
Abstract
Cellular therapy (CT) can be defined as the transference into a person of healthy cells to correct defective functions. Yesterday (1950–2010), CT consisted mostly of hematopoietic transplants for the treatment of a variety of hematological disorders. Interestingly, during that period of time other cell types with therapeutic potential—including certain lymphoid populations and other nonhematopoietic cells—were discovered and characterized; thus, CT became a promising discipline for the treatment of a broader diversity of diseases. Today (2011–2023), CT has significantly grownup through preclinical studies and clinical trials, and it is currently progressing toward its consolidation as one of the pillars of medicine in the 21st century. Indeed, different types of stem cells (e.g., hematopoietic, mesenchymal, neural, and pluripotent), as well as different lymphoid and myeloid cell populations (e.g., TILs, CAR-Ts, CAR-NKs, and DUOC-01) are being used in clinical settings or are being tested in clinical trials. For the past decade, several CT modalities have been developed, and today, many of them are being used in the clinic. Tomorrow (2024–2040), already established CT modalities will surely be improved and applied more frequently, and novel therapies (that will include cell types such as iPSCs) will enter and expand within the clinical ground. It is noteworthy, however, that despite significant advancements and achievements, problems still need to be solved and obstacles need to be overcome. Technical, ethical, and economic issues persist and they need to be addressed. Undoubtedly, exciting times of challenges and opportunities are coming ahead in the CT arena.
Introduction
Cellular therapy (CT) can be defined as the transference into a person of healthy cells to correct defective functions. A key feature of CT is that the cells that will be introduced into the patient can be manipulated ex vivo before the clinical procedure [1]. Manipulation of the target cells can be done to increase their cell number, to modify their function, or to generate a new type of cell. CT can be performed in autologous or allogeneic form, under hospitalized or outpatient settings. For the past few decades, several CT modalities have been developed, and today many of them are being used for the treatment of hematological, autoimmune, oncologic, neural, orthopedic, and metabolic disorders [2 –4].
Herein, a general, historical perspective of the evolution of CT is presented, summarizing some of the most representative developments occurred throughout two arbitrarily defined time periods: yesterday (1950–2010) and today (2011–2023). A perspective on the future development of CT is further presented as a third time period referred to as tomorrow (2024–2040).
CT Yesterday
After World War II, countries such as the United States and the United Kingdom became extremely interested in studying the deleterious effects of radiation on the human body. For obvious reasons, such kind of experiments could not be performed in humans, thus, different animal models were developed. During the late 1940s and early 1950s, Jacobson, in Chicago, Lorenz, in Bethesda, and Barnes, in Berkshire (UK), demonstrated that mice subjected to a lethal dose of radiation could survive if they received bone marrow cells from syngeneic mice [5 –7]. These research groups demonstrated, for the first time, that bone marrow transplants (BMT) were feasible in mammals.
Based on such preclinical studies, in the second half of the 1950s, Thomas et al. performed the first BMT to treat cancer patients, including patients with hematological neoplasms and patients with solid tumors, after chemotherapy and/or radiation [8]. Unfortunately, at that time very little was known about histocompatibility, chemotherapy was in its infancy, and knowledge on the hematopoietic system was scarce. Thus, all clinical procedures performed by Thomas et al. ended up with the patient's death [8]. Despite the poor results, that study demonstrated that, just like in mice, bone marrow cells could be safely transplanted from one person into another. This landmark study, in fact, could be considered as the birth of CT in humans.
During the following two decades, work by Dausset, Van Rood, and many others helped to decipher the HLA complex and its role in human transplantation [9 –11]. Till and McCulloch described the presence, in murine bone marrow, of a cell population capable of reconstituting the whole hematopoietic system when transplanted into irradiated mice [12]. They presented evidence indicating that such cells seem to be the ones responsible, at least in part, for the success of BMT, and established the basis for the identification and characterization of hematopoietic stem cells (HSCs).
Metcalf established the first in vitro cultures of murine and human bone marrow cells, and identified several molecular regulators of hematopoiesis, including colony-stimulating factors and interleukins [13]. And significant improvements were made in the development of conditioning regimens by incorporating new agents, such as busulfan and cyclophosphamide [14]. Thus, in the 1980s, hematopoietic cell transplantation (HCT) became a rather recurrent and encouraging therapeutic option for patients with hematological diseases [15].
