
Abstract
A transgenic acute promyelocytic leukemia (APL) murine model established by Michael Bishop by cloning a human PML-RARα cDNA into the hMRP8 expression cassette has been widely used in the all-trans retinoid acid and arsenic preparations for the research of APL. However, in the existing literature, the data of regularity and characteristics of the pathogenesis of this model were still missing, which hinder the development of many studies, especially application of new technologies such as single-cell sequencing. Therefore, in this article, we have made up this part of the missing data using an improved APL murine model. We clarified the effects of different inoculation doses on the onset time, latency, morbidity, life span, and proportion of APL cells in peripheral blood (PB), spleen, bone marrow, and so on. The relationship between the proportion of APL cells in the bone marrow, spleen, and PB and organ histological changes was also revealed. These results were a supplement and refinement of this APL model. It would add to the knowledge base of the field and aid in ensuring that accurate models are used for directed interventions. It also provides a great convenience for the researchers who will carry out similar research.
Introduction
APL is an aggressive type of acute myeloid leukemia in which there are too many immature blood-forming cells (promyelocytes) in the blood and bone marrow (BM) [1,2]. It was caused by a chromosomal translocation that involves the fusion of two genes: the PML gene on chromosome 15 and the RARα gene on chromosome 17, and the protein produced by this fusion was referred to as PML-RARα [2,3]. The mechanism of PML-RARα induced oncogenic transformation has been studied using various APL mouse models [4]. These models included the use of viral transduction, transgenic, and knock-in techniques. Among them, a transgenic APL murine model [5] established by Michael Bishop in 1997 by cloning a human PML-RARα cDNA into the hMRP8 expression cassette has been widely used in the all-trans retinoid acid, arsenic, and arsenic-containing preparations [6] for the research of APL and is still used today. The strong correspondence between human APL and murine leukemia described in this article indicates that the hMRP8-PMLRARα system can be used to obtain information that is directly relevant to the human disease. The leukemia progressed in this model appear to be a faithful reproduction of the human disease, which can be used to explore the pathogenesis and treatment of APL.
Realgar–Indigo Naturalis formula (RIF) is a well-known arsenic-containing preparation used to treat acute promyelocytic leukemia (APL) in China [6 –8]. As an oral preparation, RIF achieved a comparably high rate of remission and survival to intravenous arsenic trioxide as a front-line treatment in newly diagnosed APL in a multicenter randomized clinical trial [9,10]. As we want to clarify the influence of each component in RIF on hematopoietic stem cells (HSCs) and BM stromal cells' taxonomy of APL murine by single-cell sequencing technology, we encountered many difficulties. To meet the experimental purpose and the requirements of single-cell sequencing sample preparation, we need to accurately grasp the life span, onset time of APL cells (APL cell population can be observed in peripheral blood [PB] by flow cytometry, the ratio was set to 0.01%, and the number of collected cells should be no less than 100,000), and the relationship between the proportion of APL cells in the PB and injection time, etc. Despite this murine model has been adopted by many researchers, and there exist many valid data related to hematology, histopathology, toxicology, molecular biology research, etc. But unfortunately, there were no systematic studies of these information, and related regularity or characteristics of pathogenesis cannot be summarized in existing articles.
In this study, an improved murine model which was established by Zhu [11] who labeled the murine APL BM cells derived from hMRP8-PML/RARα transgenic mice (FVB/NJ) with GFP-expressing retroviral vector MigR1 was adopted to carry out systematic research of the regularity or characteristics of pathogenesis. This labeling did not alter APL cells' in vivo repopulation capacity, morphology, and immunophenotype, but it can improve the convenience of detection. We studied the life span, onset time, relationship between the proportion of APL cells in the BM and injection time, the relationship between the proportion of APL cells in BM, spleen, and PB at the same time point, and under different proportions, and the degree of pathological changes in the heart, liver, spleen, kidneys, lungs, and BM of each animal, etc. The sharing of this systematic research results hopes to give a reference for peers in similar research.
Materials and Methods
Animals
All studies were performed with the approval of the Institutional Animal Care and Use Committee at the Academy of Military Medical Sciences (No. IACUC-DWZX-2020-688). Male, adult (6- to 8-week old) FVB/NJ mice were purchased from SPF (Beijing) Biotechnology Co., Ltd. (Production license: SCXK (Jing)-2019-0010). Animals were housed in a specific pathogen-free facility with standard light–dark cycles. The animals were maintained with autoclaved food and water. Health was monitored daily. Studies adhered to the National Institutes of Health's Guide for the Care and Use of Laboratory Animals.
Preparation of samples
The first generation of spleen or BM cells we used for transplantation of leukemia was isolated from several FVB/NJ mice that had progressed to APL; these mice were generously donated by Zhu's team. Mice without leukemia were injected with 1 × 106 spleen cells using the tail vein. When they became moribund, the mice were euthanized by carbon dioxide asphyxiation, and spleen or BM cells were isolated and inoculated into secondary recipients for passage or frozen and stored at −80°C for reserve (Fig. 1).
