluded 4,037 for irrelevant content (randomized controlled trials, systematic reviews/meta-analysis/overviews or reviews, human observational studies, and in vitro studies). The 77 remaining studies were reviewed for full-text reading and, among these, 55 studies were excluded due to absence of LVEF or FS as an outcome of cardiac function, absence of a cell group without combined treatment, other cell types and cell products, and languages other than English. Finally, we included 22 studies for meta-analysis.

Flow chart of the study selection procedure.
Description of the included studies
The characteristics of the included studies are summarized in Table 1. The median publication year was 2011 (ranging from 2003 to 2019). Altogether, the studies involved 381 animals (200 rats, 55 mice, and 126 rabbits). The intervention group comprised 57% of all animals in either outcomes. Sprague-Dawley rat (31.7%), C57BL6 mouse (11.28%), and New Zealand rabbit (33%) were the most frequently chosen rodent and rabbit species, respectively. Thirteen of the studies used male animals [40 –52], whereas only three reported the use of females (33%) [53 –55], and six studies failed to report the animal sex [56 –61]. The age and/or weight of the animals at baseline were mentioned in 21 studies. The median of age and weight of rodents was 7 weeks and 195 g for rodents, and 16 weeks and 2.4 kg for rabbits, respectively.
Summary of the Main Characteristics of the Included Studies
All studies used doxorubicin, except for Chen et al. [55], which used daunorubicin.
ASC, adipose-derived mesenchymal stromal cells; BMMNC, bone marrow mononuclear cells; BMMSC, bone marrow mesenchymal stromal cells; FS, left fractional shortening; GFP, green fluorescent protein; hBMMSC, human BMMSC; hUCMSC, human umbilical cord mesenchymal stromal cells; IM, intramyocardial; IP, intraperitoneal; IV, intravenous; LVEF, left ventricular ejection fraction; U, unclear.
DOX was the ANT of choice in the vast majority of the studies, with only one study using other drug (daunorubicin) to establish AIC [55]. While DOX was administered intraperitoneally (IP) in rodents, rabbits received it intravenously (IV). The cumulative dose of ANT ranged from 10 to 24 mg/kg. The induction of cardiotoxicity protocol was highly heterogeneous in terms of frequency of ANT injections (from 48 h to 8 weeks) and the timing of cardiac function assessment following the end of the protocol (from 48 h to 20 weeks).
Most studies investigated the regenerative potential of cell therapy in AIC by treating the animals after completion of the cumulative dose of DOX/daunorubicin (median time of 3.2 weeks, ranging from 24 h to 10 weeks). Only three studies aimed to test the effects of early cell therapy in AIC experimental models [52,53,55], which means that cells were transplanted before or during ANT exposure. Five studies failed to state the time of cell transplantation. Assessment of LVEF and FS values following MSC/BMMNC transplantation by echocardiogram occurred most frequently 4 weeks after the conclusion of the ANT protocol.
Regarding the cell therapy intervention, MSC was the main type of transplanted cell (17 studies). Eight studies utilized autologous cells [41,45,48,56 –59,61], and only four used xenogeneic cells [51,53,55,60]. The cells were most frequently isolated from bone marrow (18 studies), followed by human umbilical cord (2 studies) and adipose tissue (2 studies). Eleven studies delivered the cells intramyocardially, followed by IV route (femoral, jugular, and tail) (7 studies). Finally, the cumulative number of received cells at the end of protocol varied from 0.5 × 106 to 50 × 106 cells.
Study quality and risk of bias assessment
Since poor reporting in preclinical studies is a known problem and many items of the risk of bias tool were scored as unclear, we scored three reporting items, that is, the Cochrane Collaboration criteria, SYRCLE, and CAMARADES. Figure 2 depicts the risk of bias assessment for the 22 included studies based on Cochrane Collaboration items; the risk of bias results for each study are summarized in Additional Files 2 and 3.
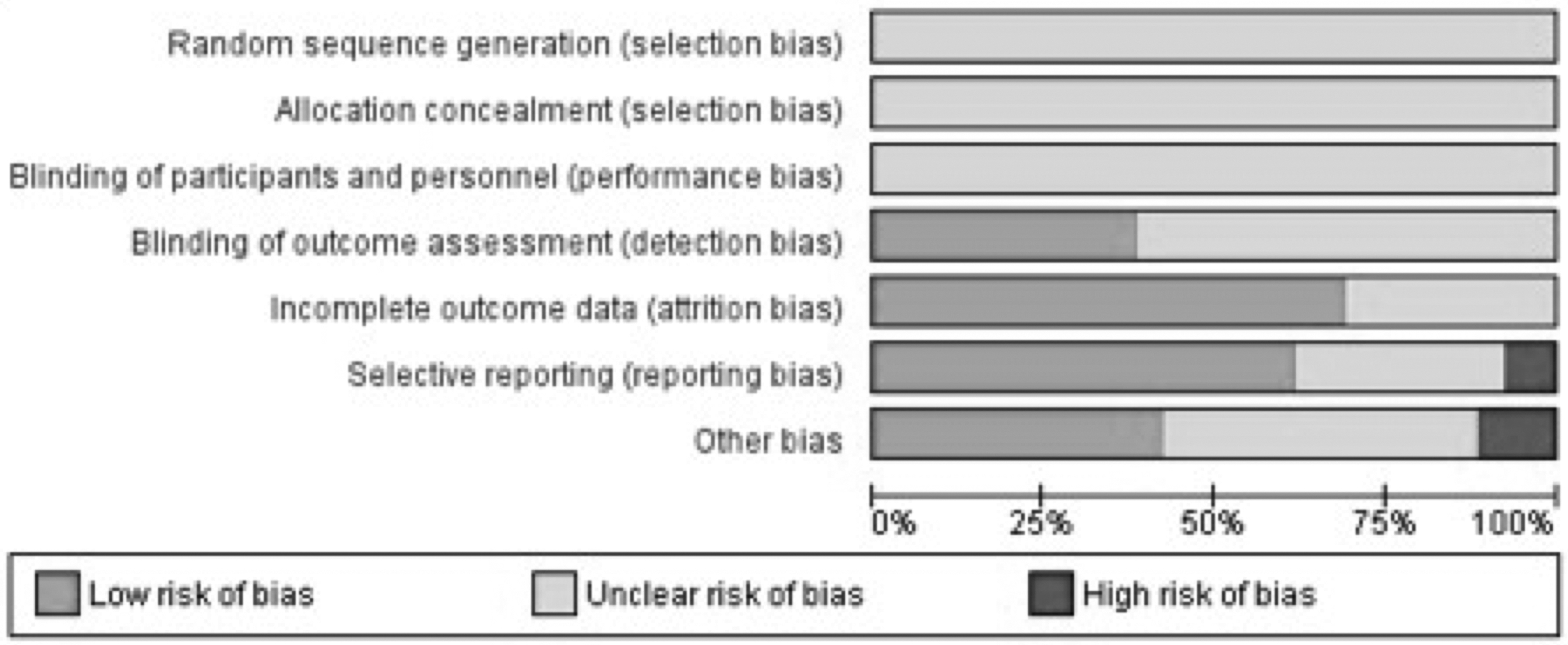
Study quality graph based on Cochrane Collaboration criteria.
