
Abstract
Most pediatric patients with global developmental delay (GDD) or intellectual disability (ID) have disrupted development. Since allogeneic umbilical cord blood (UCB) may exert neurotrophic effects, a prospective clinical trial was conducted to assess the efficacy and safety of UCB therapy for GDD and ID. A total of 13 children (ages 23–149 months) with GDD and ID were enrolled and followed up for 12 months. Under criteria of histocompatibility and cell number, allogeneic UCB units were selected and infused once intravenously, and adverse events were monitored. The Bayley Scale of Infant Development-II (BSID-II) was used as primary outcome measurement tool, and evaluations for various functional abilities were also implemented. Safety assessment did not reveal significant adverse effects. Functional improvements in mental and motor developments along with daily living activities and languages were observed at 12 months postintervention compared with the baseline abilities (P < 0.05). Furthermore, mental developmental quotient derived from BSID-II mental scale revealed significantly facilitated improvement during the first 3 months (P < 0.05). In the survey conducted 80.7 ± 13.0 months after UCB infusion to assess satisfaction and long-term safety, no long-term adverse effects were reported, and 70% of the guardians reported satisfaction with the UCB infusion. Long-term changes in two patients who were regularly followed up beyond the study completion were noticeable. One case observed for 4 years showed dramatic improvement until 12 months after UCB therapy, whereas she showed insignificant improvement beyond 12 months after the therapy. Another case showed alleviation of autism with findings of anti-inflammatory response in his peripheral blood after UCB infusion. This clinical study provides support for further applications of UCB as a therapeutic avenue for children with GDD or ID owing to its safety and partial efficacy. Due to patient heterogeneity, further studies focusing on specific clinical manifestations and etiologies are required.
Registered at
Introduction
Global developmental delay (GDD) can be defined as significant delay in two or more developmental domains that include gross/fine motor, speech/language, cognition, social/personal behavior, and activities of daily living among those younger than 5 years of age [1]. As the children grow older than 5 years, they usually present features of intellectual disability (ID) [1 –3], defined as a significant delay in cognitive development accompanying impaired adaptive ability [1,4]. In a 2-year follow-up cohort study, the improvement was minimal in children with GDD [5].
Autism spectrum disorder (ASD) is usually associated with GDD [6]. Recent research has suggested that neuroinflammatory mechanisms may be involved in pathogenesis of ID and ASD [7,8]. So far, treatments of children with ID and GDD are merely educational and psychosocial supports for gaining and maintaining function [3].
Umbilical cord blood (UCB) has emerged as a new source of cell therapy and has been proven to be effective in neurological disorders [9 –11]. Although its full mechanism is yet to be completely understood, several studies reported neuroprotective effects of UCB [12]. Various clinical trials have been reported on use of UCB in children with cerebral palsy and ASD, where its safety and efficacy have been supported [13 –15]. Since most children do not possess their own autologous UCB, although it would be the first choice for clinical trial, allogeneic UCB could be considered as an alternative option. Prior reports have shown beneficial effects of allogeneic UCB for neurological conditions [16,17].
We hypothesized that intravenous infusions of allogeneic UCB could be a safe therapeutic avenue for children with GDD and ID. We conducted this prospective pilot study to determine the efficacy and safety of allogeneic UCB therapy in children with GDD and ID and the long-term effects were assessed afterward.
Materials and Methods
Patients
Patients between 6 months and 15 years of age who met the criteria for diagnosis of GDD or ID were enrolled from January 2013 to September 2016. GDD was diagnosed with delays in two or more developmental domains with criteria of under two standard deviations in standardized measurements [1]; Bayley Scales of Infant Development-II (BSID-II) [18], Sequenced Language Scale for Infants (SELSI) [19], Preschool Receptive–Expressive Language Scale (PRES) [20], Receptive and Expressive Vocabulary Test (REVT) [21] for speech/language, Beery-Buktenica developmental test of visual–motor integration (Beery VMI) [22], Child Behavior Checklist (CBCL) [23], and Pediatric Evaluation of Disability Inventory (PEDI) [24]. ID was diagnosed with findings of significant delay in cognition and concomitant delayed acquisition of daily living activity skills, according to quotient score of Wechsler's Intelligence Scales [25,26] or München Functional Developmental Diagnostics (MFED) [27]. Childhood Autism Rating Scale (CARS) [28] or Modified Checklist for Autism in Toddlers (M-CHAT) [29] was also performed for screening autistic features.