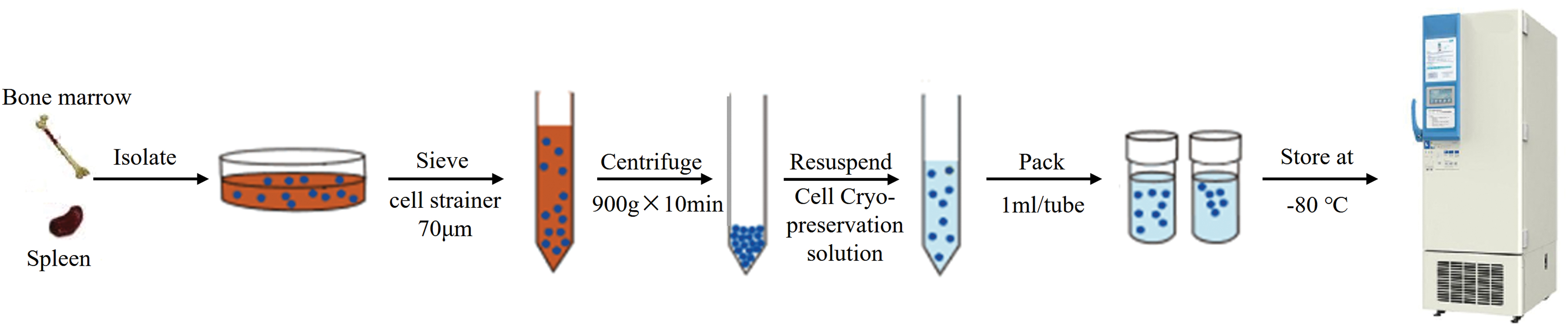
Overview of sample preparation or cryopreservation. Color images are available online.
Transplantation of leukemia
Viable cells isolated from BM, spleen, or lymph nodes of animals with leukemia can be used for inoculation and passage. In this study, spleen cells were selected for transplantation of leukemia. First, we need to determine the cell count and viability of freshly prepared or resuscitated spleen cells by Automated Cell Counter (BIO-RAD TC20™). Then, flow cytometry was used to determine the proportion of APL cells. The results showed that the total count was 2.07 × 106 cells/mL, live count was 1.33 × 106 cells/mL, and the APL cell ratio was 28.8%. Based on the count of live cells, three groups of high, middle, and low inoculation dose were set (Fig. 2a).
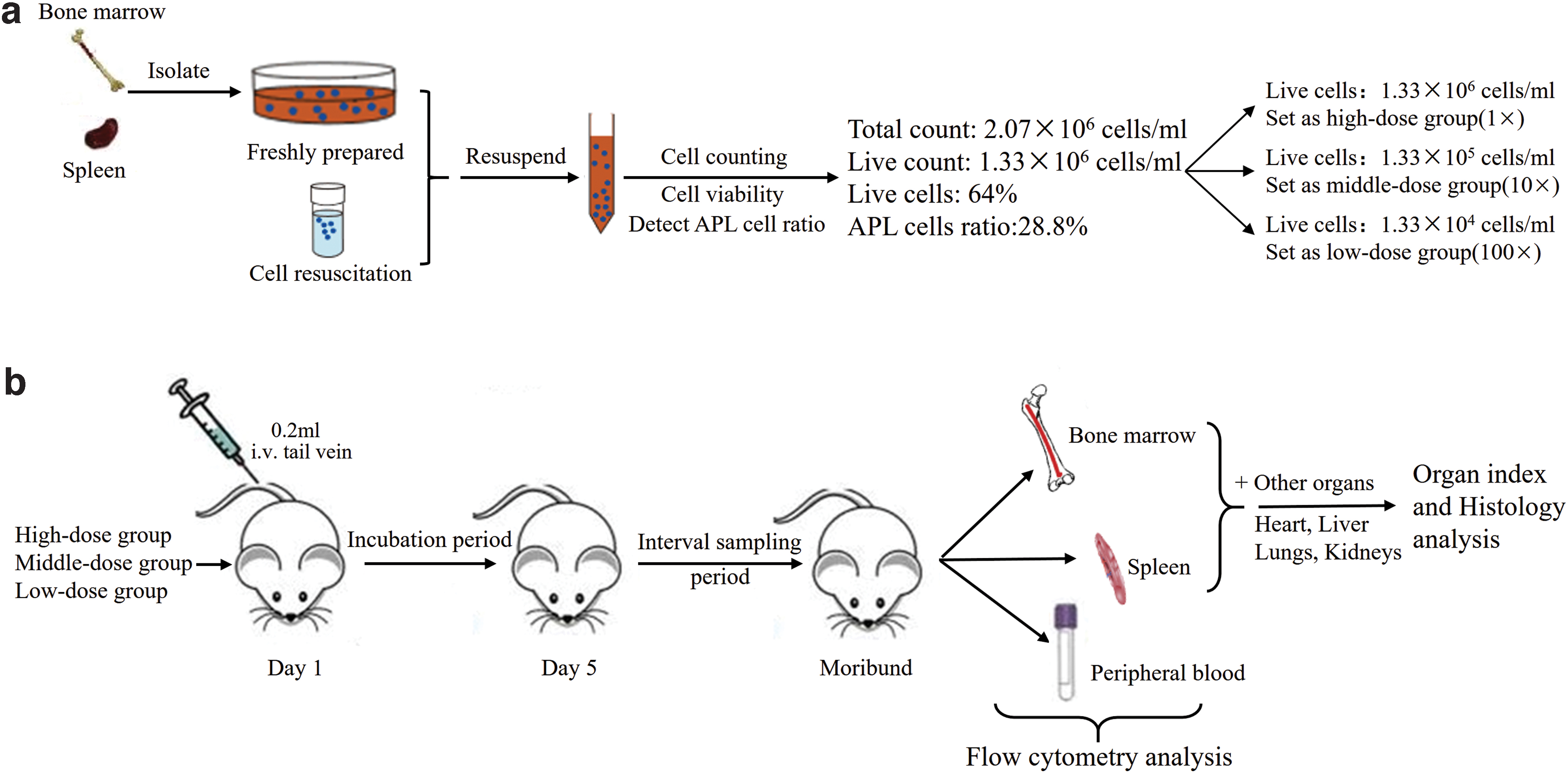
Study overview.
