
Abstract
In recent years, cell-based therapies have emerged as a promising approach for mitigating radiation-induced injury. Acute radiation syndrome (ARS) results from exposure to high doses of radiation over a short time period. This study aimed to compare the efficacy of donor-recipient chimeric cell (DRCC) therapy in mitigating ARS induced by a total body irradiation (TBI) dose of 10 gray (Gy). Thirty irradiated Lewis rats were employed as ARS models to assess the efficacy of systemic-intraosseous transplantation of different cellular therapies in five experimental groups (n = 6/group): saline control, isogenic bone marrow transplantation (isoBMT), allogeneic BMT (alloBMT), DRCC, and alloBMT+DRCC. DRCC were created by polyethylene glycol-mediated fusion of bone marrow cells from 24 ACI (RT1a) and 24 Lewis (RT11) rat donors. The creation of DRCC and chimeric state was confirmed by flow cytometry (FC) and confocal microscopy (CM). Recovery of blood parameters was evaluated through complete blood count analysis. Graft-versus-host disease (GvHD) signs were assessed clinically and histopathologically using kidney, skin, and small intestine biopsies. FC and CM confirmed the fusion feasibility and the chimeric state of DRCC. A 100% mortality rate was observed in the saline control group, whereas a 100% survival was recorded following DRCC transplantation, correlating with significant recovery of peripheral blood parameters. In addition, no clinical or histopathological signs of GvHD were observed after DRCC and alloBMT+DRCC transplantation. These findings confirm efficacy of DRCC in mitigating GvHD, promoting hematopoietic recovery, and increasing animal survival following TBI-induced ARS. Moreover, tolerogenic and immunomodulatory properties of DRCC therapy support its feasibility for clinical applications. Therefore, this study introduces DRCC as an innovative bridging therapy for alleviating the acute effects of TBI, with broad implications for stem cell research and regenerative medicine.
Introduction
Currently, the escalating demand for nuclear energy across various industrial sectors and the medical field has resulted in a more prevalent use of nuclear power. 1,2 Consequently, the probability of exposure to high doses of irradiation poses a substantive issue of concern. Total body irradiation (TBI) can induce acute radiation syndrome (ARS), a potentially fatal condition if left untreated. 3 ARS encompasses distinct symptoms, the severity of which depends primarily on factors such as the dose of irradiation, rate of exposure, and exposure geometry. 4 These symptoms predominantly affect the hematopoietic, gastrointestinal, and neurovascular systems due to the high mitotic rate of their cells. 5
Current treatment strategies typically involve allogeneic bone marrow transplantation (alloBMT) combined with supportive therapies. 6,7 However, the high mortality rates associated with ARS render existing therapeutic options unsatisfactory. Furthermore, the use of alloBMT requires human leukocyte antigens (HLA)-donor compatibility and carries the risk of graft-versus-host disease (GvHD). 8 Therefore, there is a need to explore novel, universal cellular therapies effective in treating ARS and other irradiation-induced injuries.
To overcome these limitations, we propose a novel approach involving the ex vivo creation of donor-recipient chimeric cells (DRCC). This strategy could serve as a bridging therapy until an HLA-matched donor becomes available. Previous studies conducted by our laboratory have validated the efficacy of DRCC transplantation as a promising alternative to bone marrow (BM)-based cellular therapies, demonstrating DRCC’s ability to support tolerance induction in allotransplantation. 9 –11 In addition, we confirmed the tolerogenic properties of DRCC, significantly enhancing the survival rates of allogeneic tissue grafts. 12 –14 Furthermore, the immunomodulatory potential of DRCC may eliminate the need for immunosuppression, given their inherent immunoregulatory capabilities. 9
Building upon the encouraging results of our previous investigations, we aimed to evaluate the recovery of peripheral blood parameters following TBI in the context of DRCC transplantation. We established an experimental Lewis rat model exposed to 10 Gy dose of TBI. The presented model facilitated a comprehensive assessment of peripheral blood parameter reconstitution following the systemic-intraosseous transplantation of different cellular therapies, including isoBMT, alloBMT, DRCC, and alloBMT+DRCC. Our findings demonstrate that DRCC therapy promotes the recovery of peripheral blood parameters. Furthermore, DRCC transplantation does not result in generation of clinical or histological changes characteristic of GvHD. Therefore, this study conclusively demonstrates the innovative concept of DRCC therapy for the clinical management of ARS.