Children with ASD were included if they met the GDD and ID criteria. The exclusion criteria were the presence of pneumonia, previous hypersensitivity reactions to the medications being studied, renal impairments, and intractable epilepsy. As diagnostic measures, brain magnetic resonance imaging (MRI) and gene studies, including high-resolution chromosome analysis and multiplex ligation-dependent probe amplification were performed. Parents or legal representatives provided written informed consent to participate in the study. The protocol of this prospective pilot study was approved by the Institutional Review Board of CHA Bundang Medical Center (2012-11-159).
Intervention protocol
Allogeneic UCB units were selected from the affiliated CHA Cord Blood Bank. The conditions for unrelated allogeneic UCB unit selection were ≥3 × 107/kg total nucleated cells (TNC) and at least four out of six matches for HLA-A, -B, and -DRB1 antigens in high resolution. After washing the UCB to remove dimethyl sulfoxide according to the institutional protocol [30], UCB cells were infused once intravenously by the principal investigator. For patients who had difficulty in enduring the procedure, the infusion was performed under sedation.
Cyclosporine at a dose of 7 mg/kg was orally administered twice daily, from 3 days before to 13 days after the UCB infusion, and the target cyclosporine range was determined as 50–350 ng/mL

The timeline of the study.
Safety measurements during the study period
All adverse events (AEs) were actively monitored and recorded for 1 year according to common terminology criteria for AEs (CTCAE). Laboratory studies, including complete blood count, liver enzymes, renal function tests, C-reactive protein, and urine analysis were conducted before UCB infusion, and 5 and 14 days after UCB infusion. Cyclosporine levels were measured at baseline and at 5 and 8 days after the infusion.
Functional assessments
Various assessment tools were used to evaluate functional changes. These include the BSID-II, gross motor functional measure (GMFM) [34], Wee functional independent measure (WeeFIM) [35], PEDI, Beery VMI, and speech/language tools, including SELSI, PRES, or REVT. Intelligence ability was measured with Wechsler Preschool and Primary Scale of Intelligence (WPPSI) [26] or Wechsler Intelligence Scale for Children (WISC) [25] depending on age, and the outcomes were expressed as intelligence quotient (IQ). When the Wechsler's scales were not available due to age or low cognitive ability, an estimated IQ was derived from MFED. In addition, CARS or M-CHAT was followed up in patients with autistic features. Functional measurements were conducted at baseline, and at 3, 6, and 12 months after baseline assessment. Psychological and language assessments were followed at 6 and 12 months to minimize learning effects
Developmental quotient use
Developmental quotient was derived using the developmental age estimated by BSID-II for children with ≤42 months of developmental acquisition. The calculation formula was developmental age (months)/chronological age (months) × 100 (%). This quotient was applied to the mental and motor scales of the BSID-II.
Survey of satisfaction and long-term safety
Telephonic surveys were conducted from July to October 2020 to investigate family satisfaction and long-term safety of UCB therapy. Medical doctors not participating in the trial performed the process.
Questions were: (1) Are you satisfied with the overall effect of UCB therapy? (2) If you have a chance, would you go through UCB therapy again? (3) According to your experience, would you recommend UCB therapy to other patients? Each item was rated on a five-point Likert scale [39], where five refers to strongly agree, and one to strongly disagree. Additional question was also asked if there had been any significant adverse events after the therapy.
Assessment of metabolic changes in the brain after UCB therapy
18F-fluorodeoxyglucose positron emission tomography/computed tomography (FDG-PET/CT) images were acquired using a Biograph mCT PET/CT scanner (Siemens Healthcare, USA) at baseline and 12 months after the intervention. Each patient's preprocedural PET image was compared with 1-year follow-up PET image at every pixel, using a paired t-test to detect any regional increase in metabolism. The threshold was set to P < 0.001 corrected for multiple comparisons with the family-wise error method. Spatial preprocessing and statistical analyses were performed using SPM 12 software (University College London, United Kingdom) within MATLAB R2019b (The MathWorks Inc., USA).