Using a Web-based randomization system, 45 FVB/NJ mice were randomly divided, in a 1:1 ratio, into three groups; three additional mice were used as normal controls. According to the procedure shown in Fig. 2b, each mouse was injected 0.2 mL through the tail vein. Based on experience, day 1–5 is the incubation period of leukemia, and from day 5 to moribund, we will collect samples at different intervals based on the previous results of the APL cells' ratio. Mice were euthanized by carbon dioxide asphyxiation, and femurs, spleen, and PB were collected. BM was flushed out and red blood cells (RBCs) lysed using red blood cell lysis buffer (BD Biosciences). The spleen was weighed and cut into pieces, ground through a 70 μm cell strainer, and RBCs were lysed. The PB only needs to lyse the RBCs. After RBCs were completely lysed, flow cytometry was used to determine the proportion of APL cells in BM, spleen, and PB.
Antibodies and flow cytometry
For flow cytometry, the murine model we used was improved by Zhu's team, and its own new labeled GFP fluorescence can be used to distinguish APL and normal cells; therefore, there is no need to use other antibodies. Fixable viability dye EF780 was used to identify dead or live cells. Flow cytometry analysis was performed on a FACSAria II (BD Biosciences).
For the analysis of HSC, the following mouse antibodies were used: Lineage, APC-CY7 [CD3e, CD45R (B220), Ly6G (Gr1), CD11b, TER-119]; Sca-1, BV605 (Ly6A/E); c-Kit, APC (CD117); CD150, BV421; CD48, PE. These antibodies were purchased from eBioscience (Thermo Fisher).
Organ index and histology analysis
After removing excess fat and connective tissue on the surface, the organs, including the heart, liver, lung, spleen, and kidney, were weighed. Organ index refers to the ratio of organ weight to body weight.
For tissue analysis, tissues, including heart, liver, lungs, kidneys, spleen, and femurs, were fixed with buffered formalin or 4% paraformaldehyde, embedded, sectioned, and stained with H&E according to standard techniques. Slides were dewaxed with xylene and rehydrated through a series of washes with decreasing percentages of ethanol. The slides were examined using a Leica microscope, and images were captured using LAS controller software.
Statistical analysis
The statistical methodology used and sample sizes are described in the individual figure legends. Results are presented as mean ± SD unless otherwise stated. When only two groups were compared, a Student's t-test (two tailed) was used; however, when three or more groups were compared, one-way ANOVA analysis was performed. A significance level cutoff of 0.05 was used unless otherwise stated. Statistical analysis was performed using SAS (Version 9.1), Microsoft Excel, and GraphPad Prism (version 5.0).
Results
Onset time, pathogenesis curve, and survival curve
As shown in Fig. 3a, according to the pathogenesis curves, the onset time of three inoculation groups was different; the onset time of high-, middle-, and low-dose groups was the 7th, 11th, and 18th day, respectively. It usually takes 4–5 days from the first onset until all mice progressed to APL in the groups. All FVB/NJ mice could progress to APL after transplantation.
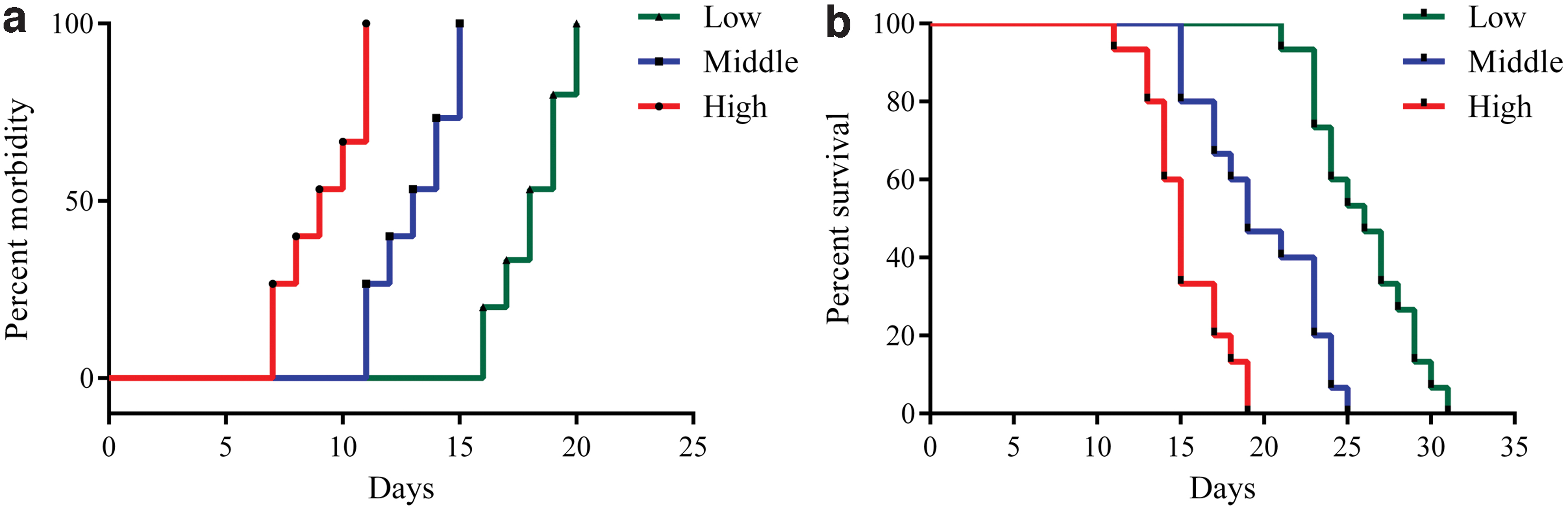
Pathogenesis curves and survival curves.
Corresponding to the pathogenesis curve, Fig. 3b is the survival curve of three inoculation groups. As shown in the figure, the high-, middle-, and low-dose group's life span was different. Without drug intervention, the main reason for this difference was closely related to the inconsistency of the onset time of the three-dose groups. If the maximum survival days of each group were subtracted from the incubation days before onset, the results were 15 days (low dose), 14 days (middle dose), and 12 days (high), respectively. In addition, judging from the proportion of APL cells in the BM we observed, if no additional interventions were taken, once the APL cells were detected, the proportion of APL cells in the BM increases exponentially. These phenomena indicate that different inoculation doses can only affect the onset time and have no significant effect on the life span of animals after onset. Furthermore, after onset, there was no significant difference in life span between the groups.