The assessment of randomization risk of bias showed that none of the included studies had properly described whether or not there was a blind strategy for allocation of the animals to the experimental groups. The baseline characteristics of 21 studies were assessed as low risk and one study as unclear risk of bias. Baseline characteristics, such as initial weight and age, were described in almost all the included studies and, except for one study, no significant differences between experimental and control groups were observed. Blinding of caregivers and researchers were not mentioned in any of the studies. Eight studies provided information concerning blinding the professional who performed the echocardiography assessments, and only one study mentioned the randomization for outcome assessment. Fifteen studies presented a low risk of incomplete outcome data, while seven studies presented an unclear risk of bias. Selective outcome reporting was assessed as low risk in 13 studies, high risk in two studies and unclear risk of bias in seven studies. Nine studies presented a low risk of other sources of bias, three studies presented a high risk, and for 10 studies this risk was unclear
Compliance with specified CAMARADES items is shown in Additional File 3. Only four studies received seven points, which was the maximum score in the included reports; six studies received six points, eight studies received five points, two studies received four points, and two studies received three points.
Meta-analysis of cardiac function
Pooling the individual effect sizes of both cell therapies (MSC/BMMNC), the meta-analysis showed that this intervention enhances LVEF (MD = 9.87%, 95% CI 7.25–12.50, P < 0.00001) and FS (MD = 7.80%, 95% CI 5.68–9.92, P < 0.00001) of ANT-treated animals. Conversely, as the overall heterogeneity between the studies was considered high (I2 = 91% for LVEF and I2 = 93% for FS), we anticipated the existence of an influence of the AIC model (with regard to ANT cumulative dose), the cell therapy protocol (cell type, total number of injected cells, and route and timing of administration), and the study design (timing of final cardiac function assessment) (Fig. 3).
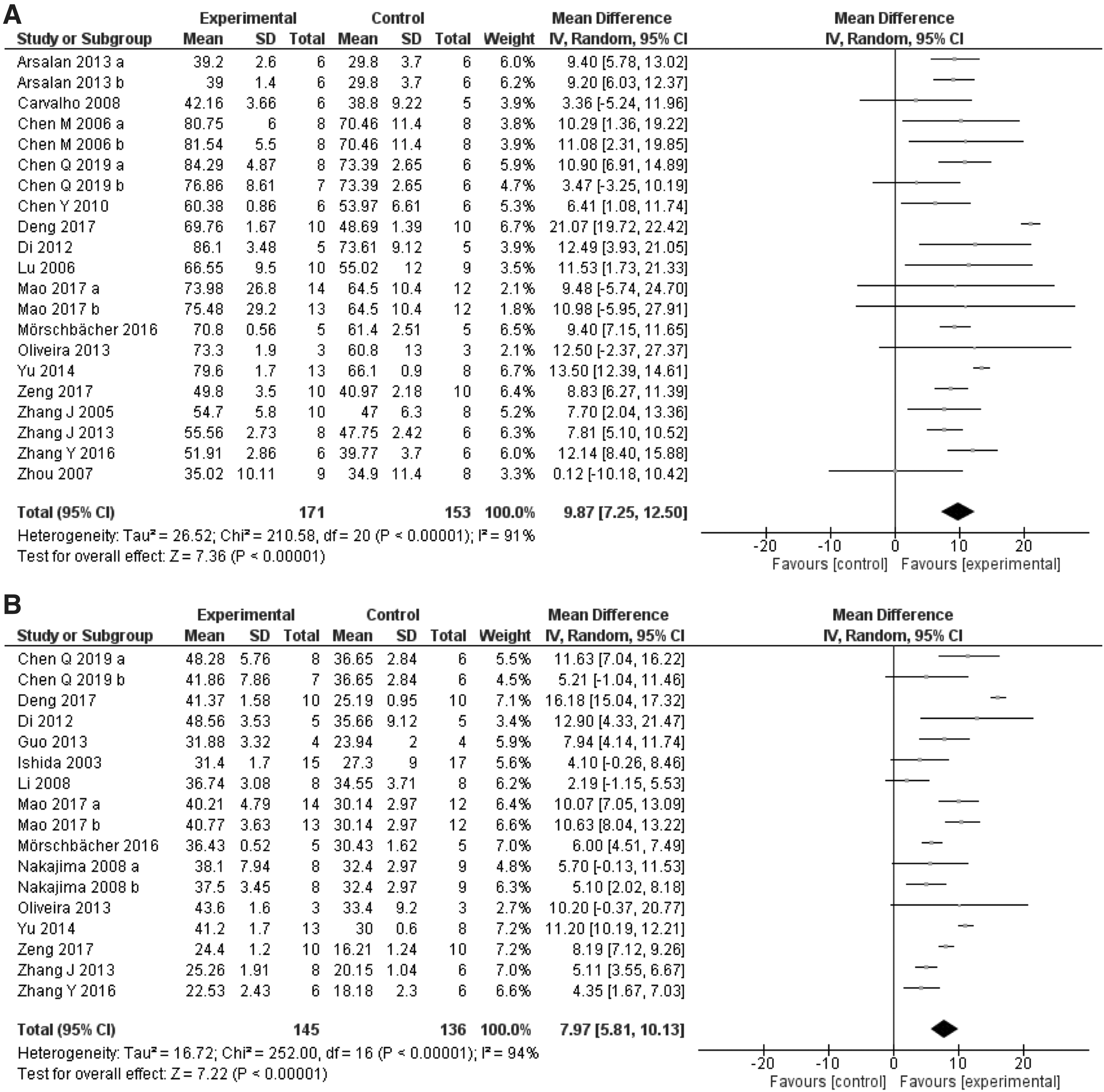
Effects of cell therapy on cardiac function of experimental models of AIC.
