
Abstract
The global COVID-19 pandemic has prompted urgent need for potential therapies for severe respiratory consequences resulting from coronavirus infection. New therapeutic agents that will attenuate ongoing inflammation and at the same time promote regeneration of injured lung epithelial cells are urgently needed. Cell-based therapies, primarily involving mesenchymal stromal cells (MSCs) and their derivatives, are currently investigated worldwide for SARS-CoV-2–induced lung diseases. A significant number of academic centers and companies globally have already initiated such trials. However, at a time of unprecedented need, it is also foreseen that families and caregivers will seek all available options, including access to cell-based and other investigational products, even before proven safety and efficacy as well as regulatory approval. This should not be an excuse for opportunists to sell or advertise unproven therapies of any kind. “Compassionate use” should be conducted in the context of a clinical investigation framed by strict ethical and regulatory permissions, with the goal of obtaining mechanistic information wherever possible.
The serious consequences of the COVID-19 pandemic have prompted a global initiative to develop effective therapies that can lessen disease severity in infected patients, particularly those with severe respiratory disease. Cell-based approaches, primarily using mesenchymal stromal cells (MSCs), have demonstrated an acceptable safety profile in patients with non-SARS-CoV-2–related acute respiratory distress syndrome (ARDS) in the limited currently available information [1]. However, whether these therapies are effective for treating respiratory virus-induced ARDS, including that resulting from SARS-CoV-2, is unknown [1]. This is despite several recent case reports and uncontrolled case series suggesting potential efficacy [2,3]. Regardless, there are an increasing number of both academic and industry-sponsored trials of cell-based therapies for COVID-19 patients initiated over the past several months. Most are investigating use of MSCs, but some are investigating MSC-derived products including extracellular vesicles (EVs) and some are utilizing other cell types. In parallel, there has been a worrisome increase in the number of businesses offering unproven and untested cell-based therapy approaches in uncontrolled and unregulated settings [4]. This creates a potentially dangerous situation for patients, families, and caregivers in often desperate situations.
An overview of the rationale, preclinical data, and clinical experience of cell-based therapy in non-COVID–related ARDS provides a strong platform underlying legitimate investigations. There is a wealth of preclinical data in both small and large animal models as well as in explanted human lungs in which either systemic or direct airway administration of MSCs mitigates experimentally induced acute lung injuries resulting from bacteria or bacterial product, for example gram-negative bacterial endotoxin, administration [5,6]. The postulated mechanisms largely focus on paracrine actions of the administered MSCs, including release of anti-inflammatory cytokines, antibacterial peptides, and EVs that mitigate inflammation in the setting of acute lung injuries (Fig. 1) [7]. These encouraging results have provided a basis for the growing number of academic and industry-sponsored investigations of systemically administered MSCs in (non-COVID) ARDS patients [1]. While these studies have uniformly demonstrated a good safety profile, there remains uncertainty about potential efficacy. One major academic-based trial did not demonstrate clinical efficacy [8], whereas improvement in clinically relevant endpoints, including increased ventilator-free and ICU-free days and decreased 1 month mortality, was suggested in one major industry trial [9]. However, neither of these trials have specifically targeted patients with respiratory virus-induced ARDS. Further, there are only a small number of preclinical studies in models of respiratory virus infection, and these all involve influenza rather than coronavirus. Notably, there were contrasting results of efficacy in these studies, possibly related to the type of influenza (swine vs. avian) infection utilized. This further adds to uncertainty about whether MSC or other cell or cell product administration will have specific efficacy in SARS-CoV-2–induced respiratory failure. There are almost no available clinical data with respect to MSC administration in other types of respiratory virus infections with only a case report in a patient with H1N1 flu-related ARDS (allogeneic bone-marrow-derived MSCs) [10] and a case series after H7N9 flu infection (allogeneic menstrual blood-derived MSCs) [11].