Relationship between the proportion of APL cells in the PB and transplantation time
The degree of APL progression depends on monitoring the proportion of APL cells in PB. As shown in Fig. 4, we revealed the relationship between the proportion of APL cells in PB and the transplantation time in low-dose, middle-dose, and high-dose inoculation groups. At the beginning of the onset, the proportion of APL cells in PB was about 0.01%; after 3–4 days of accumulation, it reached 1.0–1.5% and then entered the outbreak period. Generally, when dying, the proportion was generally 30–35%, rarely exceeding 40%; at the same time, the proportion in BM was 85–90%, and the bone marrow cavity is filled with APL cells.
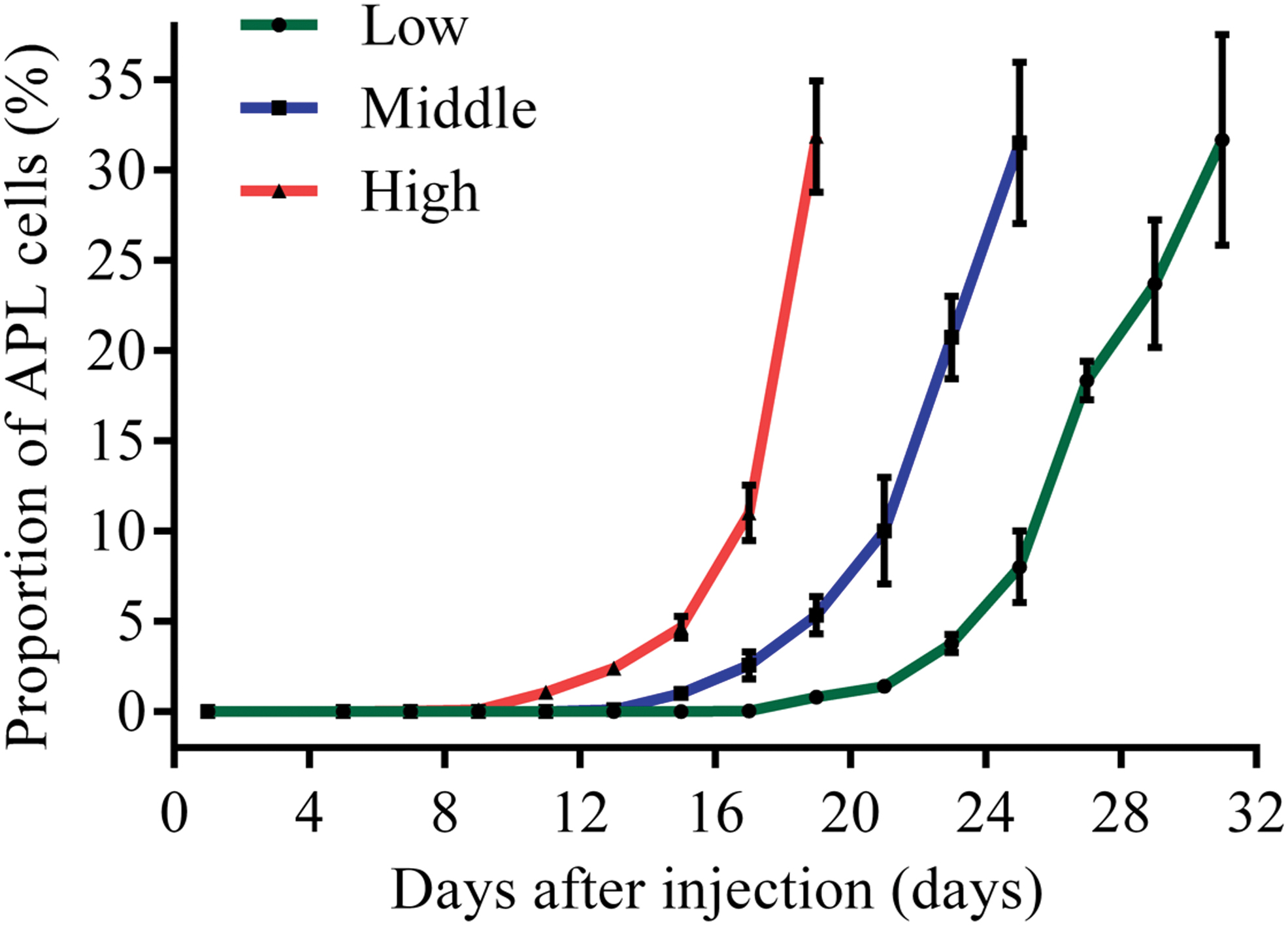
Relationship between the proportion of APL cells in the PB and transplantation time. The error bars represent the standard deviation of measurements for three parallel samples in three separate groups (n = 3). PB, peripheral blood. Color images are available online.
Relationship between the proportion of APL cells in BM, spleen, and PB at same time point
When you want to accurately predict the proportion of APL cells in BM or spleen at a certain time point, monitoring the proportion of APL cells in PB is a feasible solution. Therefore, the relationship between the proportion of APL cells in BM, spleen, and PB at the same time point was helpful. In Fig. 5, we displayed some representative proportion of APL cells in PB, and the corresponding proportion of APL cells in BM and spleen was listed below.