Next, we conducted a sensitivity analysis to identify the existence of independent predictors of LVEF improvement (Fig. 4). First, we retrieved ΔLVEF (%) between experimental and control groups within subgroups of interest and then investigated the outliers studies (Additional File 4). After omitting the outliers studies on each subgroup analysis, high cumulative cell dosage (>107 cells, P = 0.064), delivery of cell therapy by intravenous route (P = 0.083), and cell therapy before or during ANT exposure (P = 0.0781) were identified as possible predictors of better outcomes of cell therapy for AIC.

Sensitivity analysis of changes in LVEF based on clinical predictors of cell therapy success after removal of outliers studies. Line on boxplots shows mean difference of LVEF (%) between controls ANT-treated animals, and those who received cell therapy.
Finally, we omitted the outliers studies and the other included studies (one at a time) from the overall meta-analysis and from each subgroup analyses (Additional File 5). Considering overall data for LVEF and LVFS, there was no significant changes in heterogeneity or in the previously demonstrated cardioprotective effect of cell therapy, which denotes that no specific study was biasing the results.
Effect of animal model features
To investigate if cardiac function of AIC animals treated with cell therapy could have been by the main features of the AIC animal model, we conducted subgroup analyses for species, sex, and cumulative dose of ANT (Fig. 5). Improvement of LVEF following cell therapy occurred irrespective of animal species (χ 2 = 0.91, P = 0.34, I 2 = 0%) (Fig. 5A), sex (χ 2 = 0.47, P = 0.49, I2 = 0%) (Fig. 5B), and ANT cumulative dose (χ 2 = 0.00, P = 0.98, I 2 = 0%) (Fig. 5C).
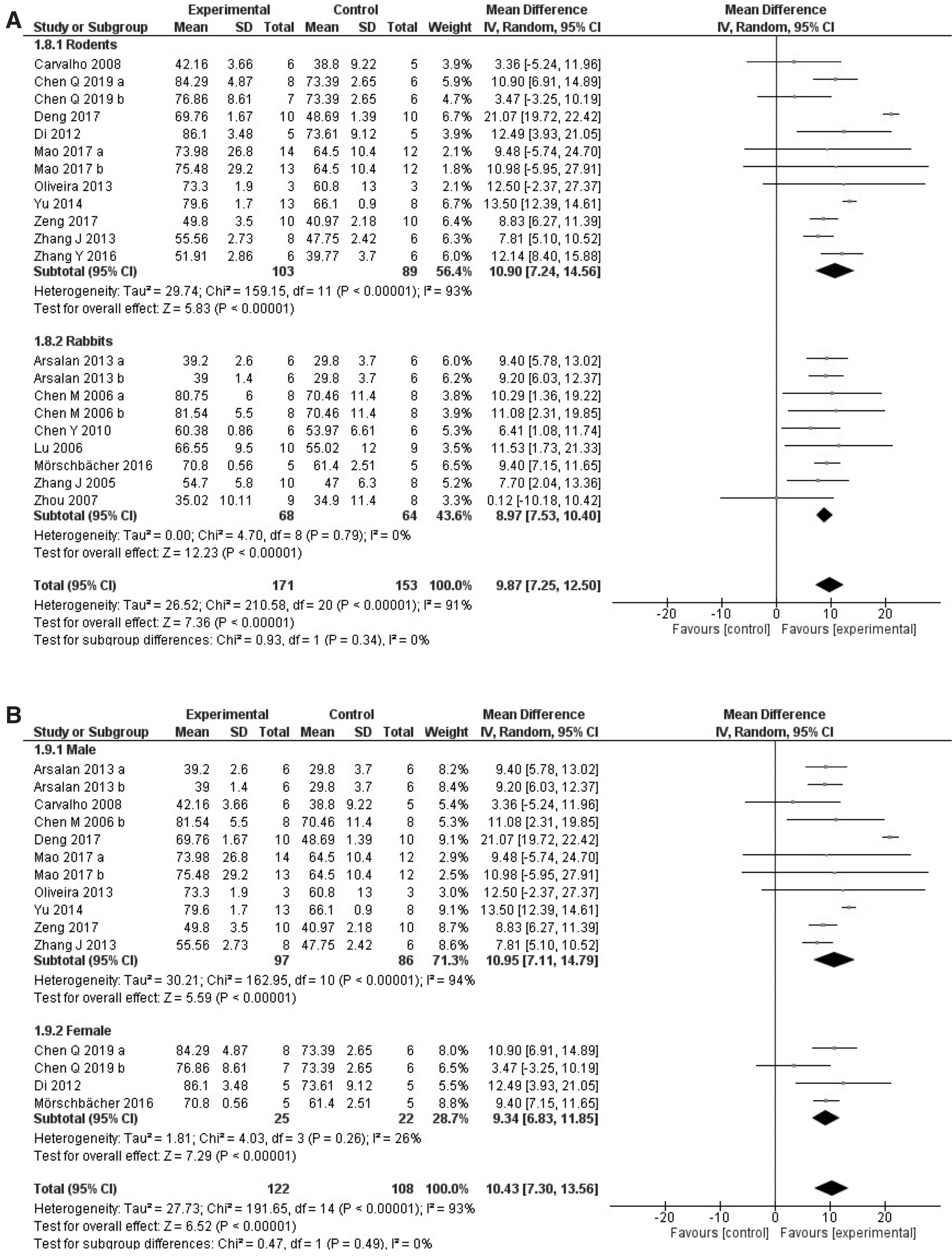
Subgroup analyses of the effect of features of animal model on LVEF of animals with AIC.