Interestingly, by the middle of the 1980s, several groups reported that primitive hematopoietic cells, including stem and progenitor cells, could be mobilized from bone marrow into peripheral blood by means of chemotherapy or the use of myeloid stimulating factors, such as granulocyte-macrophage colony stimulating factor (GM-CSF) or G-CSF (reviewed in Ref. [16]). Soon after this observation, mobilized peripheral blood (MPB) was used as a source of hematopoietic stem and progenitor cells (HSPCs) for HCT, and after only a few years, the number of hematopoietic transplants using MPB exceeded that of hematopoietic transplants using bone marrow.
In that same decade, umbilical cord blood (UCB) entered the scene. Hal Broxmeyer and his team found that HSPCs are present in UCB at levels that could be relevant for HCT [17]. Based on this observation, on October 6, 1988, Eliane Gluckman performed the first hematopoietic transplant using UCB as the source of hematopoietic cells. The recipient was a 5-year-old boy with Fanconi's anemia [18]. It was a successful transplant. Soon after that, it became clear that UCB-derived cells possess biological properties that make them very attractive targets for the development of therapeutic strategies [19]. Indeed, UCB HSPCs possess higher proliferation and expansion potentials, as compared with their adult counterparts, and the frequency of immature, naive T lymphocytes in UCB is higher than in adult sources; thus, immune rejection is usually lower than when using bone marrow or MPB.
Besides their biological advantages, UCB cells showed several practical advantages, such as the high numbers of births, as compared with the numbers of marrow or blood donors, the lack of risk for the mother and the baby at the moment of obtaining UCB, and the possibility of establishing UCB cell banks, both public and private. All of this, in turn, favored the creation of international agencies devoted to regulating the use of UCB in clinical settings. By the turn of the 21st century, it became clear that UCB represented an extraordinary alternative as a source of HSPCs for HCT [20].
During the early 1970s, a new class of primitive progenitor-like cell was discovered. Friedenstein et al. isolated and characterized a cell type capable of forming in vitro colonies of spindle-shaped fibroblast-like cells [21]. Such marrow-derived adherent cells of mesenchymal origin were later known as mesenchymal stem cells (MSCs) due to the fact that, in addition to their colony-forming capacity, they were able to generate bone, cartilage, and adipose cells when cultured in vitro under particular conditions [22]. A few years later, the immunomodulatory properties of MSCs were described. As a result, their relevance immediately increased since their potential application in clinical settings for the treatment of a wide variety of disorders became evident [23].
Immune cells, in particular B and T lymphocytes, have always been appealing cell populations for the development of therapies directed to treat immunodeficiencies and cancer. In the 1980s, Rosenberg and his team at the National Institutes of Health (United States), developed cell therapies based on lymphoid populations capable of specifically targeting and attacking tumor cells [24]. Such lymphokine-activated killer cells and tumor infiltrating lymphocytes (TILs) were used in preclinical and clinical settings with very encouraging results.
In the 1990s, cells with stem cell properties were identified within certain regions of the mammalian brain (reviewed in Ref. [25]). Interestingly, such neural stem cells (NSCs) were observed not only in the fetal brain, but also in the adult brain. As expected, these cells immediately caught the attention of several research groups, since it was clear that their study could be relevant in our understanding of the development of the central nervous system and the origin of certain neurological diseases, and also in the development of treatments for such disorders [25].
During the last two decades of the 20th century and the first decade of 21st century, HCT represented the only CT modality widely used in the clinical arena. However, several experimental approaches and methods were underway, including the use of MSCs, immune cells, ex vivo expanded HSPCs, NSCs, and pluripotent stem cells (PSCs).
CT Today
According to the Worldwide Network for Blood and Marrow Transplantation (WBMT), during the 1957–2012 period (55 years), one million hematopoietic transplants were performed. Estimates from the same source indicate that between 2013 and 2019 (6 years), 0.5 million transplants were accomplished (>80,000 transplants per year worldwide) [26]. If this trend continues, the two-million mark will be reached by 2025. Among the hematopoietic transplants that are currently being performed, 55%–60% correspond to autologous transplants, and 75%–80% use MPB as the source of HSPCs.
Graft-versus-host disease (GVHD) has been recognized as one of the major problems associated with HCT, and considering that donor-derived T cells play a key role in such an immunologic reaction, different T cell depletion methods have been developed since the 1980s [27]. Currently, T cell-depleted haploidentical hematopoietic transplants—using marrow or MPB cells from related donors—are being carried out more frequently with good results [28].