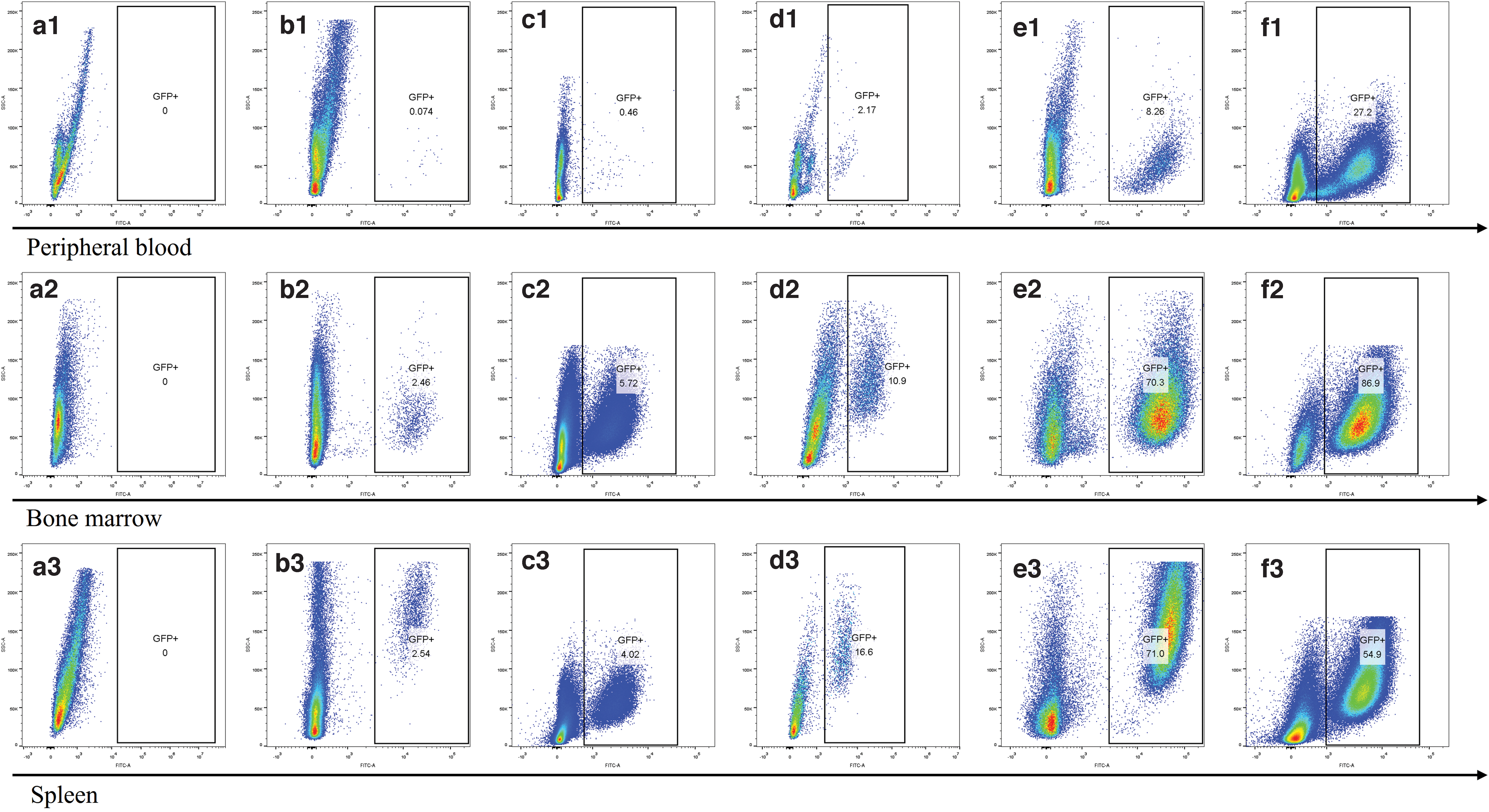
Relationship between the proportion of APL cells in BM, spleen, and PB at same time point. Figures with the prefix of letter “
As shown in the b1, b2, and b3, when the proportion was 0.074% in PB, the proportion in the BM already reached 2.46%, and the proportion in the spleen was 2.54% relative. However, the ratio of 0.074% is prone to false-negative results when the total number of cells is insufficient. Therefore, for some protocols that study early intervention of APL, the proportion of APL cells in BM should be strictly controlled. So we recommend that when monitoring the proportion of APL cells in PB, the events in flow cytometry analysis should be not less than 100,000 to avoid false-negative results.
We must also be aware that whether perfusion or not has a certain effect on the proportion of GFP+ cells in the spleen. This phenomenon is manifested in that the measured value of nonperfused spleen cells is slightly higher compared with perfused spleen cells. Despite the small impact, the trends we show in the article are still accurate and trustworthy.
Relationship between the proportion of APL cells in the BM and its histology change
As shown in Fig. 6, the bone marrow structure of a2 is basically normal, the proportion of hematopoietic cells in each line is normal, and no tumor cells were seen. The proportion of APL cells in bone marrow cells obtained by flow analysis is consistent with the trend observed in hematoxylin-eosin staining (HE) slices. But the proportion obtained by histological analysis is higher than that obtained by flow analysis.