Materials and Methods
Animals and experimental groups
This study was approved by the Institutional Animal Care and Use Committee (IACUC) of University of Illinois at Chicago. All animals received humane care in compliance with the National Research Council’s “Guide for the Care and Use of Laboratory Animals,” published by the US National Institutes of Health. A total of 84 male Lewis rats (RT11) (strain: LEW, RRID: RGD_737932) and 54 ACI rats (RT1a) (strain: ACI, RRID: RGD_737892), 8–10 weeks of age, purchased from the Charles River Laboratories (Chicago, Illinois, USA), were used. Thirty male fully major histocompatibility complex (MHC) mismatched ACI rats served as alloBMT donors. Thirty male fully-MHC matched Lewis rats served as isoBMT donors. In addition, 24 male ACI rats and 24 male Lewis rats served as BM donors to create DRCC. BM cells were isolated in a sterile manner, as previously described. 9,15,16 The cellular therapies were transplanted through intraosseous injection into the right femur of Lewis rats, as previously reported. 13,17 –19 Thirty Lewis rat recipients were randomly divided into five experimental groups (n = 6/group) (Fig. 1a): Group 1 control received 0.1 ml of saline and antibiotic therapy (trimethoprim-sulfamethoxazole, 40 mg/200 mg per 5 ml, Hi-Tech Pharmacal); Group 2 received isoBMT (80 x 106 cells) from the Lewis donors; Group 3 received alloBMT (80 × 106 cells) from the ACI donors; Group 4 received DRCC (5–8 × 106 cells) created by ex vivo fusion of BM cells from ACI and Lewis donors; and Group 5 received alloBMT (80 × 106 cells) from the ACI donors combined with DRCC (8 × 106 cells) created by fusion of BM cells derived from ACI and Lewis donors.

Experimental design of total body irradiation procedure.
Total body irradiation model