Effect of cell therapy conditions
Next, we performed three subgroup analyses with regard to the conditions of cell therapy: cell type (MSC or BMMNC), cumulative number of cells, and route of administration (Fig. 6). MSC-based therapy improved LVEF similarly to BMMNC (χ 2 = 0.29, P = 0.59, I 2 = 0%) (Fig. 6A). Since two studies used adipose-derived MSC and three used hUCBMSC, it was not possible to compare these groups separately as planned.
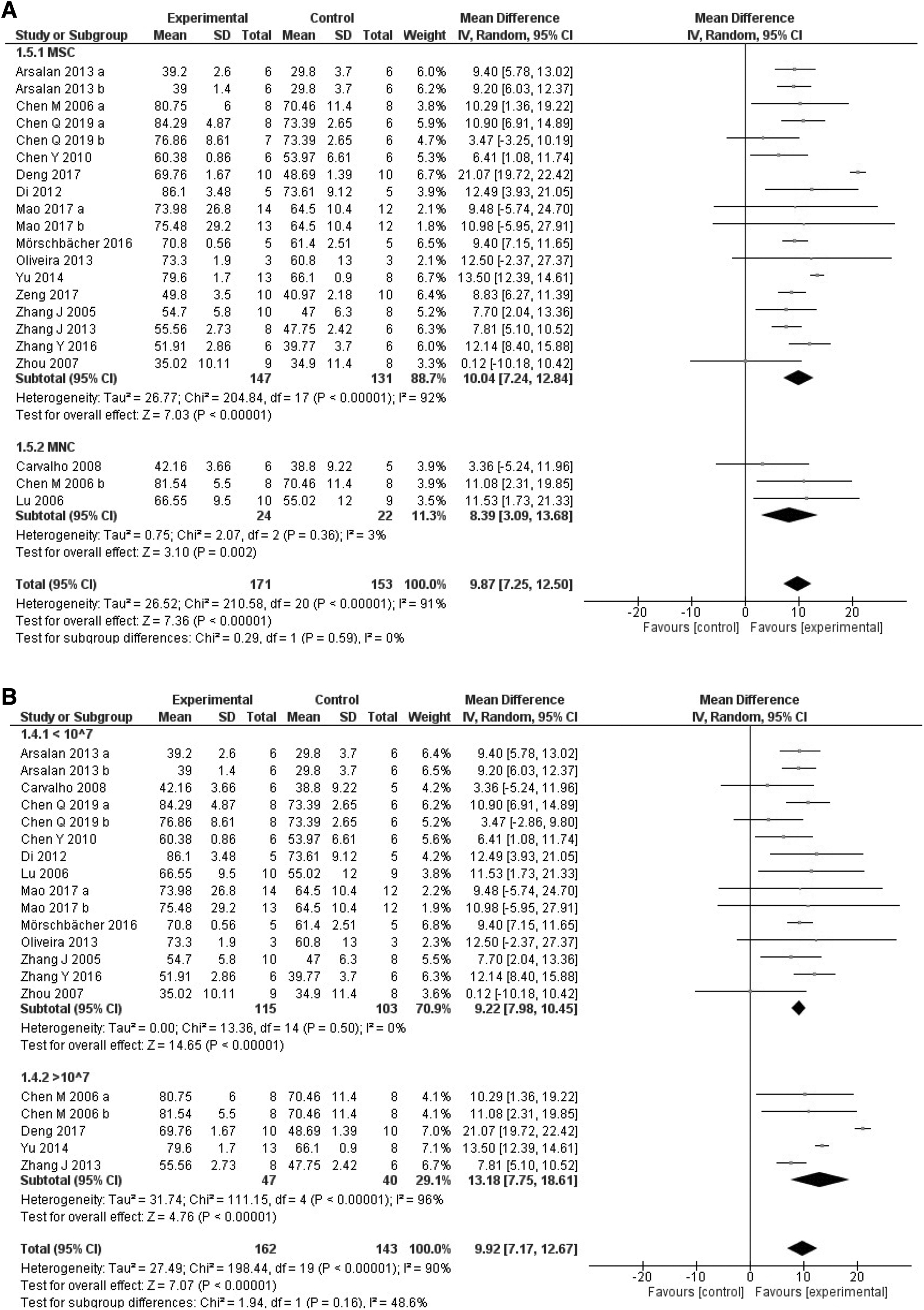
Subgroup analyses of the effects of cell therapy conditions on LVEF of animals with AIC.
