
Abstract
Steroid-refractory graft-versus-host disease (GvHD) is a life-threatening complication after allogeneic hematopoietic stem cell transplantation (alloHSCT). Alternative treatment options are often insufficient. Several studies have proven the efficacy of mesenchymal stromal cells (MSCs) in the treatment of therapy-refractory acute GvHD in adult and pediatric patients. Long-term data in pediatric patients are scarce. In this retrospective analysis, a total of 25 patients with a median age of 10.6 years (range 0.6–22.1 years) who received bone marrow-derived MSCs after alloHSCT for the treatment of steroid-refractory III and IV GvHD were analyzed. The median observation period of the surviving patients was 9.3 years (1.3–12.7 years) after HSCT. Among the 25 patients, 10 (40.0%) died [relapse (n = 3), multiorgan failure (n = 6), cardiorespiratory failure (n = 1)] at median 0.5 years (0.2–2.3 years) after HSCT. Partial response and complete remission (PR, CR) of the GvHD were achieved in 76.0% and 24.0% of the patients, respectively. Transplant-related mortality was 0% in the patients who achieved CR after MSC treatment and 26.3% for those with PR. A median improvement by one intestinal or liver GvHD stage (range 1–4) could be achieved after MSC application. No potentially MSC-related long-term adverse effects, for example, secondary malignancy, were identified. In conclusion, the intravenous application of allogeneic MSCs was safe and proved effective for the treatment of steroid-refractory GvHD. However, larger, prospective, and randomized trials are needed to evaluate these findings.
Introduction
Acute and chronic graft-versus-host diseases (GvHDs) are immunological adverse reactions that can occur after allogeneic hematopoietic stem cell transplantation (alloHSCT) driven by donor T cells responding to alloantigens of the recipient. This reaction triggers an inflammatory signaling cascade of cytokines and a dysregulation of the immune system, leading to the destruction of the host tissue. GvHD remains a leading cause of transplant-associated morbidity and mortality in patients after alloHSCT [1].
The incidence of acute GvHD in pediatric patients is highly dependent on the patient characteristics, the transplantation conditioning, and GvHD prophylaxis regimen, varying between 20% and 80% [2,3]. The first-line therapy of acute GvHD includes glucocorticoids, while treatment options for steroid-refractory GvHD include infliximab, tyrosine kinase inhibitors, mechanistic target of rapamycin inhibitors (eg, sirolimus), several different T lymphocyte antibodies [eg, anti-CD3 antibody OKT3, antithymocyte globulin (ATG), alemtuzumab, anti-CD147 antibody ABX-CBL], tumor necrosis factor alpha (TNF-α) antagonists (eg, etanercept), integrin antagonists (eg, vedolizumab), IL-12/IL-23 antibody ustekinumab, anti-CD25 antibody basiliximab, chemotherapeutics [eg, methotrexate (MTX), cyclophosphamide], immunomodulatory agents [eg, mycophenolate mofetil (MMF), janus kinase inhibitors (ruxolitinib)] or as additional therapy extracorporeal photopheresis (ECP), psoralen and ultraviolet A (PUVA) and mesenchymal stromal or stem cells (MSCs) [4 –7]. As shown in a comprehensive meta-analysis, complete response rates of these agents vary between 8% and 68.8% (antibodies), 15%–62% (TNF-α antagonists), and 15%–31% (chemotherapeutic and immunomodulatory agents). Etanercept and glucocorticoids were significantly more likely to achieve complete remission (CR) after 4 weeks of treatment compared with an external control group treated with glucocorticoids alone (69% vs. 33%; P < 0.001). Moreover in grade III and IV acute GvHD, the median survival rate in studies published after 2000 is 17% at 1–3 years [8].
Therapeutic infusion of MSC has been widely investigated in recent years as a novel treatment option for these patients [9 –16]. Bone marrow-derived MSCs are known regulators of the hematopoietic system. Thus, they support hematopoietic stem cells during hematopoiesis [17,18]. Investigations into the detailed mechanisms of their immunomodulatory effects have shown that MSCs exert both innate and adaptive immune responses with local or systemic effects mediated by cytokines, growth factors, exosomes, chemokines, and other anti-inflammatory molecules and metabolites [19 –23]. Several studies have proven effects of MSCs on chemotactic behavior and the differentiation or proliferation of B cells, natural killer cells, and dendritic cells, as well as a key role of MSCs at immunological checkpoints [12,24,25].