Cytokine analysis
Blood samples were collected before UCB infusion (D-1) and after the infusion (D + 1, D + 5, D + 8, and D + 14). Reverse transcription–polymerase chain reaction (RT-PCR) was used to measure mRNA expression of tumor necrosis factor (TNF)-α and interleukin (IL)-1β levels using ReverTra Ace® qPCR RT Master Mix (Toyobo Co., Japan). After performing three rounds of RT-PCR, the mean value was calculated and used for analysis.
Comparison of functional assessment changes after UCB therapy
For 10 patients whose developmental quotient could be confirmed, functional assessments, including developmental quotient after UCB therapy were analyzed between groups divided by age before and after 60 months and by gender, respectively.
Statistical analyses
Statistical analyses were performed using the SPSS version 21.0. software (SPSS Inc., USA). The Wilcoxon signed-rank test was used to determine the significance of change after UCB infusion from baseline function. Mann–Whitney tests were used to compare parameters between groups, with two groups divided by age and two groups divided by sex, respectively. P < 0.05 was considered statistically significant.
Results
Patients and selected UCB units
A total of 13 patients with GDD or ID were enrolled in this study. Demographics and baseline features are described in Table 1 (nine males and four females, age range of 23–149 months). Eleven patients were eligible to assess with BSID assessment manifesting 12.7 ± 8.8 months of mental and 10.7 ± 8.1 months of motor functions, while their average chronological age was 54.3 ± 34.7 months. As for the IQ assessment, WISC was applied for two, and WPPSI for one. IQ of other 10 patients were estimated using MFED due to limited cognitive ability (n = 6) or young age (n = 4). Beery VMI was not available in one patient due to young age. Two patients were diagnosed with ASD with relevant clinical manifestations. All undertook brain MRI, where six showed normal findings, and the others showed ventricular dilatation, periventricular white matter volume loss, etc. (Table 1). One patient was diagnosed with Lesch–Nyhan syndrome by PCR sequencing of the HPRT1 gene before this study, and another one had 1p duplication and 9q deletion. All the other participants did not reveal genetic abnormalities.
Demographics of Patients with Global Developmental Delay and Intellectual Disability Under Allogeneic Umbilical Cord Blood Infusion
Values are shown as mean ± standard deviation.
MRI findings in a preterm-delivered patient was within normal range.
Microcephaly was defined as less than the third percentile of head circumference.
Two patients took WISC, 1 patient took WPPSI, whereas IQ of the other 10 patients had to be estimated by use of MFED due to limitation of cognitive function or being younger than 3 years old.
Developmental age was assessable in 11 patients by use of BSID II.
The calculation formula was developmental age (months)/chronological age (months) × 100 (%).
Ten patients were tested for high-resolution chromosome study and multiplex ligation-dependent probe amplification and one was tested for array comparative genomic hybridization.
BSID, Bayley Scales of Infant Development; C-sec, cesarean section; GDD, global delayed development; GMFCS, gross motor function classification system; GMFM, gross motor function measure; ID, intellectual disability; MFED, München functional developmental diagnostics; MRI, magnetic resonance imaging; NSVD, normal spontaneous vaginal delivery; UCB, umbilical cord blood; WeeFIM, wee functional independence measure; WISC, Wechsler Intelligence Scale for Children; WPPSI, Wechsler Preschool and Primary Scale of Intelligence.
As for selected UCB units, ABO blood types were matched according to transfusion principle. Four patients were administered with HLA 1 mismatched units and nine patients with HLA 2 mismatched units. The mean TNC per body weight of infused UCB was 4.4 × 107 (Table 2).
Composition of Infused Allogeneic Umbilical Cord Blood Units in Each Patient
TNC, total nucleated cell.
Safety
No serious AEs of CTCAE grade 3 or higher were reported. Until 1 year after the intervention, AEs were reported from 11 patients (Table 3), which were all recovered. Within a month, the most common symptoms were fever accompanying upper respiratory tract infections, reported in six patients. Also, constipation and vomiting in two patients and urticaria in one were determined to be probably related to the therapy according to the occurrence time. A seizure attack was reported in one patient who had intermittent seizure attacks before this therapy, the frequency of which was not increased. Among the two patients who reported insomnia, one already suffered from insomnia before the therapy, and the other was diagnosed with sleep disorder due to snoring 6 months after UCB therapy. The average cyclosporine levels were within the target range (Supplementary Fig. S1). The laboratory study did not indicate any harmful effects of UCB therapy.
