
Abstract
Mesenchymal stem cell (MSC) therapy is considered one of the most promising treatments in the context of the coronavirus disease 2019 (COVID-19) pandemic. However, the safety and effectiveness of MSCs in the treatment of COVID-19-associated pneumonia patients need to be systematically reviewed and analyzed. Two independent researchers searched for relevant studies published between October 2019 and April 2021 in the PubMed, Embase, Cochrane Library, WAN FANG, and CNKI databases. All relevant randomized controlled trials, clinically controlled studies, retrospective studies, case reports, letters (with valid data), and case series were included in this meta-analysis. A fixed-effects model and 95% confidence interval (CI) were used to analyze the results. A total of 22 studies involving 371 patients were included in the present study. Allogeneic MSCs from umbilical cord, adipose tissue, menstrual blood, placental tissue, Wharton's jelly, or unreported sources were administered in 247 participants. Combined results revealed that MSC therapy significantly reduced the incidence of adverse events [AEs; odds ratio (OR) = 0.43, 95% CI = 0.22–0.84, P = 0.01] and mortality (OR = 0.17, 95% CI = 0.06–0.49, P < 0.01), and the difference compared with control group was statistically significant. No serious MSC treatment-related AEs were reported. Lung function, radiographic outcomes, and inflammation- and immunity-related biomarker levels all showed improving trends. Therefore, MSC therapy is an effective and safe method for the treatment of COVID-19-associated pneumonia and shows advantages in reducing AEs and mortality. However, a standard and effective MSC treatment program must be developed.
Introduction
Coronavirus disease 2019 (COVID-19), an infectious disease caused by novel severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has been sweeping the globe. According to data reported by the World Health Organization, as of June 13, 2021, 175,333,154 confirmed cases of COVID-19 have been documented in countries, areas, or territories worldwide, resulting in 3,793,230 deaths, and 2,655,782 new cases and 72,528 new deaths were reported in the past week [1]. COVID-19 has been associated with an intensive care unit (ICU) admission rate of 5% among proven cases of infection [2] and a high mortality rate for critically ill patients [3]. These unsetting numbers have prompted an urgent need for treatments that can resolve serious cases and prevent fatal consequences [4].
Based on preclinical and clinical studies, mesenchymal stem cells (MSCs) can regulate inflammation and remodeling processes and correct alveolar-capillary dysfunction; thus, MSCs are considered as a potential treatment for COVID-19 [5,6]. MSCs are multipotent cells and can be obtained from a variety of tissues, preferably bone marrow, adipose tissue, placental tissue, umbilical cord, and dental pulp [7 –12].
Notably, a controlled study by Leng et al. [13] showed that seven patients in the MSC treatment group were cured or the symptoms were significantly improved after 14 days of angiotensin-converting enzyme 2 (ACE2)-negative MSC injection, and inflammation and immune function levels were also ameliorated without observed adverse effects. The outcomes of three patients in the control group included one death, one case of acute respiratory distress syndrome (ARDS), and one remained in a severely condition. Therefore, the authors believed that intravenous transplantation of MSCs was safe and effective for the treatment of patients with COVID-19 pneumonia, especially critically severe patients. Fortunately, the application of MSCs in the treatment of COVID-19 has been well studied not only in terms of symptomatic efficacy but also in inflammation, immunity, and molecular mechanisms [14,15].
Therefore, this article conducted a systematic review and meta-analysis of the currently available literature on MSC treatment of COVID-19 since COVID-19 was first reported in 2019 to analyze its safety and efficacy and investigate the potential value of MSC therapy in patients with COVID-19.
Methods
Literature search
The systematic review was performed according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines [16]. The literature was searched with no language restrictions by two independent researchers. Since COVID-19 was first reported in Wuhan, China, and subsequently confirmed [17,18], we searched for articles published between October 2019 and April 2021 in PubMed, Embase, Cochrane Library, WAN FANG, and CNKI databases. The terms used for the search were as follows: “novel coronavirus” OR “2019 coronavirus disease” OR “novel coronavirus disease 2019” OR “2019-nCoV” OR “COVID-19” OR “SARS CoV-2” OR “severe acute respiratory syndrome-coronavirus-2” and “stem cell.” Articles from the same authors or institutions were examined, and duplicate data sets were excluded. The number of articles included and excluded was shown in a flow chart (Fig. 1).