Thirty male Lewis recipient rats were exposed to a total dose of 10 Gy TBI, administered at a rate of 0.4–1.0 Gy/min and delivered using Cs-137 radionuclide (Fig. 1b). The irradiation procedure was comprehensively described in our previous study. 20,21
Donor-recipient chimeric cell creation through ex vivo fusion procedure
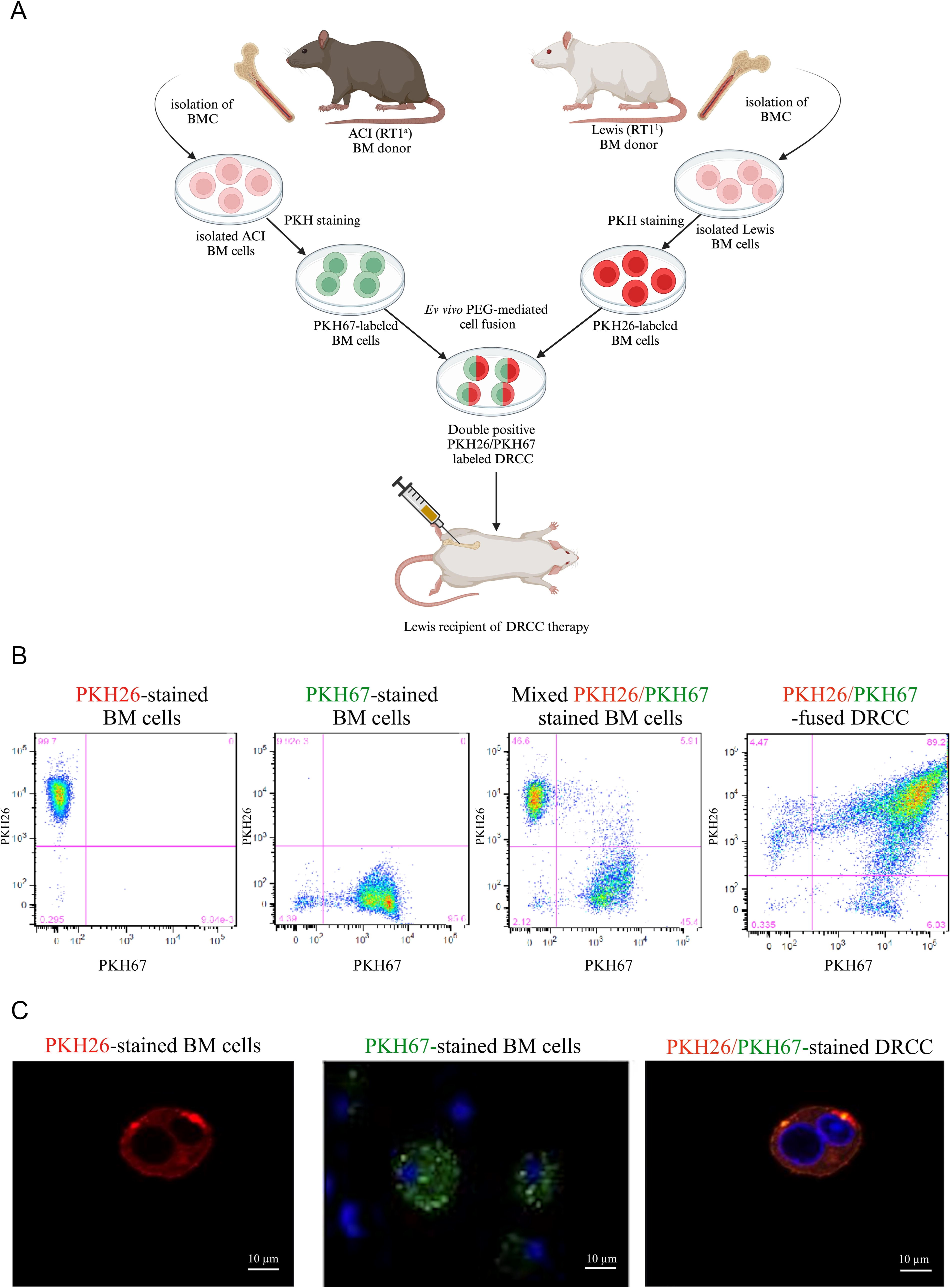
DRCC were created from BM cells derived from ACI and Lewis rat donors (Fig. 2a). The method for isolating BM cells, creating DRCC through cell fusion, and assessing DRCC properties were previously described in detail. 9,10,12,15,16 Briefly, BM cells were isolated from femurs of randomly selected ACI (RT1a) and Lewis (RT11) rat donors, and subsequently fluorescently stained with PKH26-red (ACI) or PKH67-green (Lewis) fluorescent membrane dyes (Sigma-Aldrich, St. Louis), respectively, according to manufacturer’s instructions. Next, donor cells were mixed in a 1:1 ratio and suspended in serum-free Roswell Park Memorial Institute Medium 1640 medium (Thermo Fisher Scientific). Cell fusion was performed using a 1.46 g/ml polyethylene glycol (PEG) 4000 solution (EMD, Burlington, MA, USA) containing 16% DMSO (Sigma-Aldrich), as described previously. 9,12,15,16 Fluorescence-activated cell sorting (FACS, BD FACSAriaTM II cell sorter, Becton Dickinson) was applied to isolate PKH26/PKH67-labeled cells, representing the DRCC population. The chimeric state of DRCC was confirmed by flow cytometry (FC) and confocal microscopy (CM), as outlined in prior studies. 9,18
Confirmation of the creation of DRCC from rat BM cells by ex vivo PEG-mediated fusion.
Survival rate and body weight evaluation
The rats underwent daily observations to assess the animals’ well-being and survival rates over the 90-day observation period. The baseline body mass of each animal was recorded at the beginning of the study and was then measured daily during the initial 8 days, and subsequently, every other day throughout the 90-day observation period.