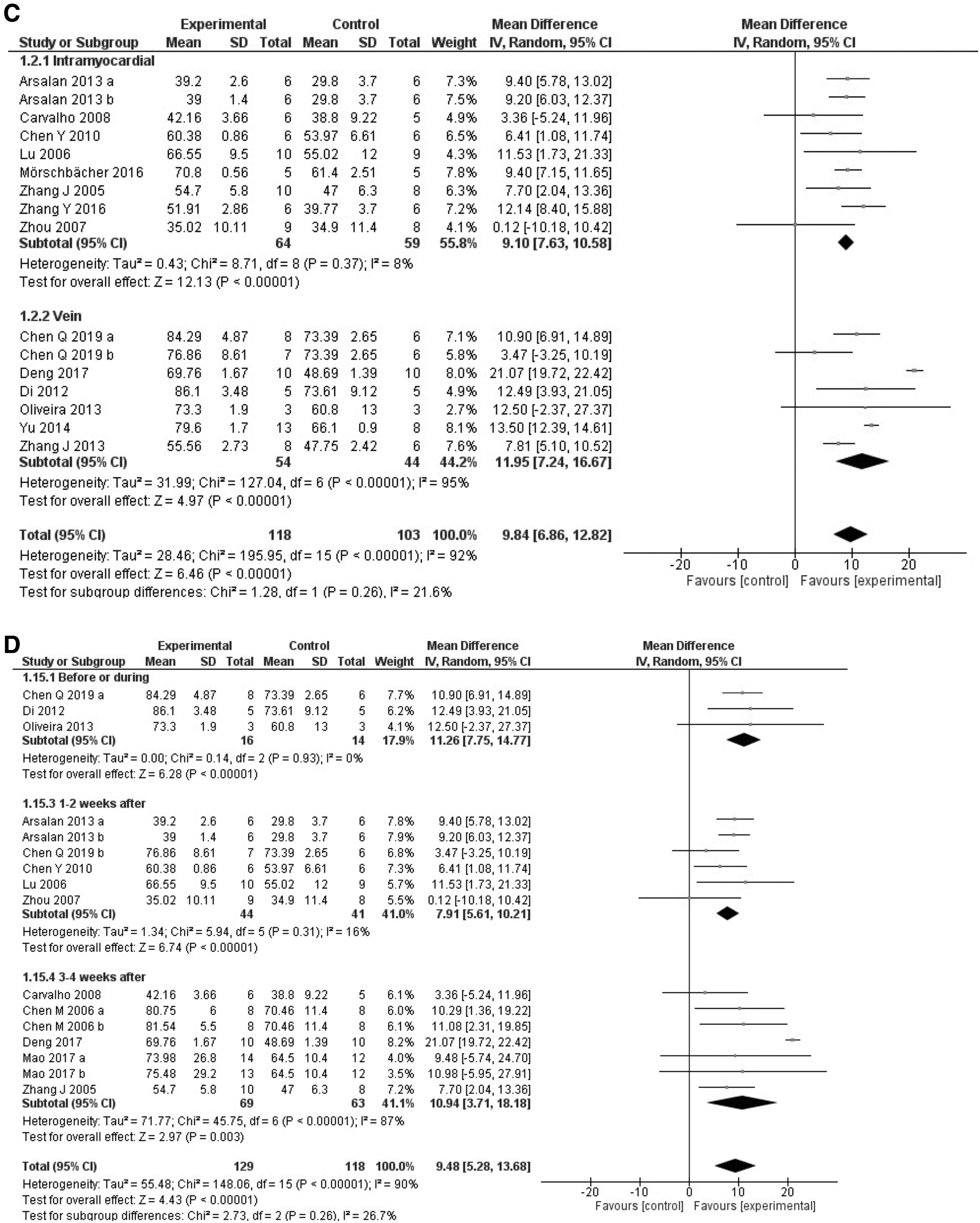
Unexpectedly, LVEF improvement occurred independently on the cumulative dose of injected cells (χ
2 = 1.94, P = 0.16, I
2 = 48.6%) (Fig. 6B
Although difference between subgroups remained not significant for the cumulative number of cells after omitting outliers [49,61], heterogeneity changed from 48.6% to 0% after Deng et al. [49] was omitted from this analysis. The same occurred for subgroup analysis of cell therapy route: omitting Deng et al. [49] eliminated heterogeneity, which was 21.6% when all studies were included. Also, sensitivity analysis of timing of cell therapy did not modify the results obtained in the subgroup analysis.
Effect of the timing of cardiac function assessment
Finally, we performed a subgroup analyses to investigate the effects of timing on the cardiac function assessment for LVEF (Fig. 7). This analysis refers to two time points: the timing when final cardiac function was assessed in relation to (1) the achievement of the cumulative dose of ANT (Fig. 7A) and (2) the timing of cell therapy administration (Fig. 7B). Although we did not identify the influence of the time of the cardiac outcome final assessment on the cell therapy-mediated effects on LVEF in animals with AIC regarding the cumulative dose of ANT (χ 2 = 0.27, P = 0.88, I 2 = 0%), after omitting the outlier study Zhang et al. [44], subgroup analysis revealed that (χ 2 = 8.27, P < 0.01, I 2 = 75.8%) the later the cardiac function assessment (>8 weeks) is performed after AIC induction, the better is the effect of the intervention (MD of LVEF: 13.41%) (Additional File 5). The timing of cardiac function assessment in relation to cell therapy did not present influence on LVEF (χ 2 = 0.04, P = 0.85, I 2 = 0%).