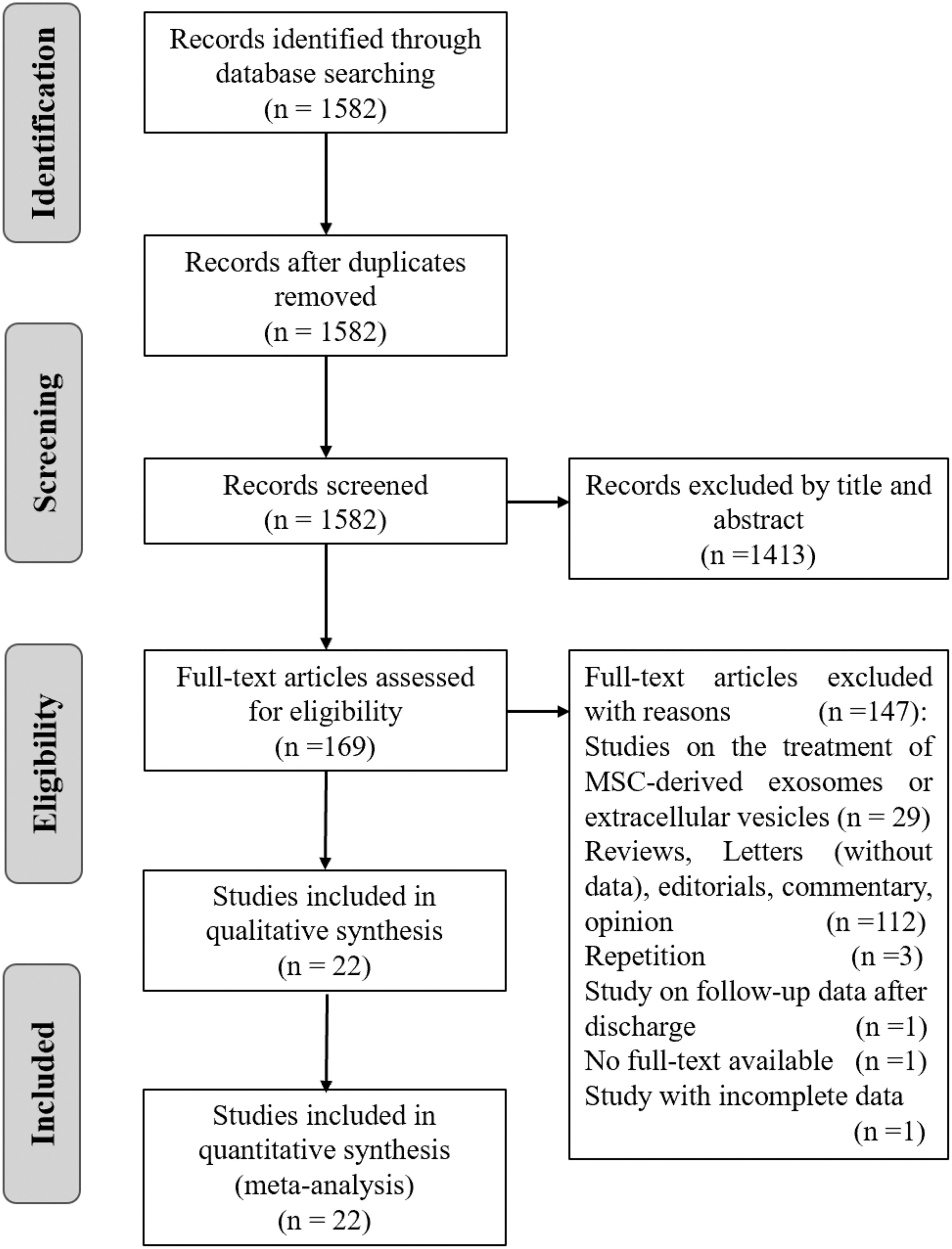
Flow chart. MSC, mesenchymal stem cell.
Eligibility criteria
We included randomized controlled trials (RCTs), clinically controlled trials (CCTs), retrospective studies, case reports, letters (with valid data), and case series evaluating the safety and/or efficacy of MSCs administered to adult patients diagnosed with COVID-19 pneumonia from any cause. Culture-expanded or minimally manipulated MSCs were included. Studies were excluded if they did not report original data (eg, reviews, editorials, letters, commentaries, opinions, guidelines, or errata).
Data extraction
The extracted data were as follows. Data in articles were extracted independently by two reviewers and verified by the third reviewer if a disagreement arose.
General data
General data are shown in Tables 1 –3 (author name, publication year, country, study design, number of cases, age, gender, and follow-up data are shown in Table 1; baseline disease severity, comorbidities, general conditions, and imaging outcomes are shown in Table 2; MSC sources, the gender and number of donors, surface markers, MSC dose per time, frequency, cell viability, and transplantation routes are shown in Table 3). Following established clinical guidelines for the diagnosis and treatment of COVID-19, disease severity was classified as mild, common, severe, or critical [19,20].
Study and Patient characteristics
CCT, clinically controlled trial; Ctrl, control group; MSC, mesenchymal stem cell; RCT, randomized controlled trial; NR, not reported.
Baseline General, Imaging Outcomes, and Disease Severity
AD, Alzheimer's disease; ARDS, acute respiratory distress syndrome; BA, bronchial asthma; CAD, coronary artery disease; CAF, chronic atrial fibrillation; CB, chronic bronchitis; CKD, chronic kidney failure; CLL, chronic lymphocytic leukemia; CMP, cardiomyopathy; COPD, chronic obstructive pulmonary disease; COVID-19, coronavirus disease 2019; CT, computed tomography; DM, diabetes mellitus; ECMO, extracorporeal membrane oxygenation; FLD, fatty liver disease; GGO, ground-glass opacity; HBV, hepatitis B virus; HD, heart disease; HT, hypertension; IQR, interquartile range; PaCO2, arterial blood partial pressure of CO2; PAD, peripheral artery disease; PaO2/FiO2, arterial blood partial pressure of oxygen/fraction of inspiration O2; SaO2, oxygen saturation.