Adverse Events Which are Reported After Umbilical Cord Blood Therapy
Adverse events was recorded in accordance with CTCAE Version 4.0. Fever, upper respiratory infection symptoms, constipation, vomiting, and urticaria were reported and resolved with conservative treatment within 2 weeks.
An adverse event strongly related to UCB infusion was one case with urticaria. During the hospitalization, adverse events were recorded with close monitoring, and after discharge, it was recorded as a voluntary contact of the guardian.
Fever was defined as 37.8°C or higher.
One patient reported fever and upper respiratory infection symptoms and one patient reported insomnia about 6 months after the UCB therapy.
CTCAE, common terminology criteria for adverse events.
Functional improvements
Both BSID-II mental and motor scores and WeeFIM total score increased at all follow-up assessments from baseline until 12 months postintervention (P < 0.05). The GMFM total score also increased during the intervals, except for the first 3 months (P < 0.05; Fig. 2).

Outcomes after allogeneic UCB infusion in patients with GDD and ID.
Developmental quotients were calculated in 10 participants since the other 3 had ≥42 months of mental function during the study period. While raw BSID mental scale scores increased continuously throughout the study period, the BSID-II mental developmental quotient significantly increased during 0–3 months, then decreased during 6–12 months (P < 0.05; Fig. 3). In contrast, the motor developmental quotient did not show significant changes over time.
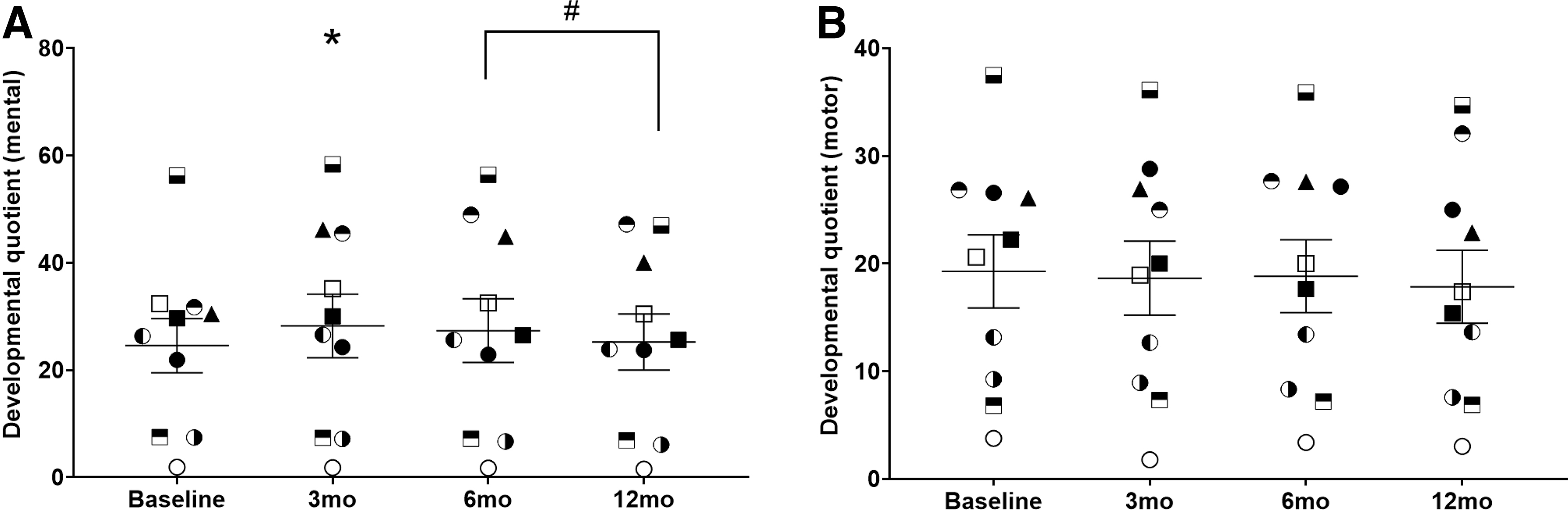
Developmental quotient changes of BSID-II mental and motor. Developmental quotient using
Scores of the PEDI functional skill scale (self-care, mobility, and social function) and caregiver assistance scale of self-care were elevated from 3 months after UCB treatment (P < 0.05). Then, self-care and social function of both scales showed continuous elevation up to 12 months (P < 0.05; Supplementary Fig. S2).