Blood sampling analysis
On days 1, 5, 20, 40, 60, and 90 from the beginning of the observation period, a sample of 0.3 ml peripheral blood was collected from the external jugular vein. An additional blood sample was collected on day 0 before TBI exposure and the application of therapies as a reference. Complete blood count evaluation, including white blood cells (WBCs) (lymphocytes, monocytes, and neutrophils), red blood cells (RBCs), platelets (PLTs), hemoglobin (HGB), and hematocrit (HCT), was performed at the blood sampling days. The procedure of blood drawing has been previously described. 20,21
Clinical evaluation
All animals were observed for signs of GvHD, daily for the first 8 days, and subsequently, every other day over the period of 90 days. The following clinical parameters were assessed: activity in the cage, body posture, and fur coverage for each individual animal. 22,23
Histopathological assessment
The histological evaluation of GvHD occurrence entailed examining kidney, skin, and small intestine samples harvested on the 90th day of study endpoint. Frozen sections of these tissues were subjected to hematoxylin and eosin staining, followed by assessment using both histological criteria 24 and a GvHD scoring system. 25,26
Statistical analysis
Data are presented as mean ± standard error of the mean (SEM). Statistical analyses were conducted using GraphPad Prism software (ver. 9.2.1, RRID: SCR_002798, Dotmatics, Boston, MA, USA) and Microsoft Excel (ver. 16.0, Microsoft Corporation, Redmond, WA). Two-way ANOVA was employed for group comparisons, with statistical significance set at P < 0.05. Graphs display mean values with SEM error bars, with statistical significance denoted as follows: *P < 0.05, **P < 0.01, ***P < 0.001, and ****P < 0.0001.
Results
Confirmation of DRCC creation
Study design outlining the ex vivo PEG-mediated cell fusion procedure of BM cells from ACI and Lewis rat donors is presented on Figure 2a. The resulting DRCC population exhibited >95% purity, with the fusion procedure’s efficacy assessed at 89.2% through FC analysis (Fig. 2b). Furthermore, CM validation (Fig. 2c) confirmed the quality of the created DRCC, revealing the presence of PKH26/PKH67 double staining, indicative of the chimeric state.
Survival outcomes
Figure 3a illustrates the survival rate changes post-TBI and therapy administration. In the control group, three rats died on the 9th day, followed by the remaining three rats on the 10th day post-TBI, resulting in no surviving animal beyond the 10th day. In the DRCC group, two rats died on days 17 and 60 due to surgical complications during blood drawing and were excluded from the study. The remaining four rats survived until the 90-day study’s endpoint, revealing a 100% survival rate. Survival rates in groups receiving isoBMT, alloBMT, and alloBMT+DRCC remained at 100% throughout the 90-day observation period.

Changes in survival rate and body weight following 10 Gy TBI and different applied therapies over a 90-day observation.
Body weight recovery
Changes in rat body mass following the administration of different cellular therapies assessed after 10 Gy TBI over the 90-day observation period are presented in Figure 3b. Initially, all rats experienced a decrease in body weight by the fifth day, reaching around 80% of the baseline weight; however, from the sixth day after TBI, a progressive weight gain was observed across all experimental groups, ultimately resulting in surpassing the baseline weight by the end of the 90-day observation period.
Peripheral blood parameter recovery
Summary of the dynamics of changes in the peripheral blood parameters among experimental groups assessed after 10 Gy TBI and administration of cellular therapies over 90 days is presented on Figure 4.

Effect of applied cellular therapies after 10 Gy TBI on complete blood count changes over a 90-day observation. Assessment of the effect of saline, isoBMT, alloBMT, DRCC, and alloBMT+DRCC therapies on the changes of blood count components after 10 Gy TBI confirms that DRCC promotes recovery of peripheral blood. Zero days stand for baseline values and a reference.
On day 1, both DRCC therapy and alloBMT+DRCC showed elevated WBC counts compared to saline control (P < 0.05) (Fig. 4a). By day 20, DRCC therapy led to a 16-fold increase in WBC counts compared to saline control (P < 0.01), whereas alloBMT+DRCC exhibited 15 times higher counts (P < 0.0001) compared to saline control. AlloBMT+DRCC also displayed a twofold increase compared to isoBMT therapy (P < 0.0001), similar to DRCC versus isoBMT (P < 0.0001). By day 40, DRCC revealed nearly a 2.5-fold increase in WBC counts compared to saline control (P < 0.0001), with alloBMT+DRCC showing 2.4 times higher counts (P < 0.0001) compared to saline control. On day 90, DRCC therapy maintained higher WBC counts than saline control (P < 0.01), with counts 1.5 times higher compared to alloBMT group (P < 0.01).