Characteristics of Mesenchymal Stem Cells and Intervention Methods
AT, adipose tissue; IV, intravenous; MB, menstrual blood; PL, placenta; UC, umbilical cord; WJ, Wharton's jelly.
Outcomes
The primary outcome was safety based on the number of patients with adverse events (AEs), frequency of AEs, serious AEs (SAEs), and MSC treatment-related AEs. Clinical outcomes included general clinical symptoms (fever, cough, dyspnea, respiratory rate, etc.), blood oxygen indexes [arterial partial pressure of oxygen (PaO2), the fraction of inspired O2 (FiO2), PaO2/FiO2, arterial or peripheral oxygen saturation (SaO2 or SpO2, respectively), etc.], six- or seven-category scale scores, the time from intervention to recovery, and mortality. Radiographic outcomes included findings on lung computed tomography (CT) scans or chest X-ray imaging.
Laboratory outcomes included the time until nucleic acid became negative, immune cell levels [dendritic cells (DCs), lymphocytes (LYMs), natural killer cells (NK cells), T cells, B cells, neutrophils (NEs), and white blood cells (WBCs)], and inflammatory cytokines [alanine aminotransferase (ALT), ammonia, aspartate transaminase (AST), bilirubin, blood creatinine, B-type natriuretic peptide, blood urea nitrogen], creatine kinase (CK), CK-MB, C-reactive protein (CRP), cardiac troponin T, D-dimer, ferritin, fibrinogen, granulocyte-macrophage colony-stimulating factor (GM-CSF), interferon-γ (INF-γ or IFN-γ), IFN-g, interleukin (IL)-1RA, IL-2, IL-4, IL-5, IL-6, IL-7, IL-8, IL-10, IL-18, IL-22, interferon-inducible protein-10 (IP-10), lactate, lactate dehydrogenase (LDH), monocyte chemotactic protein-1 (MCP-1), macrophage inflammatory protein-1α (MIP-1α), myoglobin, procalcitonin, platelet-derived growth factor-BB (PDGF-BB), regulated upon activation normal T cell expressed and secreted factor (RANTES), tumor necrosis factor-α (TNF-α), TNF-β, triglyceride, and vascular endothelial growth factor.
Quality assessment
The methodological quality of each study included in the present meta-analysis was evaluated by the National Heart, Lung, and Blood Institute (NHLBI) quality assessment tools (Supplementary Table S1) [21]. All studies were classified as either good, fair, or poor.
Statistical analysis
Data are presented as n (%) for categorical variables and as the mean ± standard deviation for continuous variables. Mortality and the number of patients with AEs were the only two outcomes considered appropriate for a meta-analysis. The Review Manager v.5.3 software was used to merge in each study, and overall estimates of effects were shown in the form of forest plot. We used I 2 indicator to evaluate heterogeneity between studies. Sensitivity analysis was performed by eliminating one included study at a time, and subgroup analysis was performed to examine the source of the heterogeneity when heterogeneity existed (I 2 > 50%). A random-effects model was used if heterogeneity still existed. Otherwise, a fixed-effects model was used (I 2 < 50%). The final selected model was used to summarize the odds ratios (ORs) of the included studies. We were unable to evaluate publication bias due to the small number of available studies.
Results
The literature search identified 1,582 unique citations. Abstract and full-text screening identified 22 studies with 371 patients to be included for the data extraction. All included studies were assessed as good [10,12,22 –31] or fair [13,32 –40] according to the NHLBI quality assessment tool (Supplementary Table S2).
Study characteristics
The 22 selected studies [10,12,13,22 –40] included 4 CCTs, 3 RCTs, 4 case series, 3 letters, and 8 case reports, 7 of which were comparative studies with control groups. All 22 studies reported mortality and laboratory outcomes (n = 371); 17 studies reported AEs and SAEs (n = 273); and 20 studies reported general clinical symptoms and imaging outcomes after MSC treatment (n = 324). A total of 247 patients received MSC therapy, while 124 patients participated as controls (Table 1).
Patient characteristics
The 22 studies were from 7 countries and regions, including China (n = 14) [12,13,22 –25,28 –31,34 –36,40], the United States (n = 1) [26], Germany (n = 1) [32], Spain (n = 2) [33,39], Iran (n = 1) [10], Mexico (n = 1) [27], and Turkey (n = 2) [37,38]. Eleven studies reported on baseline oxygenation indicators [10,13,26 –28,30,32,34,35,39,40]. General symptoms such as fever, cough, and dyspnea were reported in 16 studies [10,12,13,23,24,27 –32,34,37 –40], and lung imaging evaluation showed COVID-19-related pneumonia in 15 studies [10,12,23,25,27 –32,34,37 –40]. Disease severity was critical (n = 63), severe (n = 260), and moderate (n = 10) in 19 studies [10,12,13,22 –25,27,29 –38,40] and the patients in one study were divided into mild-to-moderate (n = 6) and moderate-to-severe (n = 18) groups according to the severity of ARDS [26].