Clinical studies in adult and pediatric patients after alloHSCT have shown positive effects of MSC on steroid-refractory GvHD as well as a reduction of transplant-related mortality. In particular, MSC infusion has proven safe, and no proven MSC-related side effects have been observed in these patients [10,11,13,14,17,26 –35]. In children with refractory GvHD, pooled MSC products from multiple third-party donors achieved partial response (PR) rates between 61% and 80% and a significantly improved overall survival after 100 days. Acute infusional toxicity of the MSC product did not occur [36,37]. A systematic meta-analysis of the efficacy of MSC treatment of patients with therapy- or steroid-refractory GvHD including 13 studies with a total of 333 patients found that children tended to achieve higher complete response rates compared with adult patients. Infusion-related toxicity was generally low. Only three studies reported possible MSC-related acute adverse reactions, including one patient with a cardiac ischemia after 24 h after MSC infusion, one patient who needed transfer to the intensive care unit after the second MSC infusion, and one patient showing calcified ectopic lesions. Although an association between the number of GvHD affected organs and the response rate to the MSC therapy was not found, it was shown that it was more likely for patients with acute steroid-refractory skin GvHD to achieve a CR compared with patients with steroid-refractory intestinal or liver GvHD [38].
Currently, there are little long-term survival data for patients after MSC administration, especially for pediatric patients. The primary objective of this work was to analyze data of the long-term follow-up after application of allogeneic MSC for the treatment of steroid- and/or therapy-refractory skin, intestinal and/or liver GvHD in pediatric and young adult patients.
Materials and Methods
Compliance with ethical standards
This analysis was performed in accordance with the Helsinki declaration adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 64th WMA General Assembly, Fortaleza, Brazil, October 2013. The legal basis for the data processing is Art. 6, 7, 9, 89 of the general data protection regulation European Union (EU) 2016/679 of the EU in combination with §§ 4, 5, 6, 8, 9, 12, 13 of the Landesdatenschutzgesetzes Baden-Württemberg in its current form of May 25, 2018. Application of MSC was performed in the course of an individual treatment approach in compliance with the Ethics Committee of the University Hospital Tübingen and the Eberhard Karls University of Tübingen. Approval for this retrospective analysis was granted by the Ethics Committee of the University Hospital Tübingen and the Eberhard Karls University of Tübingen (ID No. 665/2019BO2). Formal consent is not required for this type of study.
Patients
Data of patients of the University Children's Hospital Tübingen, who underwent an alloHSCT between 2004 and 2017, who were diagnosed with a steroid- or therapy-refractory intestinal or liver GvHD stage ≥2 after inefficient first-line treatment, and who received MSC at the University Children's Hospital Tübingen only between 2006 and 2017 were retrospectively analyzed. The data were collected from the chart documentation and clinical records, including the time from HSCT until last patient contact. The data were transferred to pseudonymized case report forms, and started on the day of the beginning of the steroid therapy and ended 4 weeks after the last MSC application. During the in-patient stay, patients are visited at least once daily. Long-term follow-up data were identified and searched using the institutional IT system. Patients with repeated HSCT or incomplete chart documentation of the time before and after MSC application were not included in this analysis.
GvHD diagnosis
Staging and grading of acute and chronic intestinal GvHD were performed according to the current diagnostic criteria based on the criteria first described by Glucksberg et al. [39 –41]. Intestinal GvHD stages 1–4 were clinically diagnosed by the quantity of feces [mL per day (d)] and frequency of bowel movements (n per d), and/or confirmed by histopathological staining of bowel biopsies. To assess remission or progression of GvHD after MSC application, the quantity of feces and frequency of bowel movements were analyzed on a daily basis. Liver GvHD was diagnosed by an increase of direct bilirubin >2 mg/dL in the peripheral blood. Blood analyses including determination of direct bilirubin and transaminases were performed daily. Skin GvHD was diagnosed with the occurrence of maculopapillary exanthema and, if necessary, histopathological staining of skin biopsies.
Indication for MSC treatment and inclusion criteria
The indication for the treatment with MSC after alloHSCT was given by diagnosis of a steroid- or therapy-refractory intestinal or liver GvHD stage ≥2 after inefficient first-line treatment with intravenous prednisolone [2 mg per kg bodyweight and day (mg∙kg BW−1∙d−1)], methylprednisolone (10 mg∙kg BW−1∙d−1), or dexamethasone [10 mg per square meter of body surface area and day (mg∙m−2∙d−1)] for at least seven days and intravenous administration of cyclosporine A (CSA) until a target serum concentration of 150–200 ng/mL was reached. A combination with other GvHD therapeutics including infliximab, tacrolimus, ATG, etanercept, muromonab, vedolizumab, alemtuzumab, ruxolitinib, MMF, azathioprine, ECP, or PUVA was allowed. Data of patients who received MSC between 2006 and 2017 were analyzed.