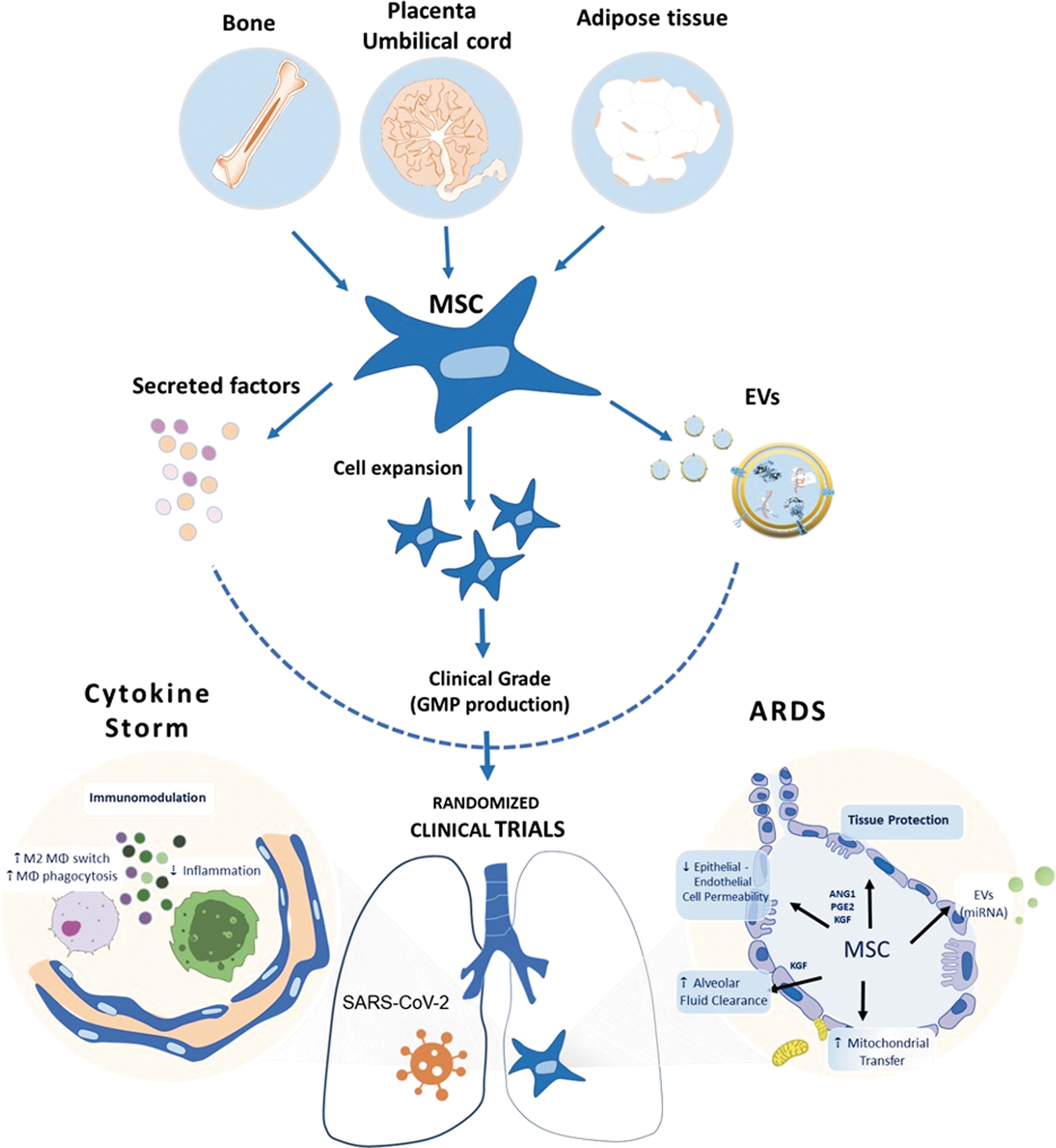
Overview of MSC properties relevant for potential use in COVID-19–related severe respiratory disease.
A recent search (November 2020) of the NIH clinical trial database and the World Health Organization-International Clinical Trial Registry Platform (WHO-ICTRP) revealed >3,787 recently registered clinical trials for COVID-19. Among these are 154 cell and gene therapy-based trials worldwide, with most registered in China (41) and the United States (36). Most of these utilize MSCs or their secreted products, including EVs or conditioned media. In a previous comprehensive review, we had presented an exhaustive summary of ongoing studies registered in the Chinese Clinical Trial Registry (
U.S. Food and Drug Administration Approved MSC-Based Clinical Trials for COVID-19
AdMSCs, autologous adipose tissue-derived mesenchymal stromal cells; ARDS, acute respiratory distress syndrome; BM-MSCs, bone-marrow-derived mesenchymal stromal cells; DMSO, dimethylsulfoxide; EAP, Expanded Access Program; IM, intramuscular; IV, intravenous; SARS-Cov-2, severe acute respiratory syndrome coronavirus 2; UC-MSCs, umbilical-cord-derived mesenchymal stromal cells; ULSC, umbilical cord lining stem cells.
Despite the lack of preclinical information on COVID-19 or any other respiratory virus pathophysiology, there has been clearance by the FDA of an IND application for the use of NK cells in clinical testing [15]. Whether these approaches are even safe for COVID-19 patients has yet to be clarified. As such we urge the FDA and other regulatory agencies to take a careful position with respect to approving cell-based products with unclear track records in either preclinical or clinical studies in lung diseases or critical illnesses for use in COVID 19 patients.
Convalescent T cells isolated from COVID-19 patients are also being considered. Recently, SARS-CoV-2–specific T cells were shown to be polyfunctional and can be expanded from convalescent individuals. These T cells were able to target structural viral proteins, including the C-terminus of membrane protein, making them good candidate for the prevention or early treatment of SARS-CoV-2 infection in immunocompromised patients with blood disorders [16].