The average ages of study participants were 45.1 to 61.0 years for the MSC group and 39.0 to 65.0 years for the control group in the comparative studies [13,22 –26,32]. In the comparative studies, disease severity in the MSC group was critical (n = 13), severe (n = 115), and moderate (n = 8), whereas that in the control group was critical (n = 11), severe (n = 105), and moderate (n = 8) [13,22 –26,32]. The most common comorbidities, including hypertension (n = 105), diabetes mellitus (n = 61), obesity (n = 19), chronic obstructive pulmonary disease (n = 11), and heart disease (n = 9), were reported in 18 studies [10,12,13,22,23,25 –28,30 –35,37,38,40]. Differences in the follow-up time after MSC treatment were also identified in these studies, with follow-up times ranging from 1 week to 2 months, which was mainly due to the times when patients recovered and were discharged from the hospital or when patients died (Tables 1 and 2).
Intervention method
Culture-expanded allogeneic MSCs were used in all 22 included studies. Allogeneic umbilical cord-derived MSCs were used in 12 studies [22,23,25,26,27,29 –31,34,35,38,39], Wharton's jelly-derived MSCs in 3 studies [12,37,40], menstrual blood-derived MSCs were used in 2 studies [24,28], and adipose tissue- or placenta-derived MSCs were separately used in 1 study [10,33]. Four studies did not report the tissue origin of the MSCs [13,32,36,39] (Table 3). Characterization was reported in most studies, with significant differences in details. Characterization of MSCs was reported in 11 studies, including most of the following markers: positivity for CD9, CD29, CD44, CD73, CD90, CD105, and HLA-ABC, and negativity for CD11b, CD14, CD19, CD31, CD34, CD45, CD79α, CD133, and HLA-DR [10,12,13,22 –28,31]. Viability was reported to be >80% [10,12,24 –29,31,32].
MSCs were mainly injected intravenously (n = 245), and two other patients were injected intratracheally and intravenously [37,38]. MSC infusion frequencies ranged from a single infusion to five infusions (n = 47, 43, 154, 2, 1). MSC dosing ranged from 1 to 2 million cells per kilogram of body weight, or a uniform dose of 30 to 200 million cells was administered. Only one study did not report the dose [37].
Safety
Adverse events
We extracted data from 16 studies on the number of AEs and the number of patients with AEs to describe the occurrence of AEs (Table 4) [10,12,13,22,24 –26,27,29 –31,33,36 –39]. In the MSC group, 48.33% (87/180) of patients have appeared AEs, and the total number of AEs was 167. Additionally, according to research by Feng et al., hypoalbuminemia, insomnia, gastrointestinal diseases, and paroxysmal arrhythmia occurred in the surviving patients [35].
Adverse Events and Mortality
AEs, adverse events; SAEs, serious adverse events.
Notably, 15 treatment-related AEs were reported in 5 studies. Meng et al. reported that two patients receiving MSCs developed transient facial flushing and fever immediately upon infusion, which resolved spontaneously within 4 h; another moderately ill patient developed transient fever within 2 h that resolved within 24 h [22]. Chen et al. reported that three patients experienced treatment-related AEs, specifically liver dysfunction, heart failure, and allergic rash [36]. Hashemian et al. reported that two patients developed shivering during the initial MSC infusion, which was relieved by supportive treatment in <1 h [10]. Iglesias et al. reported that one patient had muscle contractions in the extremities; another patient had muscle contractions in the extremities and chest, PO2 decreased to 78%, arterial hypertension, and compromised respiratory effort; and the third patient developed hypotension [27]. In the study of Lanzoni et al., a treatment-related AE was reported without specific description [26].
AE incidence rates between MSC group and control group were compared in five studies (n = 196) [13,22,24 –26]. The overall AE incidence rates were 58.0% (69/119) for MSC-treated patients and 77.9% (60 of 77) for controls, and the difference was statistically significant [OR = 0.43, 95% confidence interval (CI) = 0.22–0.84, P = 0.01] (Fig. 2).

Pooled estimate for the number of adverse events. Ctrl, control.
Serious AEs
In our data extraction process, the number of deaths was included in the number of SAEs if the study did not describe SAEs in detail and only reported mortality. The results showed that 32 SAEs occurred in 219 MSC-treated patients in 19 studies (Table 4) [10,12,13,22 –27,29 –35,37 –39]. No MSC treatment-related SAEs were reported.