During the past 35 years, the use of UCB transplants (UCBT) has increased in a significant way [29]. Since the first UCBT, it is estimated that >50,000 transplants have been performed worldwide, mainly in pediatric patients, and both public and private (family) UCB banks have been established. Today, ∼900,000 UCB units are being stored in public UCB banks from almost 50 countries, and it is estimated that >5 million units are being cryopreserved in family banks from almost 100 countries [29]. In the pediatric arena, the results reported for related and unrelated UCBTs seem to be as good as those using bone marrow or MPB. In adult patients, comparable survival rates and lower grade 2–4 GVHD have been observed, as compared with marrow or MPB transplants. However, there is usually delayed engraftment, and, in some cases, lower survival rates and higher transplant-related mortality.
Delayed engraftment is due, in great part, to a reduced absolute cell number in UCB units. Thus, different approaches have been explored to increase the absolute number of UCB cells transplanted. Such approaches include coinfusion of two different unmanipulated UCB units into a single patient, coinfusion of UCB cells together with T cell-depleted haploidentical peripheral blood, and coinfusion of UCB cells together with HSCs and HPCs from a different UCB unit that has been previously expanded ex vivo [29].
Multiple experimental methods have been used for the ex vivo expansion of UCB-derived HSPCs. Initial efforts to expand such cells were based on the use of different combinations of recombinant hematopoietic cytokines, including early- and late-acting cytokines. However, considering the fact that the in vivo development of HSPCs takes place in close association with bone marrow microenvironment cells, ex vivo systems have been established in which stromal cells, particularly MSCs, are used as feeder layers [30].
It is noteworthy that during the past 15 years, several molecules have been incorporated to the arsenal of elements that favor the expansion of primitive hematopoietic cells, including tetraethylenepentamine (TEPA), a copper chelator; Delta-like ligand-1 (DL1), a ligand for Notch; nicotinamide, a form of vitamin B3; StemRegenin-1 (SR1), a purine derivative that acts through engagement of the aryl hydrocarbon receptor; UM171, a pyrimidoindole derivative; OAC1, a small compound that activates the pluripotent transcription factor Oct4; and HDAC inhibitors, such as Valproic Acid [29,30].
As mentioned earlier, expanded HSPCs have usually been infused into the patient together with unmanipulated cord blood cells. However, in recent trials, ex vivo expanded cells have been applied as stand-alone grafts, and the results have been encouraging, since significant reductions in the time to neutrophil and platelet engraftment have been observed. This is the case for Omidubicel, a patient-specific cell product derived from a single UCB unit consisting of an ex vivo expanded CD133+ cell fraction (cells expanded in the presence of nicotinamide plus SCF, IL6, TPO, and FL) and a nonexpanded CD133– fraction [31,32]. Similar approaches using molecules such as UM171 are also being carried out [33].
Owing to their potent immunomodulatory activity, as well as their capacity to favor repair and regeneration of diseased or damaged tissue, MSCs are being widely used in clinical settings for the treatment of different conditions. Currently, one of the main applications of MSCs is in the context of HCT. Since MSCs suppress lymphocytes by paracrine mechanisms, including secretion of a variety of immunomodulatory molecules and metabolic regulators, they are being used to prevent or treat GVHD [34]. In contrast, it has also been shown that MSCs may help in the engraftment of HSCs after transplantation by secreting different hematopoietic stimulatory cytokines and/or by suppressing the residual host immunity [35,36].
Besides their use as part of HCT protocols, application of MSCs in clinical settings has expanded in a great manner for the past decade. MSCs, obtained from neonatal (placenta, amnion, or umbilical cord) or adult (bone marrow, dental pulp, adipose tissue, or peripheral blood) sources, are being used in the treatment of a wide variety of diseases and conditions, as evidenced by the number of clinical trials currently being carried out. Indeed, according to clinicaltrials.com, >1,130 clinical protocols using MSCs have been registered [36]. Most of them correspond to phase-2 and phase-1 trials (61% and 31%, respectively) and span over a wide variety of medical fields, including traumatology, pneumology, neurology, cardiology, immunology, hematology, and oncology [37].
During the past two decades, the use of lymphocyte populations as immunotherapies has grown in a significant manner. Indeed, improved TILs capable of recognizing tumor cells bearing somatic mutations have already been applied for the treatment of neoplasias such as colon and breast cancer [38,39]. On the other hand, chimeric antigen receptor (CAR)-T cells are currently one of the most promising CT modalities for cancer treatment. They consist of T cells that have been genetically modified by the insertion of an engineered gene that encodes for a receptor molecule that specifically recognizes a particular antigen present on the surface of a cancer cell [40]. When choosing the target antigen and designing the CAR gene, it is important to make sure that such an antigen is not present in normal cells of different healthy tissues, so they will not be recognized and attacked by the immune cells.