The results were similar for 10 patients who were evaluated with SELSI (another 3 patients were evaluated with PRES or REVT according to their older age and advanced language function). The scores significantly increased from baseline to 6 and 12 months (P < 0.05; Supplementary Fig. S3).
No significant improvements were found in the MFED-estimated IQ, WPPSI, WISC, and Beery VMI after treatment. Small improvements in Wechsler's IQ are described in Supplementary Table S1.
Additionally, functional outcome after UCB therapy was compared between younger age group (<60 months old) and older age group (≥60 months old), and also between male and female groups. As a result, the older group showed bigger increments of BSID-II motor development quotient during 3 months from baseline than the younger group (P < 0.05; Supplementary Fig. S5). There were no significant differences between male and female groups in the outcome parameters.
Two cases with long-term follow-up
When reviewed retrospectively several years after termination of this study, there were two cases who continued visiting our clinic until recent, the functional measures of whom were recorded beyond the study period. S02 (female) was followed for an additional 22 months after the end of the study. No genetic abnormality was detected and the brain MRI showed mild ventricle dilation, which was insufficient to explain her severe developmental delay status. UCB therapy was performed at 41 months of age. The increment of BSID mental score was dramatic during 12 months after the therapy. Her corresponding functional ages of mental scales, which was 13 months just before the intervention, became 25 months after intervention. However, it was trivial before and after the 12-month duration study period (Fig. 4).
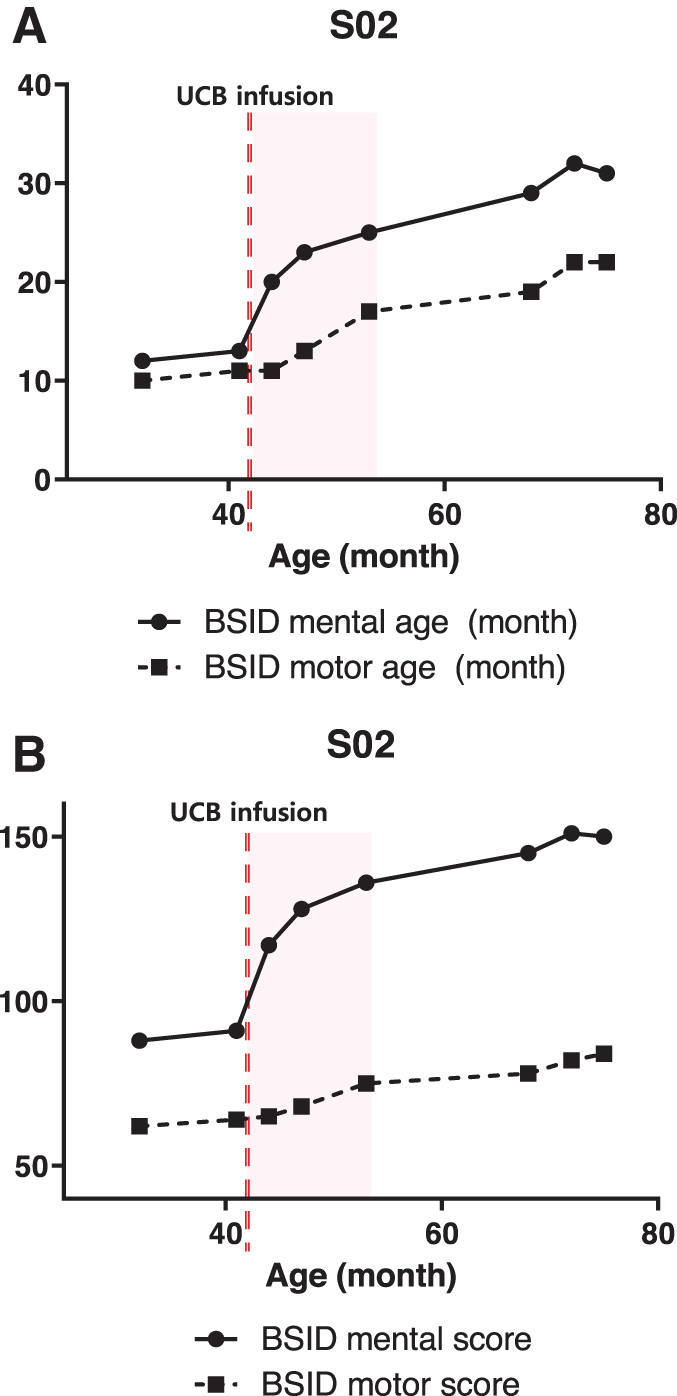
BSID-II changes in S02 who were continuously followed up beyond study. One patient was continuously followed up with BSID-II mental (dots) and motor (squares) scores 22 months beyond the study period.