The 10 SAEs reported in Xu et al.'s study included severe liver dysfunction (n = 1), expiratory dyspnea (n = 1), respiratory failure (n = 1), ARDS (n = 1), shock (n = 3), multifunctional organ failure (n = 2), and gastrointestinal bleeding (n = 1) [24]. Shi et al. reported one case of pneumothorax in the MSC group, and the patient recovered naturally after conservative treatment [25]. Lanzoni et al. reported four SAEs without detailed descriptions [26]. Häberle et al. reported a case of death due to multiple organ failure [32]. Sánchez-Guijo et al. reported that two patients died: one patient died from massive gastrointestinal bleeding, and the other patient died of secondary fungal pneumonia caused by Saccharomyces spp. [33]. Guo et al. reported four patients died without detailed descriptions [34]. Two SAEs occurred during the trial reported by Feng et al. [35]. The two patients suffered from bacterial pneumonia and septic shock and died of multiple organ failure or circulation and respiratory failure, respectively. Hashemian et al. reported the deaths of four patients due to multiple organ failure, and one patient died due to cardiac arrest [10]. Iglesias et al. reported that a patient developed left lower extremity arterial thrombosis, hemodynamic deterioration, D-dimer concentration of 7,268 ng/mL, and death; Enterobacter cloacae were cultured in aspirated samples from the patient's trachea. Another patient developed hemodynamic alterations, epistaxis, and hematuria, and died 13 days after MSC infusion [27]. In the case report of Yilmaz et al., a patient was diagnosed with upper gastrointestinal bleeding, but the patient's vital signs were stable after effective treatment [37]. Among the 7 controlled studies, 136 patients in the MSC group had 16 SAEs, while 124 patients in the control group had 49 SAEs [13,22 –26,32].
Efficacy
Mortality
Mortality was reported in all included studies (Table 4), and the overall mortality rate was 12.94% (48/371). The mortality rate among MSC-treated patients was 8.50% (21/247). Comparisons between the MSC group and the control group were made in seven studies (n = 260), and there was a trend toward a decreased mortality rate noted in the MSC group in all seven studies [13,22 –26,32]. The overall mortality rates were 3.68% (5/137) for MSC-treated patients and 21.77% (27/124) for controls. There was a favorable trend observed, and the difference was statistically significant (OR = 0.17, 95% CI = 0.06–0.49, P < 0.01). However, the certainty of the evidence for the impact on mortality was limited due to differences in the baseline conditions of the included patients and the imprecision and methodological limitations of the included trials (Fig. 3 and Tables 1 and 2).
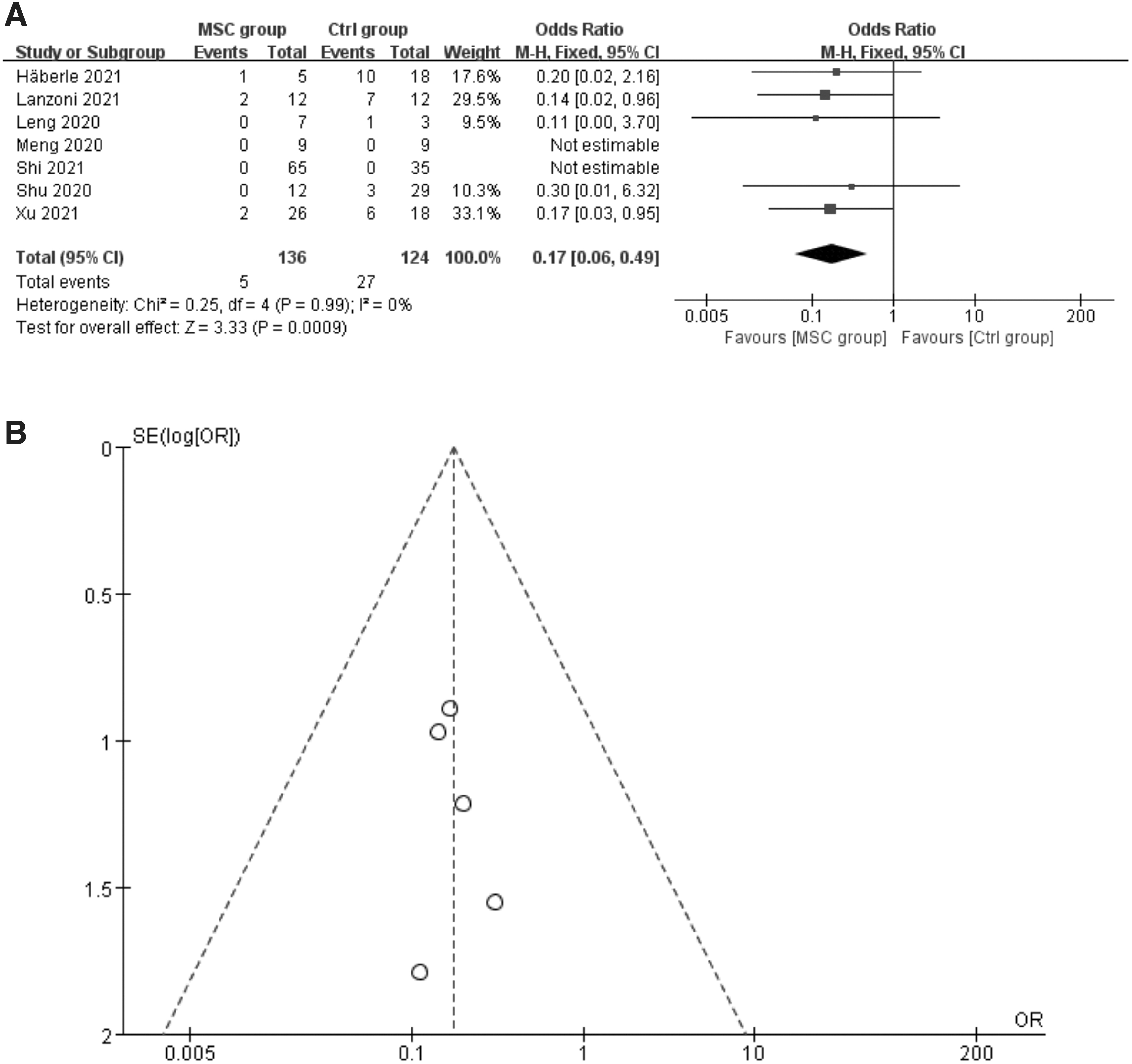
Pooled estimate for mortality.