Today, CAR-T cells are widely used for the treatment of different types of lymphoid malignancies, including lymphomas and leukemias, as well as multiple myeloma [40]. The results reported so far are promising, since a significant proportion of patients with B lymphoid neoplasias have shown partial or complete tumor regression after treatment with CD19 CAR-T cells. Consequently, the United States Food and Drug Administration (FDA) as well as the European Medicine Agency (EMA) have already approved CAR-T cell products for the treatment of some B lymphoid malignancies.
A great research activity around NSCs has been taking place during the past few years. Indeed, human NSCs, obtained mostly from fetal tissues, have been used in clinical trials for the treatment of different types of neural disorders, including demyelinating conditions, spinal cord injury, and macular degeneration [25,41].
CT Tomorrow
In the next 10–15 years, CT will surely accomplish significant goals in the treatment of a great number of disorders by improving the use of different stem cells and lymphoid cells that are currently being applied in the clinic, and with the novel use of several cell populations that are just entering the clinical field. However, there are still quite a few issues that must be solved and different obstacles that should be overcome.
There is no doubt that MSCs will continue as one of the pillars of CT in the years to come. They are easily accessible, since they can be obtained from different tissues; the culture conditions required for their ex vivo production are relatively simple; they can be produced on large scales under GMP conditions; and their mechanisms of action favor their use for the treatment of a wide variety of diseases [42]. However, there is evidence that they undergo replicative senescence that arrests cell proliferation, have a higher chance of malignant transformation, and may possess genetic instability [42]. Thus, further studies focused on their in vitro and in vivo biology need to be carried out to present more convincing evidence regarding their long-term safety when introduced into a patient.
Although CAR-T cells have proved to be efficient in the treatment of different B cell lymphoid neoplasias and other hematological malignancies, its use in solid tumors has encountered several obstacles. Indeed, due to the structural organization of the tumor microenvironment, CAR-T cells cannot effectively infiltrate into the tumor, and because of the immunosuppressive action of such a microenvironment, CAR-T cell activity is limited. Furthermore, the relatively short time of CAR-T cells in vivo, and their limited proliferation capacity within the host result in reduced efficacy of such cells [43]. Thus, different strategies must be established to make CAR T cell therapy more efficient for the treatment of solid neoplasias. One approach that is currently under investigation is the genetic modification of HSCs by introducing a CAR gene (e.g., CD19), so that HSCs will produce immune cells of multiple lineages capable of sustaining a long-term immune response against specific tumor cells [44].
Ex vivo expansion of UCB HSPCs has been achieved and the results obtained in clinical settings have been encouraging. However, such an approach has some issues that need to be solved. First, the results obtained by different groups vary depending on the expansion method used; thus, the methodologies need to be standardized, so that although not all expansion methods are the same, they all must be reproducible and reliable. Second, any expansion method must guarantee that the expanded cell population is genomically stable and that it retains its functional properties. Indeed, there is evidence that when expanding UCB-derived HSPCs, the cells generated in vitro, although identical in immunophenotypic terms, may not be functionally identical to equivalent cells obtained directly from fresh UCB [45]. Third, expansion protocols increase the cost of UCB transplants, which already are expensive. Thus, it will be important to make UCB expansion protocols not only reliable, but also affordable.
Undoubtedly, CT will expand significantly during the following decade since there are different cell populations that are just entering the clinical field, contributing to the development of novel therapeutic approaches. DUOC-01, for example, is a cell product derived from UCB CD14+ monocytes, which consists of slow-proliferating attached motile cells expressing CD11b, CD14, and macrophage and microglia markers, and capable of secreting IL-6 and IL-10 [46]. DUOC-01 has been shown to favor myelination of the brains of immunodeficient mice in which demyelination had been induced; thus, it has been suggested that DUOC-01 could be beneficial in treating demyelinating conditions [47].
It has been recently shown that many different types of cells produce extracellular vesicles containing DNA, proteins, lipids, and noncoding RNAs. Such vesicles, known as exosomes, seem to be key elements for intercellular communication. MSC-derived exosomes play key roles in cancer therapy resistance. Indeed, there is important evidence indicating that MSC-derived exosomes carry molecules (e.g., miRNAs) that favor tumor resistance to chemotherapy, radiotherapy, targeted therapy, and immunotherapy [48].