S19 (male) was diagnosed with ASD and received UCB therapy at 11.5 years. Gene and brain MRI assessments did not reveal abnormality. The CARS score before the UCB therapy was 32 points, indicating autism, and the follow-up score 4 years after the UCB therapy decreased to 28.5, which was lower than the cutoff value [40] for autism. His parents reported that he became calmer and more communicable after the intervention.
Metabolic changes in 18F-FDG-PET
Except for 1 participant, brain FDG-PET data from 12 participants were available for analysis. There were no significant changes in glucose metabolism before and 12 months after UCB infusion.
Changes in cytokine expression
Peripheral blood samples from three participants were available for cytokine analysis. When these blood samples were drawn, there were no symptoms indicating inflammation and all showed normal C-reactive protein levels. The previously described patient S19 with autism who showed improvement in autistic manifestations showed downregulated mRNA expressions of TNF-α on D + 5, D + 8, and D + 14 days and IL-1β on D + 5 and D + 8 days (Supplementary Fig. S4). The other two samples did not show remarkable findings in the cytokine assays (S17 and S20).
Survey about satisfaction and long-term safety
A telephonic survey was conducted 80.7 ± 13.0 months after the UCB therapy involving the families of 10 participants. The other three could not be contacted. Satisfaction, with a Likert scale of 3 or higher, was obtained in 7 of 10 patients (70%) for item 1, 4 patients (40%) for item 2, and 6 patients (60%) for item 3 (Fig. 5). We also verified long-term safety through the absence of suspected intervention-related AEs beyond the trial period. The majority of participants, except for S17 and S20, were satisfied and S19 especially expressed strong satisfaction.

Survey about satisfaction of UCB therapy. The Likert scale ranged from 1 to 5 points, with 5 strongly agree (red), 4 generally agree (yellow), 3 somewhat agree (green), 2 generally disagree (light blue), and 1 strongly disagree (dark blue) for the three items of satisfaction survey.
Discussion
This prospective study aimed to verify the efficacy and safety of allogeneic UCB treatment. No serious AEs related to the therapy were reported. The other AEs were mild and transient. Considering the occurrence time, constipation and vomiting in two patients and urticaria in one patient might be related to UCB therapy. However, most of the other AEs were fever and upper respiratory infection, which seemed to be related with cyclosporine use, similar to our previous studies where allogeneic UCB was administered for cerebral palsy [41 –43]. In addition, in the survey conducted after more than 6 years, no long-term harmful effects were identified. Therefore, allogeneic UCB therapy may be regarded as safe in children with GDD and ID.
As for efficacy, improvements in most domains of development, such as cognition, speech, and motor function, were observed. However, as the patients were still in the developing stage, we could not conclude therapeutic efficacy of UCB for GDD. Therefore, we adopted a “developmental quotient” using BSID-II mental and motor scales. In addition, the BSID-II evaluation was conducted at 3-month intervals because there was no learning effect when conducted at 3-month intervals [44]. The results revealed significant facilitation of mental development during early period after UCB treatment, especially for the first 3 months. This effect diminished afterward, resulting in a decremental slope of the developmental quotient after 6 months. However, motor developmental quotient did not reveal significant change by lapse of time. Comparing BSID-II motor development quotient by age-specific analysis, we found that the improvement in motor development was higher in older children than in younger children.