Changes in general clinical symptoms and lung function
The results showed that the average time from the first injection to recovery or discharge from the hospital ranged from ∼2 to 24 days for MSC-treated patients (Table 5) [10,12,13,22 –24,26,27,29 –31,33,39,40]. In several controlled studies, Shu et al., Xu et al., and Lanzoni et al. reported that the average time required to improve (or recover) in the MSC group was shorter than that in the control group, and the difference was statistically significant [23,24,26]. However, Meng et al. reported that the time from admission to discharge was similar between the two groups [22]; and Xu et al. reported no significant difference in either the length of hospital stay or the number of days in the ICU between the two groups [24].
Clinical Symptoms and Imaging Outcomes
Day: Time starts from the first injection of MSC.
6-MWT, the 6-minute walk test; CI, confidence interval; ICU, intensive care unit; SpO2, peripheral oxygen saturation.
Changes in general clinical symptoms and pulmonary function (including the oxygenation index and chest radiology examinations) after treatment were recorded in 21 studies (Table 5) [10,12,13,22 –25,27 –40]. Different studies used different assessment indicators for lung function, which complicated the extraction of the outcomes. General clinical symptoms and pulmonary function (such as SaO2, PaO2/FiO2, the oxygenation index, and chest CT or X-ray) were found to improve in the early days after MSC treatment in most studies. Some studies reported that the MSC group showed a significant clinical improvement compared with the control group, and the oxygenation index in the MSC group recovered to the normal range faster than that in the control group [23,25,32]. Additionally, some indicators (including CT scores, the number of lobes involved, ground-glass opacity, and consolidation, etc.) reflecting the lung inflammation were significantly better in the MSC group than that in the control group [22 –25].
However, a study reported that cough showed significant improvement in the MSC group compared with the control group at day 1 after MSC treatment, but no difference was found at other time points; the expiratory dyspnea showed significant improvement in the MSC group compared with the control group at days 1, 3, and 5, but no difference was found at days 7, 14, and 30 [25]. Another study reported that pulse oxygen saturation significantly improved in survivors compared with nonsurvivors, even though all patients received MSC treatment [10].
Laboratory outcomes
The laboratory outcomes are shown in Table 6. The negative status of HCoV-19 nucleic acid was evaluated in 11 studies [12,13,22,24,26,28 –31,34,39]. The average time from the first injection to a negative nucleic acid test ranged from ∼4 to 15.8 days for MSC-treated patients. Comparisons between the MSC group and the control group were made in two studies, and no significant difference was found between the two groups [24,26].
Laboratory Outcome
Day: Time starts from the first injection of MSC.
ALT, alanine aminotransferase; AST, aspartate transaminase; BNP, B-type natriuretic peptide; BUN, blood urea nitrogen; CK, creatine kinase; CK-MB, creatine kinase-MB; CRP, C-reactive protein; cTnT, cardiac troponin T; DCs, dendritic cells; GM-CSF, granulocyte/macrophage colony-stimulating factor; IFN-g, interferon-g; IL, interleukin; INF-γ or IFN-γ, interferon-γ; IP-10, interferon-inducible protein-10; LAC, lactate; LDH, lactate dehydrogenase; LYMs, lymphocytes; MCP-1, monocyte chemotactic protein-1; MIP-1α, macrophage inflammatory protein-1α; NEs, neutrophils; NK, natural killer; PCR, polymerase chain reaction; PCT, procalcitonin; PDGF-BB, platelet-derived growth factor-BB; RANTES, regulated upon activation normal T cell expressed and secreted factor; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TNF, tumor necrosis factor; VEGF, vascular endothelial growth factor; WBCs, white blood cells.
Immune cells were tested in 15 studies [12,13,23,25,27 –35,37,40]. Increases in DCs, LYMs, NK cells, T cells, and B cells, and the decrease of NEs and WBCs were found in most of the studies. However, Guo et al. reported that there was no significant difference in WBCs before and after MSC treatment [34], and Iglesias et al. reported that only one patient (1/5) had a decrease in total LYMs from 1,570 to 984/mL at 7 days postinfusion [27]. In the controlled studies, significant reductions in WBCs and NEs and a significant increase in LYMs were found in the MSC group compared with the control group [23,32]. However, one study reported no significant difference in subsets of peripheral LYM counts (CD4+ T cells, CD8+ T cells, B cells, NK cells) between the two groups at days 0, 6, 10, and 14 after the first MSC injection [25].