MSC donors
MSC donors underwent a comprehensive virological and microbiological laboratory assessment before donation. This assessment included determination of toxoplasmosis and syphilis titers, IgG and IgM status for varicella zoster virus, herpes simplex virus, Epstein-Barr virus, cytomegalovirus, and adenovirus. IgM and IgG status of human immunodeficiency virus (HIV), hepatitis A virus, hepatitis B virus, and hepatitis C virus (HCV) were analyzed. In addition, polymerase chain reaction testing for HIV and HCV was performed. Donors were cleared for bone marrow donation with overall negative results.
Expansion of MSC
MSCs were applied in accordance with §13 and §72 of the “Gesetz über den Verkehr mit Arzneimitteln” (German Medicines Law) and licensed by the Regierungsprädisium Tübingen, Baden-Württemberg, Germany (DE-BW-01-MIA-2013_0047/DE_BW_UKT_Immunlabor). Animal sera-free expansion of MSC was performed as described previously [42 –44]. In brief, 20 mL of heparinized bone marrow were aspirated from the spina iliaca superior posterior of the MSC donor (respective HSCT donor or third-party donor). Red blood cell lysis of the aspirate was performed at room temperature with ammonium chloride lysis buffer (8.29 g NH4Cl, 1 g KHCO3, 37 mg Na2EDTA · H2O, 1,000 mL double deionized H2O) for 5 min. After washing with Hank's balanced salt solution, cells were resuspended in 50 mL of low-glucose Dulbecco's modified Eagle's medium (Cambrex, Verviers, Belgium) supplemented with 5% (v/v) fresh frozen plasma (Center for Clinical Transfusion Medicine Tübingen), 5% (v/v) platelet lysate (starting concentration 1 × 108 platelets per mL plasma; Center for Clinical Transfusion Medicine Tübingen), and 1 mM glutamine (Cambrex). Cells were cultured for 48 h at 37°C under an atmosphere of saturated humidity and 10% CO2. Adherent cells were passaged at 80% confluency using trypsin (Cambrex). MSCs were reseeded at a density of 200 cells/cm2 in 175 cm2 flasks (Corning, Corning, NY). Cell harvest was performed after three passages. MSCs were harvested, washed, and resuspended in 50 mL physiological NaCl solution containing 0.1% human albumin (Octapharma, Langenfeld, Germany), passed through a 70 μm cell strainer (Corning) and transfused within 60 min over a period of 15 min.
MSC release criteria
MSCs were released for donation after being cultured for <4 weeks, when a viability of >80% was proven, and when a surface expression of CD73, CD90, and CD105 (>90% of the cells) and absence of expression of CD45 (<2% of the cells) as assessed by flow cytometry analysis (FACSCalibur; BD Biosciences, Franklin Lanes, NJ) were observed. Sterility of the graft was assessed at the start of cell culture and during the last passage.
MSC application
After release, MSCs were administered either as an intravenous infusion or through a central or peripheral venous access (eg, Hickman catheter) within 3–5 min. The MSCs were administered directly after cell harvest or from thawed aliquots of previously frozen lots. Frozen cells were thawed, washed in 0.9% NaCl solution, and administered within 1 h after thawing.
Remission
PR was defined as an improvement of the affected organ system (intestinal or liver GvHD according to the Glucksberg criteria) for which they were treated with MSC by at least one GvHD stage. The time to response (by one GvHD stage) was analyzed, and compared with respect to the malignancy of the underlying disease and the initial overall GvHD grade as diagnosed before the MSC application. CR was defined as complete regression of all clinical symptoms. Nonresponse was defined as no clinical improvement (0 stages) within 4 weeks after the first administration of MSCs.
Safety and tolerance
The safety and tolerance analysis in this study included assessing the occurrence of acute adverse events associated with the infusion of allogeneic MSC, such as tachycardia, infusion-related allergic reactions, respiratory distress, dizziness, hypo- or hypertension as documented, as well as the long-term observation of the occurrence of malignancies until the last documented patient contact. To minimize the risk of malignant transformation of MSCs, we followed the manufacturing recommendations for good manufacturing practice-compliant production of MSCs [43].
Statistical analysis
The overall patient survival probability was determined using the Kaplan–Meier estimator. The median survival time was considered from the time between the first MSC administration and the last follow-up or date of death. Significant differences of the overall survival between analysis groups (eg, malignant vs. nonmalignant disease or age groups) were identified using the Logrank (Mantel-Cox) test. For estimation of the non-relapse mortality cumulative incidence curves were used, considering relapse mortality as a competing interest. Linear regression curves were used to identify a correlation between patient age and improvement of GvHD stages after MSC application.