By day 5, alloBMT showed higher RBC counts versus DRCC (P < 0.01), with DRCC exhibiting higher RBC counts compared to alloBMT (P < 0.05) and saline control (P < 0.01) by day 60 (P < 0.01) (Fig. 4b). By day 90, isoBMT showed higher RBC counts compared to alloBMT+DRCC (P < 0.05).
On day 20, the DRCC group showed a threefold increase in PLT counts compared to alloBMT therapy (P < 0.0001), and over a fourfold increase compared to saline control (P < 0.0001) (Fig. 4c). Similarly, a nearly threefold increase was observed in PLT counts following alloBMT+DRCC therapy compared to alloBMT (P < 0.0001), and a fourfold increase compared to saline control (P < 0.0001). By day 40, DRCC group revealed higher PLT counts compared to alloBMT (P < 0.0001), with alloBMT+DRCC showing over a 2.5-fold increase compared to saline control (P < 0.0001). By day 60, alloBMT+DRCC showed higher PLT counts versus saline control (P < 0.0001), and on day 90, DRCC showed higher PLT counts versus alloBMT (P < 0.0001).
On day 20, lymphocyte values exhibited a 15-fold increase in DRCC therapy compared to saline control (P < 0.0001), with both isoBMT and alloBMT groups showing nearly twofold increase compared to saline control on day 40 (P < 0.0001) (Fig. 4d). By day 90, DRCC therapy revealed higher lymphocyte counts versus saline control (P < 0.0001) and alloBMT (P < 0.0001).
AlloBMT+DRCC therapy showed higher monocyte counts compared to both alloBMT (P < 0.0001) and saline control (P < 0.0001) on day 20, and on day 40 (P < 0.0001) (Fig. 4e).
Neutrophil counts on day 1 were over twofold higher in the DRCC group than alloBMT (P < 0.0001), and 1.3-fold higher compared to alloBMT+DRCC (P < 0.05) (Fig. 4f). By day 20, alloBMT+DRCC displayed nearly a threefold increase in neutrophils versus saline control (P < 0.001), with alloBMT showing nearly a 2.5-fold increase compared to saline control (P < 0.01).
Throughout the 90-day period, HGB (Fig. 4g) and HCT (Fig. 4h) levels remained comparable across all therapies.
Clinical outcomes
The effects of different cellular therapies on the animal activity, body posture, and fur coverage assessed after exposure to 10 Gy TBI over a 90-day period are presented in Figure 5.

Clinical assessment of rats following 10 Gy TBI and different applied therapies over a 90-day observation. The evaluation of activity, posture, and fur coverage of rats after 10 Gy TBI and application of saline, isoBMT, alloBMT, DRCC, and alloBMT+DRCC.
On day 10, the saline control group showed significantly reduced activity compared to the isoBMT group (P < 0.0001) and both the alloBMT and DRCC groups (P < 0.0001) (Fig. 5a). Similar trends were observed between the saline control and alloBMT+DRCC groups (P < 0.0001). Throughout the remaining observation period, the alloBMT group consistently had the lowest activity levels.
On day 10, the saline control group exhibited the poorest posture compared to all other groups (P < 0.0001) (Fig. 5b). The alloBMT group consistently displayed the worst body posture throughout the remaining observation period.
On day 10, fur coverage was significantly worse in the saline control group compared to isoBMT group (P < 0.001), as well as compared to both alloBMT and DRCC groups (P < 0.05 and P < 0.0001, respectively) (Fig. 5c). This trend continued when comparing the saline control group with the alloBMT+DRCC group (P < 0.001). In addition, fur coverage was worse in the alloBMT group compared to DRCC group (P < 0.05). On day 20, fur coverage remained worse in the alloBMT group compared to the DRCC group (P < 0.01) and alloBMT+DRCC group (P < 0.05). Throughout the observation period, except on day 50, the alloBMT group consistently exhibited the poorest fur coverage.
GvHD histological outcomes
The histopathological changes indicating GvHD presence in tissue biopsies are summarized in Figure 6. The incidence of GvHD-associated histological changes in the kidney and skin samples was significantly lower in isoBMT, alloBMT, DRCC, and alloBMT+DRCC groups (P < 0.0001 for all measurements) compared to the control group. In small intestine biopsies, more pronounced GvHD changes were observed in the saline control compared to the isoBMT(P < 0.0001), alloBMT (P < 0.05), DRCC (P < 0.0001), and alloBMT+DRRC (P < 0.0001) groups. In addition, the changes were significantly more severe in the alloBMT group compared to the DRCC group (P < 0.05).