Interestingly, because exosomes are involved in intercellular communication, possess strong tumor tropism, possess low immunogenicity and toxicity, are capable to escape clearance and to cross biological barriers, it has been suggested that MSC-derived exosomes could be used as carriers of anticancer chemical agents and biomolecules [49]. In this regard, it is noteworthy that different miRNAs have already been used in preclinical trials as anticancer biomolecules contained within MSC-derived exosomes [48]. Furthermore, engineered MSC-derived exosomes have already been tested in animal models and the results are promising [49].
Since their initial characterization and development, PSCs, including both embryonic stem cells (ESCs; obtained from blastocysts) and induced-pluripotent stem cells (iPSCs; obtained from reprogramming of adult somatic cells), have represented a promising tool for the treatment of different types of diseases [50,51]. Ethical issues (influenced by religious beliefs) have hampered the progress in human ESC development as a therapeutic tool. Human iPSCs, in contrast, have already been used in preclinical and clinical trials aimed at studying, modeling, and treating a variety of disorders [42].
Accordingly, it is expected that in the near future, iPSCs will be used more frequently in the clinical arena. There are, however, some issues that need to be looked at before incorporating iPSCs in clinical settings. For example, there is evidence that some reprogramming methods can cause tumorigenesis due to unspecific integration of viral sequences; quality assessments need to be established and incorporated into the general practice when generating iPSCs since there is great variability between reprogramming methods [42].
Application of NSCs in clinical procedures will surely increase in the next decade. There are two major sources of human NSCs: fetal tissues and iPSCs. Regarding the former, ethical issues have been observed as elements for discussion when preparing the agenda for the clinical use of NSCs. Regarding the latter, technical concerns exist, since it is still not clear whether iPSCs-derived cells are safe and functionally efficient when introduced into a patient. Nevertheless, there is confidence in that both of these issues will be solved in the near future. NSCs are currently being used for the treatment of demyelinating conditions, spinal cord injury, and retinal disorders; interestingly, a significant number of preclinical studies are being carried out for the treatment of conditions such as Alzheimer's and Parkinson's diseases [52,53]. Thus, NSCs, derived from either fetal tissues or from iPSCs, will surely be used for treating such neurodegenerative disorders.
Based on the panorama described herein, there is no doubt that during the following decade, the CT scenario will be dominated by five cell types: hematopoietic, mesenchymal, immune, neural, and pluripotent (Fig. 1). Hematopoietic cells will include not only primary HSPCs from bone marrow, MPB, and UCB, but also ex vivo generated HSPCs, as well as particular mature cell populations, such as macrophages. MSCs, which up to now have been considered as a single population, will include specific MSC subpopulations identified and selected based on specific functional properties.