Graphs and statistical tests were created with GraphPad Prism version 8.1.1 (330) for Windows (GraphPad Software, Inc., La Jolla, CA) and R version 3.5.1 (2018-07-02, Copyright 2018, The R Foundation for Statistical Computing). All statistical tests were two sided. P values <0.05 (*), <0.01 (**), <0.001 (***), and <0.0001 (****) were defined as statistically significant.
Results
Patient characteristics
Between September 2006 and November 2017, a total of 25 patients [8 female (32%), 17 male (68%)] with a median age of 10.6 years [range 0.6–22.1 years; 23 pediatric (92%) and 2 young adult (8%) patients] received a total of 65 MSC applications for the treatment of a steroid- or therapy-refractory GvHD. MSCs were applied at a dosage of median 1.3 × 106 cells/kg BW (range 0.3–39.5 × 106 cells/kg) maximum once every 2 weeks and at median once per patient (range 1–16 applications per patient). Patients underwent alloHSCT for the treatment of malignant disorders in 14 cases (56%) and nonmalignant diseases in 11 cases (44%). They received grafts from a matched family donor (n = 5; 20%), a mismatched family donor (n = 6; 24%), a matched unrelated donor (n = 12; 48%), or a mismatched unrelated donor (n = 2). For GvHD prophylaxis, patients received ATG (n = 10; 40%), CSA (n = 18; 72%), thymoglobulin (n = 10; 40%), MMF (n = 7; 28%), MTX (n = 15; 60%), muromonab (n = 5; 20%), and alemtuzumab (n = 1; 4%). Detailed patient characteristics, HSCT modalities, and the applied GvHD prophylaxis or therapy applied are presented in Table 1.
Patients, Hematopoietic Stem Cell Transplantation Modalities, and Graft-Versus-Host Disease Prophylaxis and Therapy
Alemtuz, alemtuzumab; ALL, acute lymphoblastic leukemia; AML, acute myeloid leukemia; ATG, antithymocyte globulin; Azathiop, azathioprine; BDAn, blackfan-diamond anemia; Bus, busulfan; BW, bodyweight; ChHS, Chédiak-Higashi syndrome; CML, chronic myeloid leukemia; CP, cyclophosphamide; CSA, cyclosporine A; Dexa, dexamethasone; ECP, extracorporeal photopheresis; Etanerc, etanercept; Eto, etoposide; EwS, Ewing's sarcoma; FAnem, fanconi anemia; Flu, fludarabine; Gemt, gemcitabine; HLH, hemophagocytic lymphohistiocytosis; Inflix, infliximab; JMML, juvenile meylomonocytic leukemia; MDS, myelodysplastic syndromes; Melph, melphalan; MFD, matched family donor; MLD, metachromatic leukodystrophy; MMFD, mismatched family donor; MMUD, mismatched unrelated donor; MTX, methotrexate; Mucopolys, mucopolysaccharoidosis; MUD, matched unrelated donor; Muro, muromonab; MMF, mycophenolate mofetil; MPredn, methylprednisolone; Predn, prednisolone; PUVA, psoralen and ultraviolet A; Ritux, rituximab; Ruxo, ruxolitinib; SCID, severe combined immunodeficiency; SCA, sickle cell anemia; Tacr, tacrolimus; TBI, total body irradiation; TCR, T cell receptor; Thiot, thiotepa; Thymo, thymoglobulin; TLI, total lymphoid irradiation; TNC, total nucleated cells; Treo, treosulfan; Vedo, vedolizumab.
GvHD diagnosis and therapy
The patients had a median maximum acute GvHD grade of III (range III–IV). Three of the 25 patients (12%) later developed a chronic extensive GvHD (cGvHD). Manifestation of acute GvHD was at median 30 days after HSCT (range 11–77 days), while cGvHD was initially diagnosed at a median of 132 days (100–418 days) after HSCT. Skin GvHD was diagnosed in 20 patients (80%) with a median stage of 2 (range 1–3), intestinal GvHD was diagnosed in 25 patients (100%) with a median stage of 3 (range 2–4), and liver GvHD was diagnosed in 4 patients (16%) with a median stage of 3 (range 2–4).
Of the 25 patients, 21 (84%) were treated for steroid-refractory intestinal GvHD III–IV, 4 of whom (16%) were treated for multiple affected organs (intestinal GvHD III–IV and additional liver GvHD II–IV). As an additional finding, 20 patients (80%) were diagnosed with acute skin GvHD (median stage 2, range stages 1–3) (Table 2).