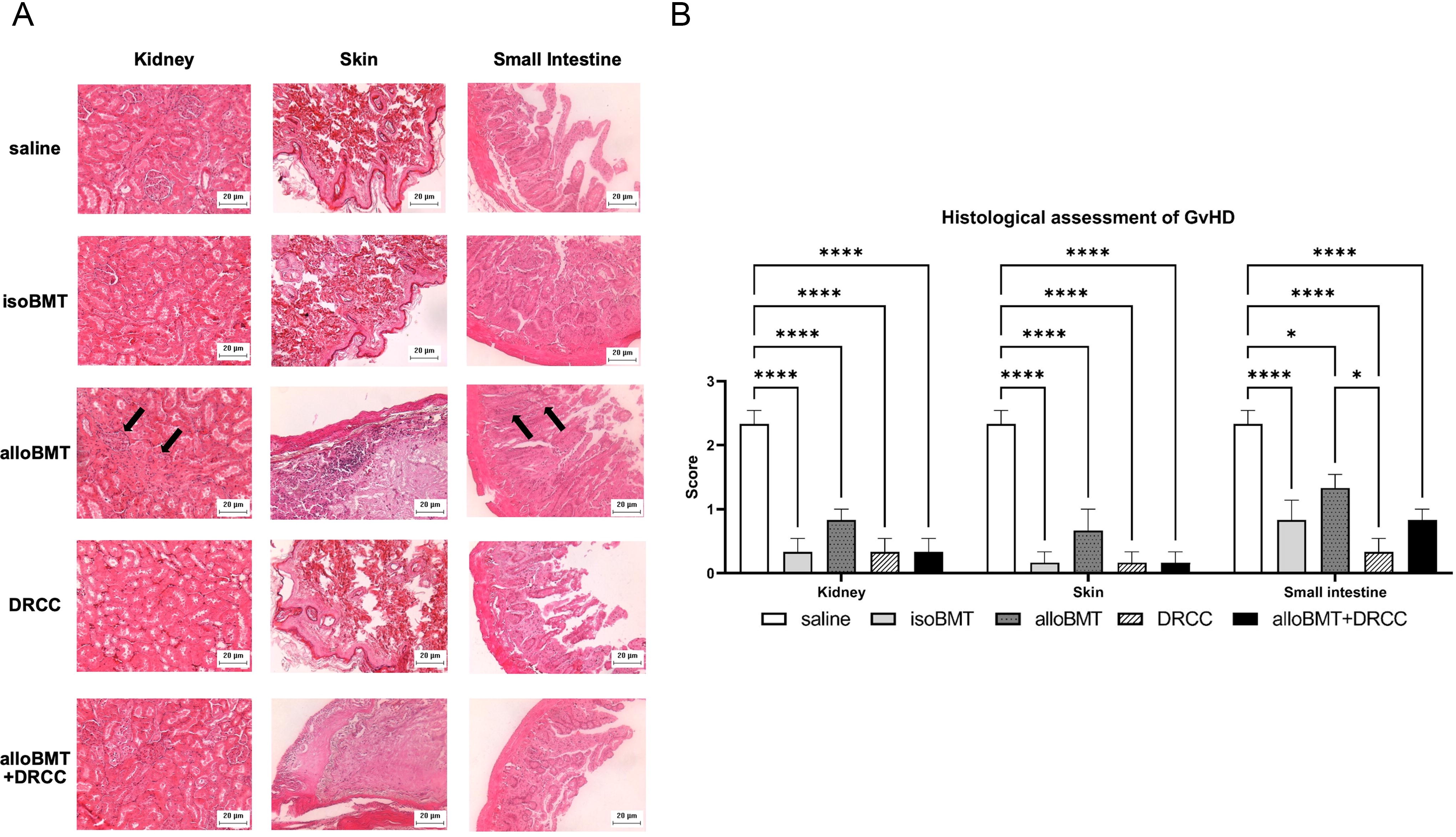
Effect of different therapies on the pathology of kidney, skin, and small intestine after 10 Gy TBI and different applied therapies.