Inflammatory cytokines were evaluated in all studies. Most studies found that serum cytokines, chemokines, and growth factors improve to varying degrees following MSC therapy. Two controlled studies reported that the concentrations of CRP, GM-CSF, IFN-g, IL-5, IL-6, IL-7, TNF-α, TNF-β, PDGF-BB, and RANTES in the MSC group were significantly lower than those in the control group [23,26]. However, we also noticed no significant difference in plasma markers (IL-6, IL-8, IFN-γ, IL-1Ra, IL-18, MCP-1, MIP-1α, and IP-10) between the two groups reported in the two controlled studies [25,32].
Discussion
Specific vaccines against the SARS-CoV-2 virus have been produced and promoted. In mainland China, people are being vaccinated for free in a planned manner, and nearly 1.1 billion doses of SARS-CoV-2 vaccines have been administered as of June 23, 2021 [41]. However, the shortage of vaccines, vaccine-related AEs, and virus variants have kept some countries and regions in the shadow of the raging COVID-19 epidemic [42 –46]. Therefore, other active treatments are still essential. At present, a considerable number of studies have analyzed the possibility of MSCs for the treatment of COVID-19, and some clinical trial results have confirmed their effectiveness. Therefore, this meta-analysis reviewed published results of MSC treatment of COVID-19 patients with a focus on safety, efficacy, and related pulmonary and immunologic responses. Our analysis of relevant studies found that MSC therapy is safe and shows the potential to mitigate immunity- and inflammation-related damage to the lungs and other organs and decrease the mortality of COVID-19 patients.
Safety
Safety is the primary concern for any new therapies, especially in patients at a high risk of death due to treatment, and was carefully assessed in MSC-treated patients in the reviewed studies. This study analyzed the occurrence of AEs and found that the MSC group had fewer patients with AEs than the control group in five controlled studies [13,22,24 –26], and the difference was statistically significant. Fifteen transient AEs related to MSC treatment were reported [10,22,26,27,36], most of which resolved spontaneously in a short time. Regrettably, 32 SAEs occurred in the 219 MSC-treated patients, but the authors of these studies believed that none of these SAEs was related to MSC therapy [10,12,13,22 –27,29 –35,37 –39]. Additionally, the number of SAEs in the MSC group was also lower than that in the control group in the controlled studies [13,22 –26,32]. The safety observed is consistent with observations in other human clinical trials involving MSC treatment [47,48].
The primary outcome used to analyze the potential efficacy of MSC therapy in this study was the mortality of patients with COVID-19. A systematic review of human ARDS from the Qu et al. believes that cell-based treatment may reduce COVID-19 mortality [49]. The present study found that all seven controlled studies reported that the MSC group had reduced mortality [13,22 –26,32], and the pooled estimates of mortality showed that the mortality rate of the MSC group was significantly lower compared with the control group (3.68% vs. 21.77%). The difference suggests that MSC treatment may be effective in reducing the mortality of these patients.
COVID-19 is characterized by notable hematological manifestations, thrombocytopenia, and coagulation abnormalities on presentation and is associated with poor outcomes during the disease courses [50]. A study reported that despite low-molecular-weight heparin prophylaxis or full anticoagulant therapy, the incidence of deep vein thrombosis, mainly asymptomatic, in hospitalized COVID-19 patients was 14.5% [51]. However, some patients had to discontinue anticoagulation therapy due to bleeding or anemia and eventually died of hemodynamic disorders [27]. Notably, 10 patients were already in very serious condition before receiving MSC treatment and died of multiple organ failure or hemodynamic disorders [10,27,32,35,39]. Although their condition improved within a few days after MSC transplantation, this sympathetic treatment failed to save their lives. Therefore, the authors of the present study considered that although MSC treatment may play a positive role in most COVID-19 patients and help save their lives, there are still individual differences in its efficacy.
Efficacy
The results of three studies showed that the average time of improvement (or recovery) in the MSC group was significantly shorter than that in the control group [23,24,26], while two studies showed that the length of hospital stay was not different between the two groups [22,24]. The authors of the present study believe that the reason for this difference is that the time from symptom onset to COVID-19 diagnosis or hospitalization differed in these studies. Therefore, the difference in the length of hospital stay between these studies is not considered statistically significant because of the small number of included cases and a lack of uniform admission criteria.
Hashemian et al. reported that nonsurvivors' pulse oxygen saturation did not show the same improvement as that of survivors even though all patients received MSC treatment [10]. A case report showed that the patient's consciousness and mental state began to improve after MSC treatment, and the patient's pulmonary compliance increased significantly, but extracorporeal membrane oxygenation and mechanical ventilation could not be discontinued because no significant improvement in lung function and chest CT scans was identified. The treatment results were not satisfactory even after receiving five MSC injections, and the patient was fortunate to receive a lung transplant but regrettably died of transplant rejection [40].