Graft-Versus-Host Disease and Mesenchymal Stromal Cell Application
Indicates improvement of the organ system, the patients were treated for with MSC.
adm., administration; aGvHD, acute graft-versus-host disease; cGvHD, chronic extensive GvHD; CR, complete remission; CRF, cardiorespiratory failure; Max., maximum; MOF, multiorgan failure; MSC, mesenchymal stromal cell; PR, partial response; RUD, relapse of the underlying disease.
All 25 of the patients with acute GvHD received GvHD first-line therapy with steroids for median 36 days (range 14–198 days). Before being chosen to receive MSC for the treatment of their acute or chronic GvHD, the patients had received a standard GvHD therapy with prednisolone at a dosage of 2 mg/kg body weight for ∼1 week (n = 25; 100%) and/or prednisolone plus methylprednisolone (n = 17; 68%) at a dosage of 10–20 mg/kg bodyweight for ∼3 days, and—if required—additional GvHD therapy including infliximab (n = 17; 68%), CSA (n = 1; 4%), tacrolimus (n = 13; 52%), dexamethasone (n = 1; 4%), ATG (n = 3; 12%), etanercept (n = 1; 4%), muromonab (n = 1; 4%), vedolizumab (n = 1; 4%), ruxolitinib (n = 1; 4%), MMF (n = 9; 36%), azathioprine (n = 1; 4%), ECP (n = 2; 8%), and/or PUVA (n = 2; 8%), without clinically relevant improvement of their GvHD. The patients were then treated with allogeneic MSC. The GvHD characteristics of each patient are displayed in Table 2, while a summary and analysis of the GvHD characteristics are provided in Table 3.
Graft-Versus-Host Disease—Outcomes
Staging and grading of acute and chronic GvHD were performed according to the criteria formulated by Glucksberg and colleagues [39 –41].
n, sample size; N, total number of analyzed subjects.
MSC application
The patients received the first MSC application at median 82 days after HSCT (range 22–446 days) and at median 50 days after the occurrence of acute GvHD (range 8–426 days). From the patients with multiple MSC application (n = 6; 24%), the last MSC application was performed at a median of 283 days (range 99–1,452 days) after HSCT. A total of 65 MSC doses were applied once every 2 weeks at the most, and at median once per patient (range 1–16 applications per patient). The median dosage was 1.3 × 106 cells per kg BW (range 0.3–39.5 × 106/kg BW). Of the 25 patients, 9 (36%) received MSC from their HSCT donor, while the other 16 patients (64%) received MSC from a third-party donor (Table 2).