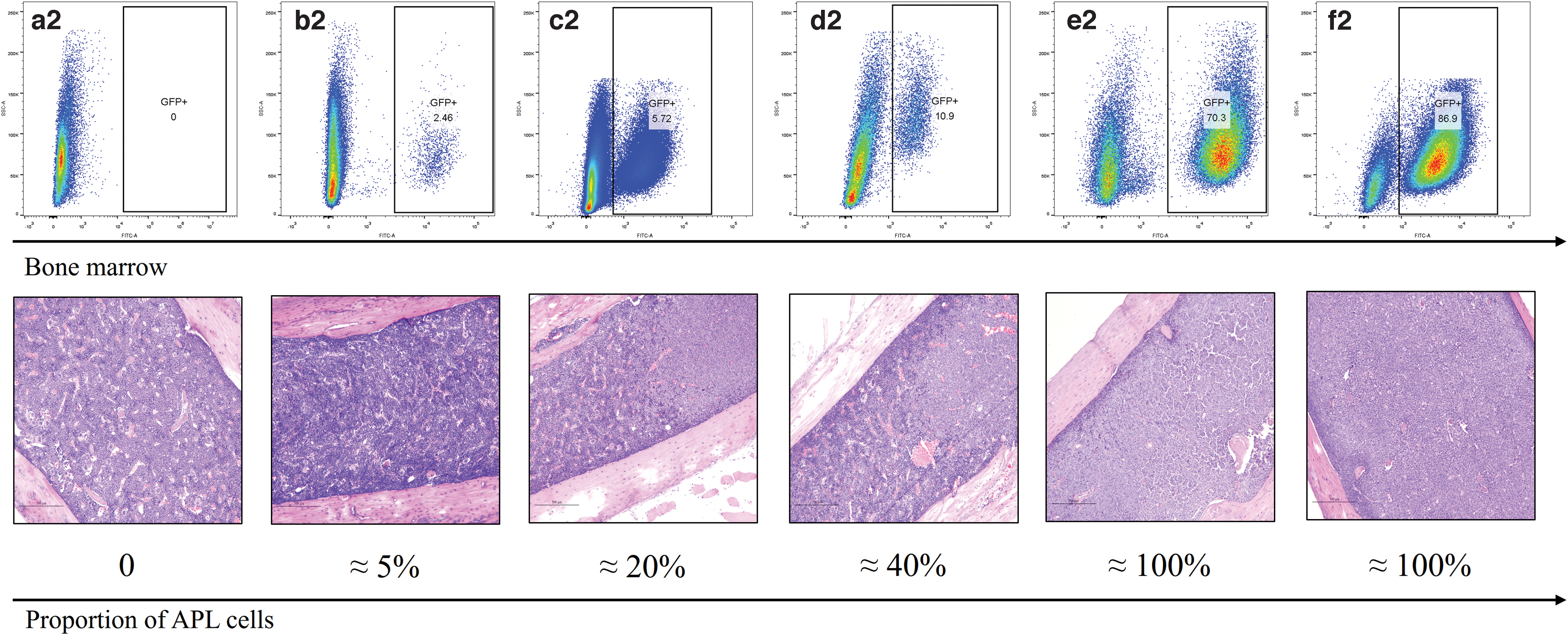
Relationship between the proportion of APL cells in the BM and its histology change. The Figures of
Relationship between the proportion of APL cells in the BM and organ histological change
As shown in Fig. 7, the hepatic lobular structure of a2 was normal, with no congestion in the central vein and the vein of the junction area, and no obvious bleeding and inflammatory cell infiltration were seen. No tumor cells were observed. With the progress of APL, the histological changes of the liver were gradually significant from b2 to f2. From the beginning, tumor cells were only occasionally seen in the liver sinus, and the structure of the liver lobule gradually blurred until disappeared. Diffused tumor cells in the liver sinus gradually formed tumor “nodules”.
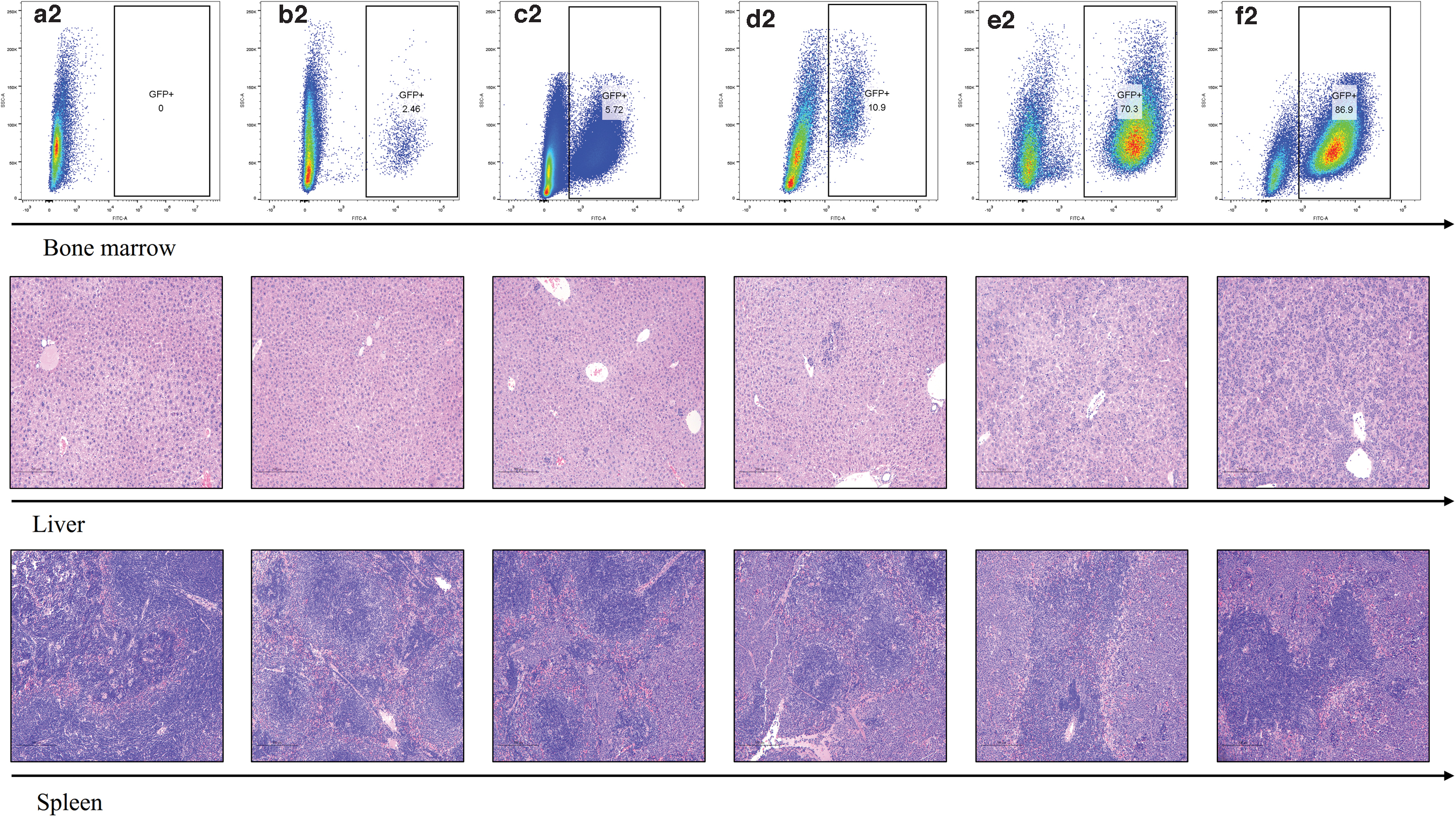
Relationship between the proportion of APL cells in the BM and organ histological change. The Figures of
The trend of histological changes in the spleen is consistent with the liver. The spleen structure of a2 was basically normal, the red pulp and white pulp were clearly demarcated, the splenic corpuscle structure was normal, and no tumor cells were seen. With the progress of APL, in the b2, c2, and d2, few red pulps remain, and the red pulp was infiltrated by tumor cells in different degrees; in the e2 and f2, the structure of the splenic corpuscle is still normal, but the red pulp is almost disappeared, filled with tumor cells.