However, general clinical symptoms, pulmonary function, and radiographic imaging were found to be improved in the early days after MSC treatment in most included studies, and the improvement in the MSC group was significantly better than that in the control group. Intravenously infused MSCs have been found to migrate directly to the lung, where they can secrete a variety of factors with important roles in immune regulation, protection of alveolar epithelial cells, resistance to pulmonary fibrosis, and improvement of lung function. MSCs show considerable benefits for the treatment of severe lung diseases in COVID-19 [52,53]. The findings of this study also further support the use of MSCs to treat COVID-19-related pulmonary function decline.
The interaction between viral infection and the immune system determines the occurrence and development of SARS-CoV-2. Previous studies have shown that dysregulation of the immune system, including lymphopenia and cytokine storms, may be key factors related to disease severity in COVID-19 patients [49,54]. Moreover, Chen et al. found that the absolute numbers of T cells, CD4+ T cells, and CD8+ T cells in almost all patients decreased, and the numbers in severe cases were significantly lower than those in moderate cases. Additionally, severe cases are more prone to the development of dyspnea, lymphopenia, and hypoalbuminemia, with higher levels of ALT, LDH, CRP, ferritin, and D-dimer, than moderate COVID-19 cases [20]. In severe cases, patients with COVID-19 pneumonia may progress to ARDS due to elevated levels of inflammatory cytokines. Therefore, some scholars believe that the best strategy to treat COVID-19 pneumonia probably involves reconciling the strong inflammatory response of the host immune system and regeneration of impaired cells [55].
Previous studies demonstrated that the secretion of multiple functional factors of MSCs, such as cytokines, chemokines, angiogenic factors, growth factors, exosomes, and extracellular vesicles, is the main mechanism of these cells' therapeutic effect. These multiple functional mechanisms render MSCs suitable for the treatment of complex and multifactorial diseases for which no other confirmed drug treatments are available, such as COVID-19-related pneumonia and other inflammatory diseases involving cytokine storms [14,56,57]. The present study found that MSC therapy has a positive impact on the immune and inflammatory processes that lead to organ damage in COVID-19 patients. Most of the included studies showed that the number of immune cells improved and serum inflammatory factors gradually abated with MSC treatment. Additionally, patients' WBC counts returned to the normal range before MSC injection, resulting in no significant difference before and after MSC treatment in Guo's study [34].
Other findings
Hoffmann et al. demonstrated that SARS-CoV-2 uses the SARS-CoV receptor ACE2 to enter cells, and the virus uses host cell transmembrane serine protease II (TMPRSS2) to initiate spike envelope protein [58]. ACE2 and TMPRSS2 exist on the surfaces of various human cells, including alveolar cells and capillary endothelial cells, while studies reported that human MSCs express neither ACE2 nor TMPRSS2, and human MSCs derived from fetal and adult tissues are not allowed to be infected with SARS-CoV-2 [13,59,60]. These research results further allow MSC therapy to gain the attention of more professionals combating COVID-19 pneumonia.
We also found that the three most common comorbidities were hypertension, diabetes mellitus, and obesity, which is consistent with the concerns of many previous authors [61 –64]. Because diabetes mellitus has a chronic course, some elderly hypertension patients require treatment with ACE inhibitors, which may increase ACE2 expression. In addition, pioglitazone and liraglutide, which are used to control blood glucose levels, have been found to upregulate ACE2 expression in experimental models [65 –67]. Previous studies also confirmed that comorbidities such as hypertension, diabetes, and obesity are risk factors for severe symptoms and increased mortality in COVID-19 patients [61 –65,68].
Research significance
This comprehensive systematic review and meta-analysis of published reports on MSC therapy for COVID-19 have yielded several important findings. Primarily, the number of patients with AEs in the MSC group was significantly lower than that in the control group, and the mortality rate was also significantly reduced (3.68% vs. 21.77%). Only 36 SAEs occurred in 219 patients treated with MSCs, none of which was related to MSC transplantation. Additionally, MSC therapy plays an active role in restoring lung function and improving symptoms. Furthermore, MSC therapy is beneficial for managing cytokine storms and correcting immune disorders. This study provides a sympathetic treatment option for doctors and patients in areas still under the shadow of the COVID-19 outbreak and summarizes experiences that may help when addressing new challenges in the future.
Limitations
Although we did our best to include all clinical reports on MSCs for the treatment of COVID-19-related pneumonia in this systematic review, toward the end of the project, targeted studies remain limited, and the included studies did not have a standardized treatment plan and evaluation criteria for MSCs. Therefore, large-scale RCTs are urgently needed. Moreover, selection bias may exist, and the description of the evaluation in published results may be insufficient.
Conclusion
This systematic review and meta-analysis of existing studies demonstrated the safety and effectiveness of MSCs in the treatment of COVID-19-related pneumonia. Adequately powered clinical trials are urgently needed to test the clinical results of MSC therapy in patients with COVID-19 and SARS-CoV-2 infection and to explore a standard MSC therapy program.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Jiangsu Provincial Medical Youth Talent [Grant No. QNRC2016342]; Project on Maternal and Child Health Talents of Jiangsu Province [Grant No. F201801]; and Six Talent Peaks Project in Jiangsu Province [Grant No. LGY2019035]. No benefits in any form have been or will be received from a commercial party related directly or indirectly to the subject of this article.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.