Survival
Overall, 10 of 25 patients (40%) died during the observation period. Causes of death were multiorgan failure (n = 6; 24%), relapse of the underlying disease (RUD; n = 3; 12%), or cardiorespiratory failure (n = 1; 4%). The median survival time of the patients who died after HSCT was 0.5 years (range 0.2–2.3 years; Fig. 1a). The median observation period and the survival time of the patients who survived was 9.3 years (range 1.3–12.7 years) (Table 2).
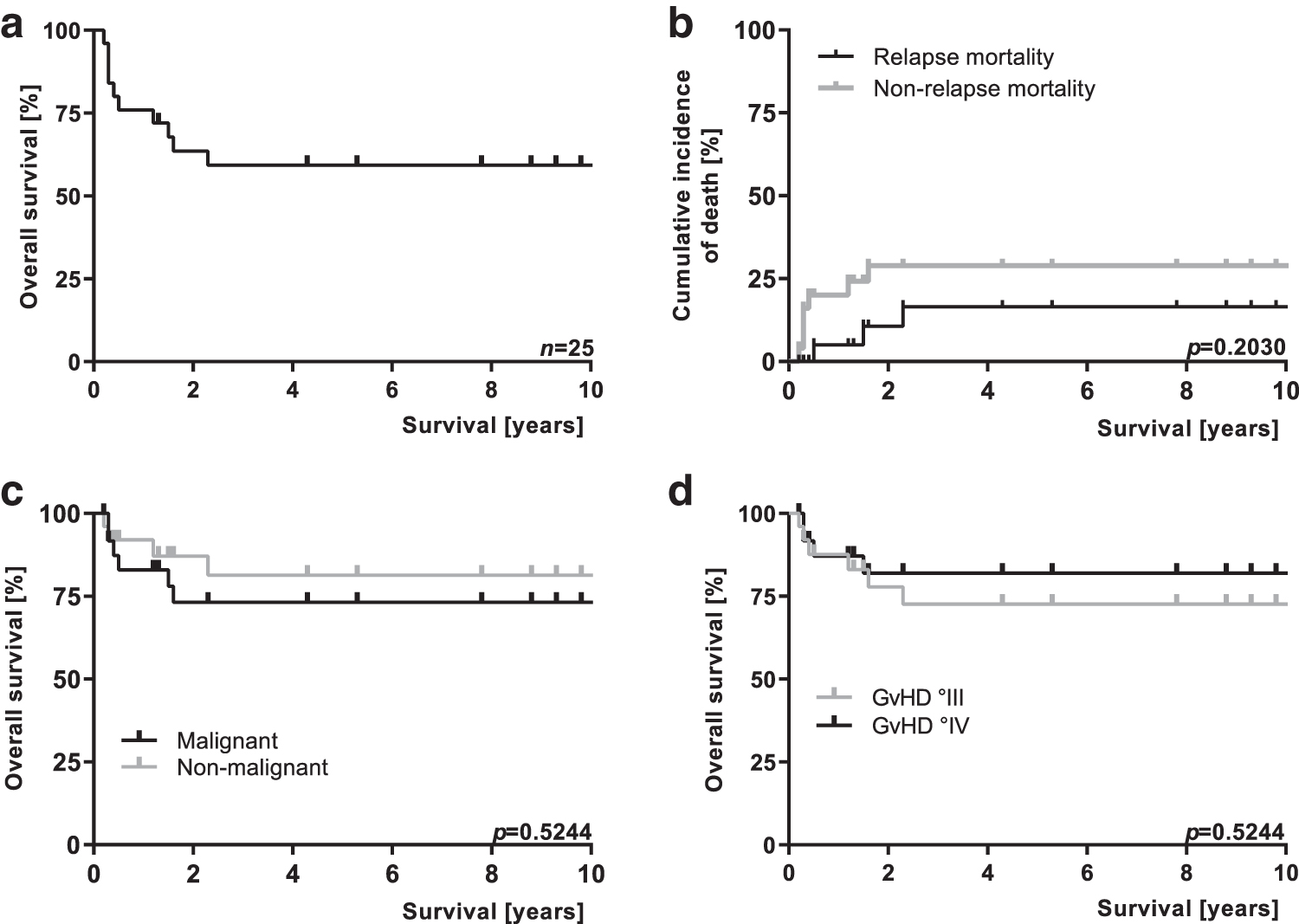
Survival. The graph shows the overall survival of all patients
A CR of the GvHD occurred in 6 of 25 patients (24%). One of these six patients died from RUD. The median survival time of the patients with a CR was 4.1 years (range 2.3–10.2 years).
A partial remission of the GvHD occurred in 19 of 25 patients (76%). The median survival time of these patients was 4.3 years (range 0.3–11.7 years).
Cumulative incidences of death were not significantly different between patients with relapse or nonrelapse mortality (P = 0.2030; Fig. 1b). Likewise, the overall survival of patients was not significantly different depending on the malignancy of their underlying disease (P = 0.5244; Fig. 1c) or the overall GvHD grade (P = 0.5244; Fig. 1d).
Time to response
The time to response by one stage of liver or intestinal GvHD could be analyzed in 24 of the 25 patients. In one patient (GvHD III; malignant underlying disease), the time to response was not clearly documented in the charts. The median time to response of the analyzed 24 patients was 24 days (range 12–1,050 days; Fig. 2a). The malignancy of the underlying disease had no statistically significant (P = 0.2153) impact on the time to response; patients with a malignant (n = 16) or nonmalignant (n = 9) underlying disease comprised a median time to response of 24 days (range 12–1,050 days) and 24 days (range 14–249 days), respectively (Fig. 2b). In the patients with GvHD III (n = 17), the time to response (median 23 days; range 12–1,050 days) was significantly shorter (P < 0.05), than in the patients with GvHD IV (n = 7; median 81 days; range 21–245 days; Fig. 2c).