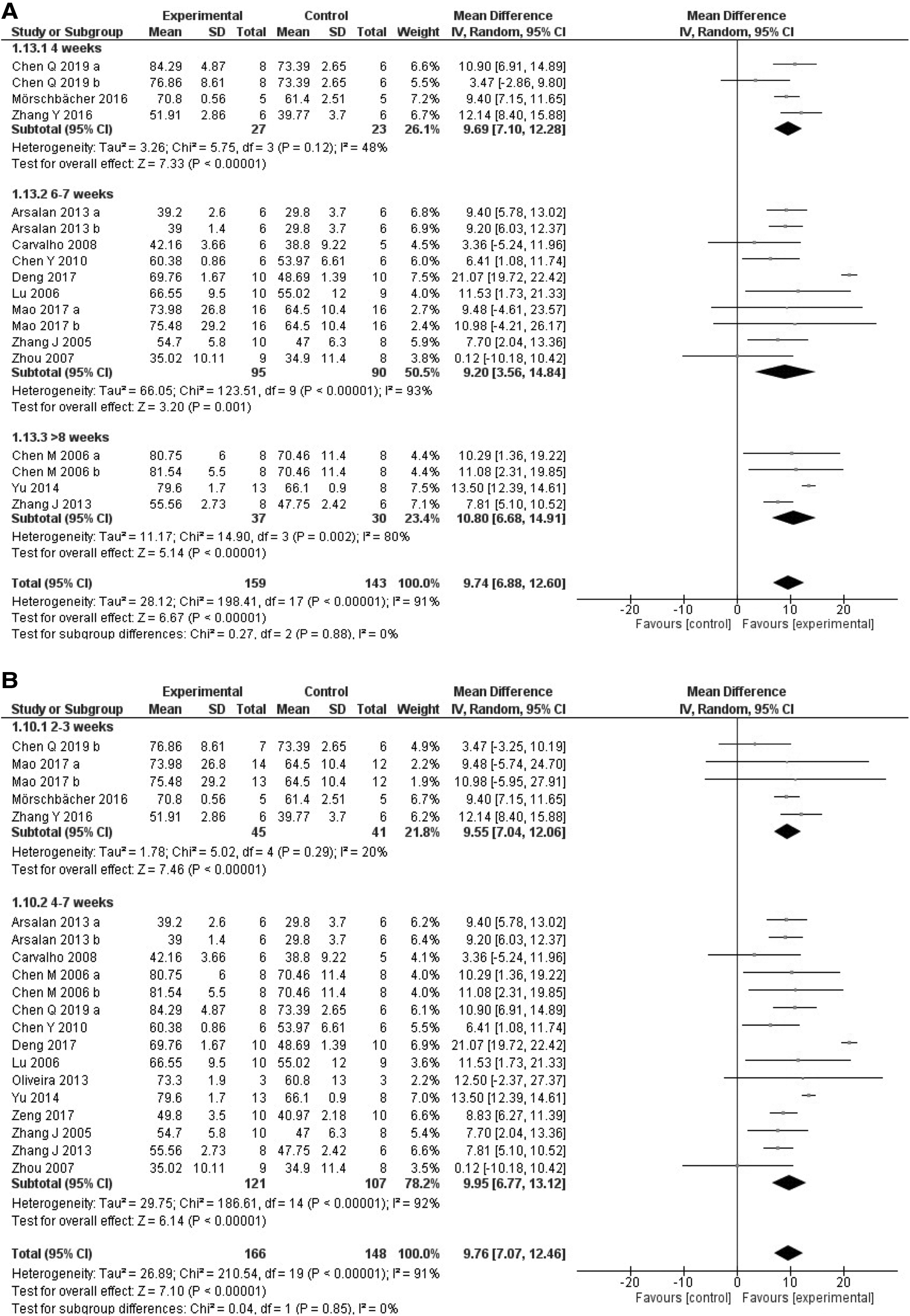
Subgroup analyses of the influence of the moment of cardiac outcome assessment.
Publication bias
Analysis of publication bias was found to be influenced by the presence of small study effects. Asymmetric funnel plots indicated the presence of publication bias for LVEF and FS (Egger's test, P < 0.01, and P < 0.0001, respectively) (Fig. 8).
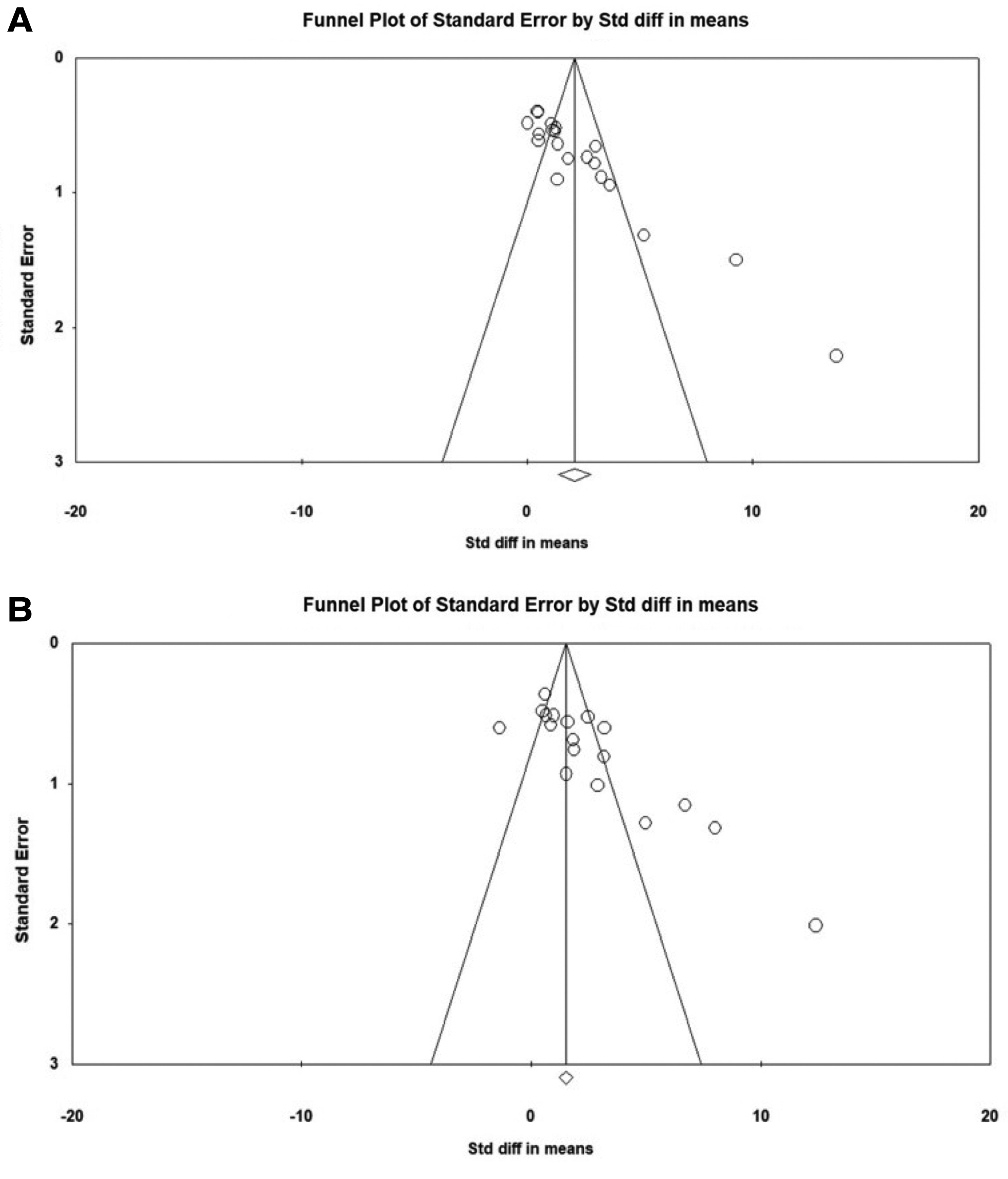
Publication bias.