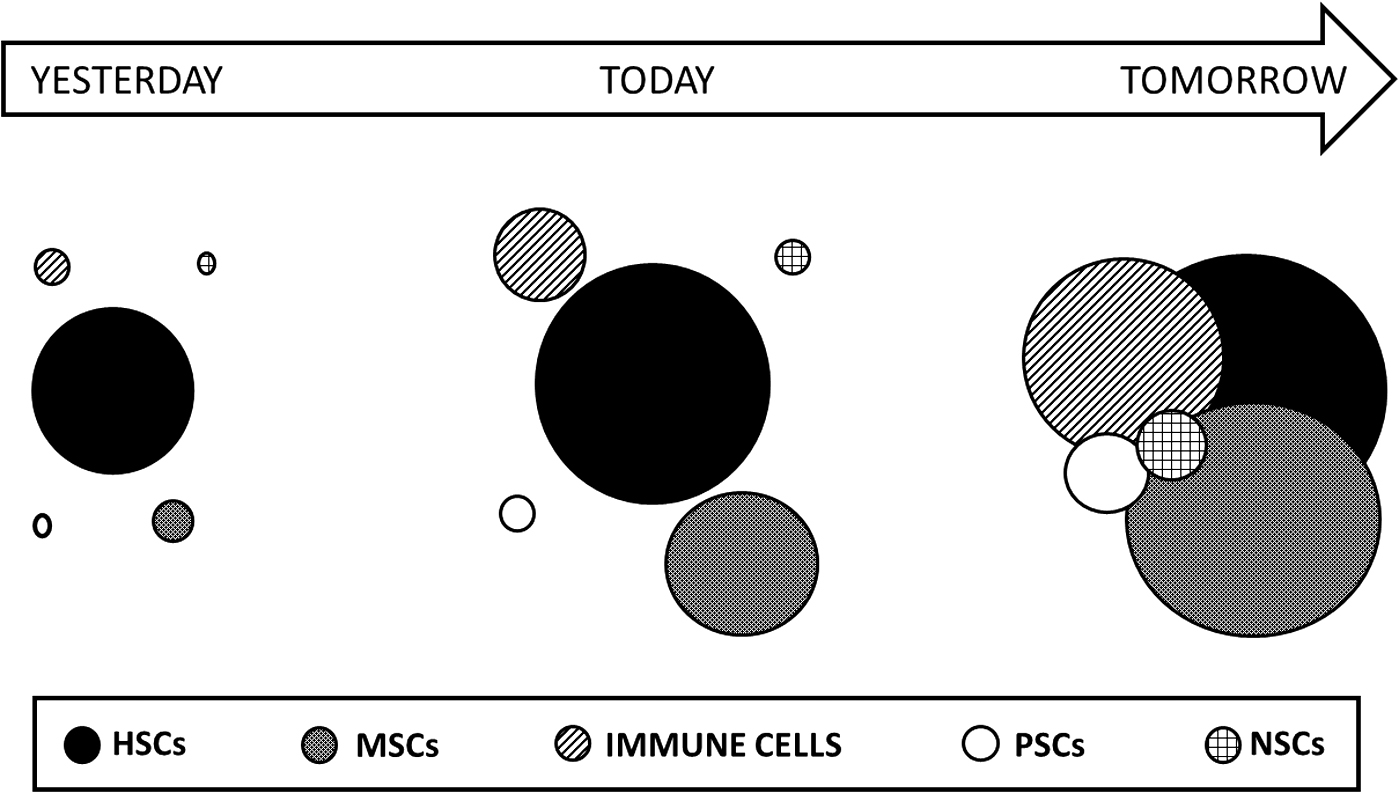
Graphical representation of the development of CT throughout time. The figure illustrates the application of HSCs, MSCs, immune cells (B, T, and NK cells, as well as macrophages), NSCs, and PSCs in preclinical and clinical studies for the treatment of a variety of diseases. The term YESTERDAY corresponds to the period between 1950 and 2010; TODAY corresponds to the period between 2011 and 2023; TOMORROW corresponds to the next 10–15 years. The size of the circles represents the degree of development, involvement, and impact of each cell type in the preclinical and clinical arenas. CT, cellular therapy; HSCs, hematopoietic stem cells; MSCs, mesenchymal stem cells; NSCs, neural stem cells; PSCs, pluripotent stem cells.
Immune cell therapy will mainly consist of different types of CAR cells and TILs, although primary T, B, and NK cells will also be used. Pluripotent cells will mostly consist of iPSCs, which will be a major source for obtaining NSCs. Despite this, we cannot rule out the possibility that, once some ethical issues are solved, fetal-derived NSCs, as well as pluripotent ESCs, will also be applied more frequently in the clinic. It is also possible that other organ/tissue-specific cells will enter the clinical scene as well.
Finally, it is important to point out that in the near future, cell therapies combining two or more different cell types will surely become common practice, since each cell type can contribute particular features that will complement each other [54]. For example, it is appealing to imagine that in 5 years from now, a patient with a particular medical condition could be treated using a multi-CT approach that includes the anticancer effects of CAR-T cells, the capacity of ex vivo expanded HSCs to reconstitute the hematopoietic system, and the immunosuppressive capacity of MSCs.
Concluding Remarks
Yesterday, CT was seen as a promising discipline within the vast medical scenario. Today, CT represents one of the pillars of medicine in the 21st century. Indeed, different types of cells with stem cell properties (e.g., hematopoietic, mesenchymal, neural, and pluripotent), as well as different myeloid and lymphoid cell populations (e.g., TILs, CAR-Ts, CAR-NKs, and DUOC-01) are being widely used in clinical settings or are being tested in clinical trials. Tomorrow, already established CT modalities, as well as novel approaches (including cell types such as iPSCs) will be applied more frequently. It is noteworthy, however, that despite significant advancements and achievements, major problems still need to be solved and obstacles need to be overcome. Technical, ethical, and economic issues are still present and they need to be addressed. Undoubtedly, exciting times of challenges and opportunities are coming ahead in the CT arena.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
Research in H.M.'s laboratory is supported by grants from Instituto Mexicano del Seguro Social (IMSS) and from Consejo Nacional de Ciencia y Tecnologia (CONACYT), Mexico.