The histological changes of the heart, kidneys, and lungs are displayed in Supplementary Fig. S1. With the progress of APL, there were no significant differences in the histological changes of the heart and kidneys. However, the lungs' histology changes a lot. Alveoli and alveolar wall of a2 were basically normal; no tumor cells were seen in lung tissue. In the b2, c2, and d2, alveoli and alveolar wall were basically normal; occasional focal hemorrhage, mild congestion of alveolar wall blood vessels, a bit of monocyte, lymphocytes, and occasionally neutrophils were observed. In the e2 and f2, mononuclear cells and lymphocytes increased in the alveolar septum, and small blood vessels containing tumor cells gradually increased, tumor cells in the blood vessels also gradually increased, filling in the lumen to form tumor thrombus, and the cells of the tumor thrombus resulted in degeneration and necrosis to varying degrees. We even observed tumor cells outside of the blood vessels and inside the alveolar cavities of f2.
The most obvious change in the organ index (data not shown) was spleen. With the progress of APL, APL cells in the spleen gradually increased and the spleen gradually enlarged. At the end point of sampling, the spleen index has a very significant difference (P < 0.001) compared with the NC group. The rest of the organs include the heart, liver, kidneys, and lungs. Its organ index changes are not significant during the progression of APL.
Relationship between the proportion of APL cells in the BM and HSC
Near the end of the experiment, we analyzed the changes of HSCs and their components in the bone marrow of APL animals. As shown in Fig. 8 and Table 1, the ratio of total HSC (Lineage−Sca-1+c-Kit+) cells in the bone marrow was significantly lower (P < 0.02) than that in the NC group. Among the three components of total HSC, the trend of HPC-1 (CD150−CD48+Lineage-Sca-1+c-Kit+) was consistent with total HSC, which was obviously decreased compared with the NC group (P < 0.02). In contrast, LT-HSC (CD150+CD48−Lineage−Sca-1+c-Kit+) (P < 0.05) and MPP (CD150−CD48−Lineage−Sca-1+c-Kit+) (P < 0.001) were significantly increased compared to the NC group.
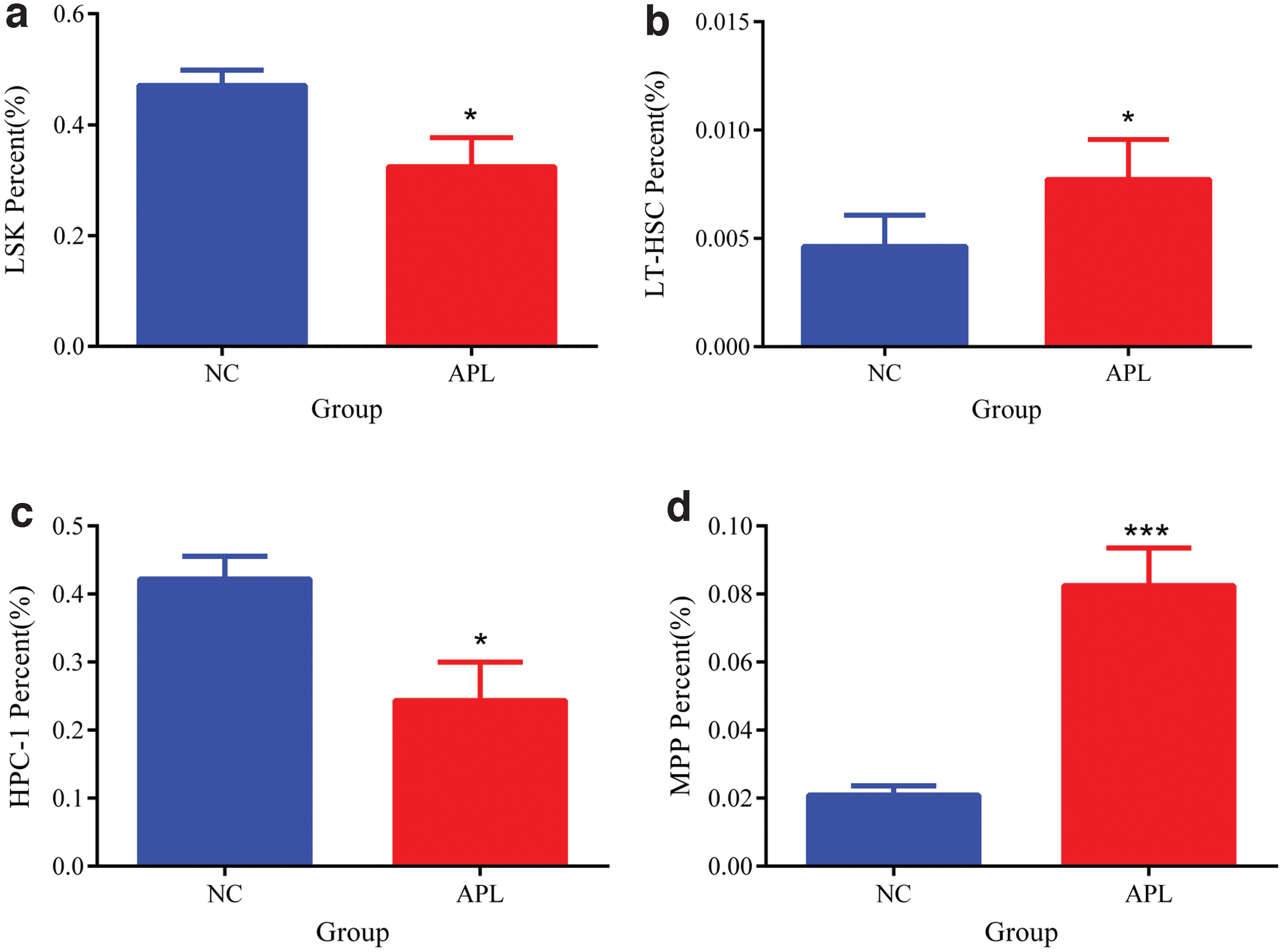
Relationship between the proportion of APL cells in the BM and HSC.