Power calculation
Based on the overall results, we performed a sample size calculation for future studies in cell therapy for AIC. To obtain a power of at least 90% in a two-sided two-sample t-test with an alpha of 0.05, 9 rodents or 13 rabbits are needed to be included on each experimental group, to detect a significant difference of 9.67% in LVEF, and 3 rodents or 16 rabbits to detect a minimal difference of 7.80% in FS between groups. Also, we estimated the sample size considering the possible main predictors of MSC therapy success and based on the MD obtained in each prespecified subgroup analyses (Additional File 6).
Discussion
After a comprehensive search and data assimilation from 22 studies of MSC/BMMNC therapy on AIC animal models, pooled analysis showed cell therapy results in a difference of 9.87% for LVEF and of 7.80% for FS of ANT-treated animals. The main findings were: (1) cell therapy improves cardiac function of animals with AIC; (2) sensitivity analysis suggests a superior effect of higher cell dosage (≥107), delivery by intravenous route and moment of intervention (before/during ANT treatment); (3) subgroup analyses, however, did not confirm the superiority of these factors concerning the available evidence.
Effects of animal model features
Many animals exposed to ANTs experience lesions morphologically comparable to those occurring in patients taking these drugs [62]. Although LVEF of rodents and rabbits with AIC and treated with cell therapy were similar, studies of AIC with rabbits are less heterogeneous.
The influence of sex is extensive in CVDs [63]. Clinical evidence has shown that prepubertal and menopausal female cancer patients are at increased risk of AIC in comparison to males of the same age, which demonstrates the relevance of sex-related differences in this context [64]. However, this meta-analysis included only three studies with female animals, and none of these mentioned handling the estrous cycle stage or discussed the choice of sex.
The ANT administration route, schedule, and cumulative dose are sensitive features of an AIC animal model, with a high risk of biasing the results. While in humans ANT are administered intravenously, only studies with rabbits and one of the studies with rats [55] chose IV route to administer these drugs. Regarding dosing regimen and cumulative dose, a bolus injection of a high ANT dose is associated with higher mortality rates from noncardiovascular causes in rodents, and the administration of the same cumulative dose over days or weeks results in better survival rates and induces more classic features of DOX-induced cardiomyopathy [65].
The mean adult cancer patient surface body area is around 1.72 m2 (mean weight = 66.3 kg) [66], and the majority of patients undergoing DOX treatment will not exceed a maximum lifetime cumulative dose of 550 mg/m2 or 14.26 mg/kg [67]. Although five studies used cumulative dose between 18 and 24 mg/kg, the effects of cell therapy on cardiac function were the same in comparison to those which used lower doses.
Conditions of cell therapy
The encouraging effect of cell therapy in cardiac function of animal models of AIC was obtained regardless of cell type, the cumulative number of injected cells, or the route of cell therapy delivery. However, it is of great importance to highlight that, despite the absence of differences between subgroups, the heterogeneity and inconsistency of results were extremely low in studies that used BMMNC, a lower number of cells, and the IM route.
While previous reports suggested that MSC harbor the greatest potential in regenerative medicine [68], a meta-analysis of clinical trials with BMMNC transplantation for ST-segment elevation myocardial infarction and nonischemic dilated cardiomyopathy showed improvements in functional parameters [69,70]. Contrary to our results, a meta-analysis of preclinical models of ischemic cardiomyopathy identified the independent influence of cell type on global ventricular function [71]. Importantly, it must be considered that, as for LVEF, only three studies with BMMNC could be included in the pooled analysis [41,45,58].
Clinical evidence of cell therapy in ischemic cardiomyopathies suggests that the transplantation of a greater number of cells (≥107) appears to have a more pronounced impact on LVEF [30,72] and ventricular remodeling [73]. Considering only the studies that provided mean body weight, the mean number of transplanted cells per kilogram was 1.17 × 107. However, for humans, intravenous cell therapy must never exceed 12 million cells/kg [74], and most preclinical studies use a near fivefold higher dosage. Consequently, it is extremely challenging to compare the magnitude of the results between species and to translate experimental protocols into clinical practice, as preclinical results might be overestimated.
Although it is well documented that MSC and BMMNC harbor the ability to sense released factors from remotely damaged tissues and migrate to injury sites [32,75], we did not identify the influence on the route of cell therapy delivery (IM vs. IV) on the main outcome. For this analysis, we excluded four studies that administered the cells by other routes [41,43,51,56]. A meta-analysis showed that IM or intracoronary MSC delivery has superior effects on LVEF in comparison to IV administration in acute myocardial infarction and ischemic heart failure [76]. However, direct injection of cells into cardiac tissue requires invasive surgery [77], and could disrupt electrical conduction due to the formation of immature gap junctions with cardiomyocytes [41,56]. Furthermore, a limited number of cells reach the site of injury following IV administration because of cell trapping by other organs [78]. This is particularly relevant within the context of general ANT toxicity [3], where systemic delivery of cell therapy might result in the migration of these cells to other injured organs rather than specifically to the heart, and improve the general condition. However, the expected effect on cardiac function might be suboptimal.