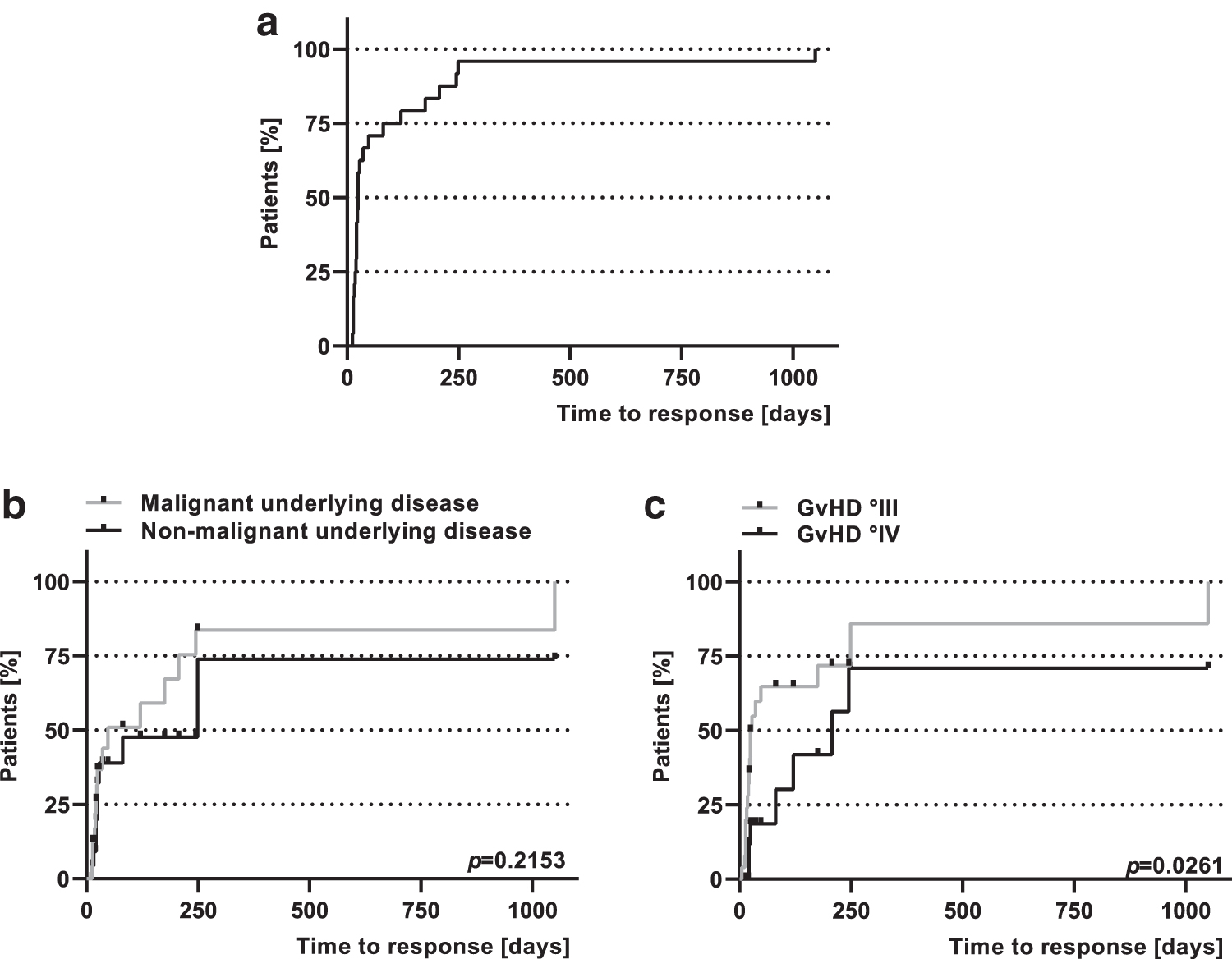
Time to response. The graph shows the time to response (improvement of the GvHD by one stage) of all analyzed patients
Safety and tolerance
None of the patients experienced acute MSC-related adverse reactions or side effects, including tachycardia, infusion-related reactions, respiratory distress, or hypertension. Moreover, in the long-term analysis up to 12.7 years after MSC infusion, no potentially MSC-related adverse effects were identified. The administration of this cell-based product was thus safe and free of detectable long-term adverse effects in this small cohort.
Treatment efficacy
All patients responded to the treatment with MSC for therapy- or steroid-refractory acute gut GvHD (Tables 2 and 3). Complete responses were seen in 6 patients (24.0%) and PRs in 19 patients (76.0%).
Among the patients with liver GvHD (n = 4), 1 patient had a CR (initially liver GvHD stage 4), while the other 3 patients had a median improvement by 1 stage (range 1–2 stages). Among the patients with intestinal GvHD [n = 25; 100.0%; median intestinal GvHD stage 3 (range 2–4)], 6 patients (24%) had a CR, and 19 (76%) had a PR after MSC application. A median improvement by one GvHD stage (range 1–4 stages) could be achieved in these patients.