Relationship Between the Proportion of Acute Promyelocytic Leukemia Cells in the Bone Marrow and Hematopoietic Stem Cell
“*” means P < 0.05.
“***” means P < 0.001, n = 4.
APL, acute promyelocytic leukemia;
Discussion
Initially, the purpose of our study is to clarify the influence of each component in RIF on HSCs and bone marrow stromal cells' taxonomy [12]. To further explore the rule of compatibility of monomers in RIF from the perspective of hematopoiesis, single-cell -omics technology was adopted to conduct this research. When conducting this study, a suitable sampling end point is very important. This end point should meet a necessary administration period of RIF, and the ratio of HSCs and bone marrow stromal cells in the bone marrow should be in an appropriate range. This appropriate range refers to the characteristics of bone marrow HSCs and bone marrow stromal cells that cannot be completely obscured by APL cells [13], and the ratio of these cells should be friendly to flow cytometry sorting. To meet these two requirements, the relationship between the onset time of APL mice, the life span, and the proportion of APL cells among BM, spleen, and PB at different time points must be clarified.
In the original article of professor Bishop [5], the onset time of the mice transplanted leukemia cells was 3–5 weeks. In another article [6], after 1 × 105 cells expressing PML-RARα were injected, the onset time of the mice was not reported, but the life span of the APL control group was 25 days. These data were consistent with the low-dose and middle-dose group's onset time and life span in this study. However, these two articles did not specify the relationship between onset time and the number of injected leukemia cells. The data presented in this article is a supplement and refinement to the previous work.
Understanding the precise process of APL in mice was also very important for formulating the intervention plan or mechanism research of certain drugs. Our results show that the onset time is positively correlated with the injected number of cells expressing PML-RARα. Our results can provide a great convenience for subsequent researchers, taking the results of this article as an example; if they need a period of latency longer than 15 days for drug administration, the number of injected cells should be consistent with the low-dose group.
Based on the results of this article, the experiment of single-cell sequencing was performed to study the effects of RIF components on bone marrow HSCs and bone marrow stromal cells. The low-dose transplantation group was selected as the APL control group; all mice were monitored for the proportion of APL cells in the PB from the 13th day after injection. Until about day 20, the proportion of APL cells in the PB of the APL control group was 0.9–2.0%, and this time point was selected as end point of sampling. After single-cell omics analysis, we successfully sorted out bone marrow HSCs and bone marrow stromal cells [14] and divided these two types of cells into 17 subclusters. Through cell identification of subclusters, we found that Tanshinone IIA and Indirubin in RIF can maintain the stability of the bone marrow stromal cell population by affecting the development of osteoblasts. The maintenance of this steady state can amplify the differentiation and direct killing effect of arsenic trioxide on APL cells (data not showed). This is very important evidence for scientifically explaining the mechanism of RIF compatibility. Furthermore, it is an example of a successful application of the results in this article.
Some of the data in this article also had limitations. In the histological analysis, HE analysis is not sensitive enough to the detection of APL cell infiltration in organs in the early stage of APL. However, for this article, HE analysis was sufficient to discover the relationship between APL progression and the trend of organ histology changes. For researchers who are concerned about the organ histology changes, immunohistochemistry is a recommended improvement method.
Conclusion
This article was based on an improved, widely used, and transgene-initiated murine APL model, aiming at the lack of regularity and characteristic data of pathogenesis. The relationship between different transplant doses of spleen cells, which expressed PML-RARα and the onset time, latency, morbidity, and life span of the APL model, was discovered. Relationship between the proportion of APL cells in BM, spleen, and PB and injected time and organ histology changes were revealed. These results were a supplement and refinement of the regularity and characteristics of this APL model. The data shared in this article provide great convenience and help researchers who will use this model to conduct research.
Footnotes
Acknowledgment
The authors thank Xiang-Tao Luo for supporting animal experiments.
Author Disclosure Statement
The authors declare no conflict of interest.
Supplementary Material
Supplementary Figure S1
Funding Information
This research was funded by the National Natural Science Foundation of China (81703669) and National Science and Technology Major Project of “Major New Drug Creation” (2017ZX09301012-007).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.