Finally, it was not possible to compare different sources of cell therapy, as the vast majority of the studies utilized BM as source and only four studies utilized adipose-derived MSC and hUCMSC. Even though BM-derived cells are the most utilized in clinical randomized studies [79], a recent study showed that Wharton's jelly MSC have a stronger immunomodulatory effect and proregenerative features than BMMSC [80]. Also, hUCBMSC therapy has been seen to exert beneficial effects in ameliorating cardiotoxic manifestations in preclinical studies of AIC [81,82].
Timing of cardiac outcome assessment
The moment when cardiac function is assessed to define the establishment of AIC may implicate in different models of disease presentation (acute/chronic; early/late onset) [83], it is crucial to clinical translation that preclinical studies consider the timing of cardiac function assessment a crucial variable. Our meta-analysis identified the influence of the timing of the final cardiac function assessment after AIC induction (>8 weeks) only after omitting an outlier study. It was recently proposed that the assessment of cardiac function and intervention 1 and 6 weeks after the ANT protocol represents acute and chronic AIC, respectively. In humans, cardiotoxicity is classified as acute if the clinical manifestation occurs within 2 weeks from the end of treatment, and chronic if it develops within 1 year [5]. Most of the included studies reported final cardiac function more than 8 weeks after the establishment of the AIC model, so we can infer that these studies were, in fact, evaluating the chronic presentation of cardiotoxicity. Furthermore, some clinical studies have reported that beneficial effects of cell therapy for CVD are temporary and diminish by 1 year after intervention [84,85]. Thus, while short periods of observation may overestimate the magnitude of cardiac regeneration, prolonged observation periods could add valuable information of more permanent effects in experimental studies.
Possible mechanisms implicated in cell therapy-mediated effects in AIC animal models
Despite suggestions in the discussion sections of some of the included studies [43,44,49,57] that LVEF/FS improvement could have been achieved following MSC or BMMNC differentiation into cardiac and vascular cells, this was not proven by molecular or cellular evidence. In fact, it is likely to occur due to the paracrine effects [42,48,51,52,56,60], including the stimulation of angiogenesis [40,48], the release of antioxidant factors [53], a decrease in immune cell infiltration [55], a reduction in cardiomyocyte apoptosis [61], an increase of factors involved in tissue repair [51], or renin angiotensin-system modulation [42]. Moreover, MSCs have been implicated in an enhanced response to oxidative stress and the restoration of mitochondrial function in cardiomyocytes, which is particularly relevant in the context of DOX-induced cardiotoxicity mechanisms [86,87].
Recommendations for future translational cell therapy research on AIC
Preclinical studies must be designed and conducted similarly to randomized clinical trials to ensure the highest translational potential to the clinical scenario. Besides the heterogeneity of the AIC model, the wide ranges of cell dosages used, regardless of the route of administration or considering an adjustment by weight do not allow for a proper comparison of dose-dependent effects between studies. In addition, because most of the studies suggest that the improvement in cardiac function was exerted by paracrine effects, it is not possible to infer that the potency of released mediators was proportional to the number of administered cells. Thus, future preclinical studies must take into account the weight-adjusted dosage of cells to predict human responses in a more accurate way.
Also, our search retrieved only one study with tumor-bearing animals. Considering the prescription of the cell therapy concomitantly to cancer treatment, and the ability of these cells to modulate essential factors for tumor survival, the migration of MSC/BMMNC into tumor sites may act as a double-edged sword. Current state-of-the-art of the effects of MSC/BMMNC therapy on tumor progression is still controversial [88]. Therefore, further studies are demanded to clarify the long-term outcomes and influence of preventive cell therapy for AIC on oncological outcomes of tumor-bearing patients.
Finally, as half of the included studies had missing information on sex, age, number of administered cells, the timing of the cardiac outcome assessment, and cell therapy regimens, the quality of reports must be improved.
Limitations
A major limitation of this and other meta-analysis of preclinical models lies in the fact that negative results of preclinical studies are underreported, which may act as a major source of bias. Also, the studies present high heterogeneity, inconsistency, and poor quality of protocols and results reporting. The cardiac function outcomes (LVEF and FS) are extremely sensitive and may account for the heterogeneity, as the acquisition of these parameters by echocardiography are subjected to inter- and intraobserver variability [89]. Moreover, although echocardiography is the method of choice for noninvasive left ventricular function assessment in small animals, a systematic critical evaluation of imaging quality and the resulting data is often lacking [90].
Conclusion
Despite the advances on the comprehension of the mechanisms of antineoplastic-induced cardiac toxicity and the growing investigations into pharmacological approaches, there is no consensus regarding the best strategy to prevent or treat cardiotoxicity. This meta-analysis showed that cell therapy for AIC is safe and improves LVEF and FS in small animals. However, these results must be taken with caution, as heterogeneity and poor report quality and distance from the clinical landscape may have overestimated the magnitude of cell therapy benefits on cardiac function in AIC preclinical models. Future experimental studies must include several features to diminish sources of bias, that is, to include tumor-bearing animals and antineoplastic agent combinations, to design feasible cell therapy schemes in clinical practice and to evaluate long-term outcomes.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was financed by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brazil (CAPES)—Finance Code 001 and by Fundo de Apoio do IC-FUC à Ciência e Cultura—Institute of Cardiology of Rio Grande do Sul/University Foundation of Cardiology—Rio Grande do Sul, Brazil (FAPICC).
Supplementary Material
Additional File 1
Additional File 2
Additional File 3
Additional File 4
Additional File 5
Additional File 6
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.