It is well known that young children perform no better than older children in activities [45]. Two out of three analyzed children over 60 months of age showed improvement in the BSID-II motor development quotient, which seems to have been affected by UCB treatment rather than the natural course development.
In a patient (S02) with available long-term follow-up assessment, meaningful developmental improvement was observed only during the 1-year study period, while the improvement was trivial before and after the study. Therefore, these results might indicate a therapeutic response in mental development during a limited period after UCB infusion and also suggest that repeated UCB administration may be effective for a longer term [46 –48]. In the assessment of VMI and IQ derived from MFED, no significant differences were found. This might be due to the severe cognitive impairment status of the patients from the baseline and inadequate assessment of their changes. In several studies, the Wechsler intelligence test was administered every 3–6 months for cognitive function tests, so tests were conducted at 6-month intervals to evaluate cognitive development [49 –51]. However, for the Wechsler test, the cognitive status of most recruited patients was too severe to perform this test.
In a survey on the satisfaction of UCB therapy by guardians, 70% mentioned satisfaction with UCB therapy, and 60% said that they would recommend UCB therapy to other patients with GDD and ID. This is a meaningful result, considering the course of children with GDD and ID, which usually do not show satisfactory improvement even with various interventions.
As for the 18F-FDG-PET analysis, no specific changes were observed. Likewise, another clinical trial for cerebral palsy that performed the same assessment with a 12-month follow-up interval did not identify significant findings in 18F-FDG-PET analysis [52].
We obtained long-term follow-up results of patient S19 who was diagnosed with ASD. The patient's CARS score decreased below the cutoff value 4 years after UCB therapy. Interestingly, his blood sample showed downregulation of proinflammatory gene expressions, such as TNF-α and IL-1β. In contrast, participants who did not show remarkable changes in cytokines (S17 and S20) did not exhibit significant change, therefore, the parents were not satisfied. Although the exact mechanism is unknown, UCB may exert therapeutic effects by reducing neuroinflammation [12,53]. This is in line with a human pilot study that reported amelioration of ASD symptoms after taking an oral immunomodulatory agent that downregulated TNF-α and IL-1β [54]. Cognitive improvement after treatment is presumed to be caused by neurotrophic effects that last for a limited period. However, the etiology of children with GDD and ID is diverse, and the pathophysiology is not clearly understood [55,56]; therefore, further research is needed to determine which patients would show favorable response to UCB therapy.
While our results suggest promising results for children with GDD and ID, this prospective trial has limitations. This study was conducted with a small sample size, and children with GDD and ID have heterogeneous features and etiologies, which could have caused bias in the outcomes. Additionally, since being an uncontrolled open-label study, it was impossible to determine whether the improvements were due to a treatment effect or the natural developmental course of the children. However, it is known that children with GDD and ID generally gain abilities slowly in their natural course. Moreover, the severity of the disability correlates with later functional outcomes [57]. All patients who participated in this study had a severe degree of developmental delay. The average age of BSID-II estimated cognitive and motor development age was 12.7 and 10.7 months, respectively, which were much lower compared with their average chronological age of 54.3 months. Considering poor developmental courses in severe developmental delays, this study showed possible therapeutic effect in GDD and ID during a limited period.
Conclusion
The UCB therapy might benefit in developmental improvement, especially in cognition and speech development in children with GDD and ID for a limited period. UCB therapy is also a safe and satisfactory treatment option for these children. Further studies to enlighten therapeutic mechanisms of UCB therapy and to find out possible responders according to etiology or characteristics should be followed.
Footnotes
Acknowledgment
Umbilical cord blood was supplied by the CHA Cord Blood Bank.
Statement of Human and Animal Rights
All procedures in this study were conducted in accordance with the Medical Ethics Review Boards at the above medical centers.
Statement of Informed Consent
Written informed consent was obtained from a legally authorized representative before commencement of study.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health & Welfare, Republic of Korea (Grant No. HI16C1559).
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
Supplementary Figure S3
Supplementary Figure S4
Supplementary Figure S5
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.