Discussion
Chronic or acute steroid- or therapy-refractory GvHD is a life-threatening complication after alloHSCT, and it still poses a major treatment challenge [45]. This study reports the long-term follow-up up to 12.7 years after alloHSCT in 23 pediatric and 2 young adult patients with steroid- and therapy-refractory acute GvHD, who received MSC from their stem cell donor or a third-party donor for the treatment of GvHD.
Despite numerous side effects and limited efficacy, corticosteroids remain the key component of the first-line therapy of acute GvHD. However, in pediatric patients, a systemic steroid therapy can be harmful to the growing body, indicating that the avoidance or reduction of systemic steroids (eg, through the complementation of immunomodulatory agents that allow a reduction of corticosteroids or other therapy alternatives) is of great importance [46]. Furthermore, the long-term immunosuppression through the systemic use of steroids significantly increases the risk of life-threatening viral or invasive fungal infections [47,48].
In 2004, the use of MSCs in a pediatric patient with steroid-refractory acute intestinal GvHD was initially reported [27]. In the following years, several clinical and preclinical studies confirmed the immunosuppressive and anti-inflammatory properties of MSCs and their efficacy, especially for patients with steroid-refractory GvHD [12,35,49]. Acute MSC-related toxicity and side effects are generally low [35]. In a phase II/III study including adult patients with steroid-refractory grade III and IV GvHD, MSC infusion-related adverse reactions or the formation of ectopic tissue was not observed [50].
However, data on long-term safety and efficacy of this cell-based therapy option are missing, especially in pediatric patients.
In this study, 25 pediatric and young adult patients received a total of 65 MSC applications up to 4 years after HSCT for the treatment of acute and/or later for their cGvHD (n = 3; 12.0%). All patients responded with mainly PR (76% of the patients). CR was seen in 6 patients (24%) with GvHD III–IV. In contrast to earlier studies, the median observation period of the surviving patients in this analysis was 9.3 years (range 1.3–12.7 years) [15,29,51].
A recent study using expanded MSC from a pool of 8 donors presented data of 69 patients [51 pediatric (median age 8.2 years) and 18 adult (median age 45.5 years) patients] with refractory III–IV GvHD. The overall response rate was 83% within 28 days after MSC application and 86% in the follow-up analysis (median 8.1 months after MSC application) [15]. Transplant-related mortality in this study was 0% in the patients with CR and 26% in the patients with PR. In a phase II study with 37 pediatric patients who received parental MSC for steroid-refractory acute GvHD III–IV, transplant-related mortality in the patients with CR (59%) was 14% compared with a transplant-related mortality of 60% in the remaining patients [51].
Prospective data have been missing for a long time. In 2014, a prospective multicenter study was published, which included 75 pediatric patients with steroid-refractory acute GvHD II–IV also receiving MSCs from a pool of 7 donors. The treatment schedule was comprised of MSCs infused twice weekly for four consecutive weeks (eight infusions total). The overall response rate (PR and CR) was 61.3% within 28 days after MSC application. Patients with PR or CR had significantly higher survival rates by day 100 after HSCT compared with patients who did not respond to remestemcel-L therapy (78.1% vs. 31.0%; P < 0.001) [37].
One concern in the application of MSC has been malignant transformation. It is known for a long time that application of MSC is accompanied with little or no acute toxicity [16,26,52,53]. However, late effects have not yet been reported. Therefore, our study contributes information to the safety profile of MSCs in a relevant clinical setting by a long-term follow-up of up to 12.7 years. It is noteworthy that we did not find late, potentially MSC-related side effects in any of the patients. At present, there are no comparable data reporting long-term observations or evaluations of MSC applications in pediatric patients for the treatment of GvHD.
Conclusion
In this study, the treatment of acute steroid- or therapy-refractory GvHD of 25 pediatric and young adult patients with allogeneic MSC was safe and effective. In the long-term follow-up of up to 12.7 years after HSCT, in this limited cohort all patients responded at least partially to MSC. A survival rate of 60% and a transplant-related mortality of 24% were observed. MSC-related long-term side-effects were not observed in any of the patients. Larger, prospective, and randomized trials are needed to evaluate the long-term effects of MSCs and our findings.
Footnotes
Acknowledgments
This work was supported by the Madeleine Schickedanz-KinderKrebs-Stiftung, Fürth-Dambach, Germany and the Stiftung des Fördervereins für krebskranke Kinder Tübingen, Tübingen, Germany.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This work was financially supported by the Madeleine Schickedanz-KinderKrebs-Stiftung, Fürth-Dambach, Germany and the Stiftung des Fördervereins für krebskranke Kinder Tübingen, Tübingen, Germany.