Of the recent published reports and small case series from both academic and industry sources suggesting potential efficacy of systemic MSC administration in COVID-19 patients, the available data presented are either anecdotal or from incompletely presented, poorly controlled investigations [2,17]. The situation is also further complicated by lack of consensus or full understanding with respect to MSC source of origin, dose, dosing strategy, use of freshly thawed versus continuously cultured cells, and other factors involved in potential use of MSC-based cell therapies. The same holds for a recently published initial safety investigation utilizing MSC-derived EVs in which no information about the actual biological substance being administered was provided [18]. Therefore, although there may be a potential role for MSCs and other cell-based therapies in treatment of COVID-19, these need to be investigated in a rationally designed, controlled approach if safety and efficacy are to be demonstrated accurately. Importantly, in addition to legitimate peer-reviewed academic trials being conducted globally, one industry-sponsored prospective randomized, double-blinded, placebo-controlled phase 2 (intramuscular injection of placental-MSC,
At a time of unprecedented need, it is natural for patients, families, and caregivers to seek all available options, including access to cell-based and other investigational products, even before adequate demonstration of their safety and efficacy according to regulatory approval. This should not be an excuse for opportunists to sell or advertise unproven therapies of any kind. “Compassionate use” should be conducted in the context of a clinical investigation framed by strict ethical and regulatory permissions, such as expanded access authorization, with the goal of obtaining mechanistic information wherever possible. There must be a strong stance against the rogue stem cell clinic industry, which has already begun to offer unproven therapies for COVID-19. A number of global organizations, including the International Society for Cell and Gene Therapy (ISCT) and the International Society for Stem Cell Research (ISSCR), have taken positions against this predatory behavior [19]. The FDA has recently increased oversight activities against businesses offering unproven therapies, but more regulatory oversight and action are needed [20]. These actions are necessary to develop rationale evidence-based platform for potential use of cell-based therapies both for COVID-19 and for a wider range of respiratory and other diseases potentially amenable to these advanced therapies.
Footnotes
Author Disclosure Statement
M.K. is Assistant Professor at the faculty of medicine of the University of los Andes, Santiago, Chile and Chief Scientific Officer of Cells for Cells and Regenero (Chile), spin-offs of the same University. He receives research support from the Chilean National Agency for Research and Development (ANID), the Economic Development Agency of the Chilean Government (CORFO), Cells for Cells-Regenero and from the University of Los Andes.
L.I. is Associate Professor of Oral Biology at the University at Buffalo, The State University of New York and the Chair of the International Society for Cell & Gene Therapy Presidential Task Force (PTF) on the Use of Unproven and/or Unethical Cell and Gene Therapy. He has written an expert report in a class action lawsuit filed against a business selling unproven stem cell interventions, and wrote the report on a pro bono basis.
M.D. is Professor of Oncology at the University of Modena, Italy. He is a specialist physician at the Department of Medical and Surgical Sciences for Children and Adults, University Hospital of Modena, Italy. He receives research support from Associazione Italiana Ricerca Cancro (AIRC), the Associazione Sostegno Ematologia e Oncologia Pediatrica (ASEOP), and the Associazione ASLEM and MIUR (Progetto Dipartimenti Eccellenti 2017). He has been Chair of the ISCT Presidential Task Force on unproven cell and gene therapy (2014–2020).
K.L. is Professor of Clinical Stem Cell Research at the Division of Clinical Immunology and Transfusion Medicine, Karolinska Institutet and Senior Consultant, Center of Allogeneic Stem Cell Transplantation and Cellular Therapy (CAST), Karolinska University Hospital Huddinge, Stockholm, Sweden. She receives research support from the Swedish Research Council, Stockholm County Council, Swedish Foundation for Strategic Research, Laryngfonden, Karolinska Institutet.
B.L.L. is the Barbara and Edward Netter Professor of Cancer Gene Therapy at the Perelman School of Medicine at the University of Pennsylvania, and President of the International Society for Cell and Gene Therapy. Disclosures of equity: Tmunity Therapeutics. Honoraria: Novartis, Terumo, AstraZeneca. Consulting or Advisory Role: Brammer Bio/ThermoFisher Viral Vector Services, Avectas, Immuneel, Ori Biotech, Vycellix.
D.J.W. is Professor of Medicine at the University of Vermont and Chief Scientific Officer of the International Society for Cell & Gene Therapy. He receives research support from the National Institutes of Health, Department of Defense, Cystic Fibrosis Foundation, and the University of Vermont. He has written an expert report in a class action lawsuit filed against a business selling unproven stem cell interventions, and wrote the report on a pro bono basis.
Funding Information
No funding was received for this work.