Discussion
Radiation exposure can lead to ARS, primarily manifesting as hematopoietic syndrome with high mortality rates if untreated. 27 –29 Given the limitations of current treatment options, particularly alloBMT, exploring novel, highly effective therapies is crucial for ARS management. This study proposes DRCC therapy as a promising bridging therapy for ARS.
Building upon promising previous research on chimeric cells, 12,15,16 we aimed to assess the immunomodulatory properties of DRCC and their impact on peripheral blood parameter reconstitution after TBI in the context of ARS. The envisioned approach of DRCC therapy, characterized by a donor/recipient phenotype, strives to establish a clinically viable cellular therapy that provides reduced immunogenicity, established immunomodulatory characteristics, and enhanced recovery of peripheral blood parameters compared to alloBMT.
Cell fusion process feasibility and DRCC generation were evaluated using FC and CM. DRCC administration followed our established systemic-intraosseous injection protocol, 13,17 –19 with dosage determined based on previous studies. 15,19
Applying an experimental Lewis rat model of TBI, we initially assessed survival rates. While all control group rats died by day 10, rats in the other experimental groups survived until the study endpoint, demonstrating the need for bridging rescue therapy, as confirmed by the efficacy of the administered cell therapies, including DRCC. These findings are consistent with available scientific literature, which indicates that doses exceeding 7 Gy can be lethal for rats. 30 –32 Therefore, these results highlight the efficacy of the DRCC therapy in enhancing survival rates following TBI.
Furthermore, despite initial weight loss, all experimental animals regained weight, with those treated with isoBMT showing the fastest weight recovery. In addition, the body posture, activity, and fur condition were most similar to normal in rats treated with DRCC therapy, either alone or combined with alloBMT, when compared to alloBMT alone. These results confirm the tolerogenic impact of DRCC therapy, in contrast to the unfavorable clinical outcomes linked to the allogeneic properties of the alloBMT administration.
All experimental groups exhibited rapid leukocytopenia, lymphocytopenia, granulocytopenia, and monocytopenia post-irradiation. However, from day 20 onwards, significant increases in WBC, lymphocyte, monocyte, and neutrophil counts were observed in all treated groups, particularly in the DRCC therapy, highlighting the positive impact of DRCC transplantation on peripheral blood cell reconstitution. These findings are consistent with our previous studies, confirming hematopoietic recovery in rats following 7 Gy TBI. 21 In addition, testing chimeric cell phenotype confirmed the expression of hematopoietic (CD45), B cell (CD45RA), and myeloid cell (CD11b/c, OX-82) markers in DRCC, 9,10,19 affirming their capacity for multilineage chimerism induction compared to alloBMT. Scientific literature suggests that RBCs and PLTs, lacking nuclei, are relatively resistant to irradiation, 5 a trend confirmed in our study. However, while RBC, HGB, and HCT levels remained stable across all treatments, PLT counts fluctuated notably. Following an initial decline, PLT values gradually increased, with the most significant boosts seen in the DRCC group by day 20 and the alloBMT+DRCC group by day 60. These findings are consistent with previous research indicating DRCC’s ability to differentiate into progenitor and myeloid cells, supporting their positive impact on PLT recovery. 10,33
Moreover, histopathological analysis revealed minimal GvHD changes in rats treated with DRCC or alloBMT+DRCC therapy, contrasting with more pronounced changes in rats treated with alloBMT alone, affirming the safety profile of DRCC therapy.
Although this study used a rat model, which has inherent differences in hematopoiesis compared to humans, presented findings confirm the beneficial effect of DRCC on peripheral blood parameter recovery. Therefore, due to the tolerogenic properties and low immunogenicity, DRCC may serve as a valuable, bridging therapy until the HLA-compatible donor becomes available.
Conclusions
This study demonstrated the potential of DRCC therapy not only in ameliorating the adverse effects associated with BMT but also in attenuating the acute manifestations of TBI and preventing GvHD. Therefore, DRCC therapy emerges as a pioneering and innovative bridging therapy to advance the management of ARS and other irradiation-induced injuries, applicable to the field of stem cell research and regenerative medicine.
Footnotes
Acknowledgments
The authors thank Joanna Cwykiel, PhD, and Rafal Gendek, MD, PhD, for technical support and data acquisition, the staff members of the Radiation Safety Department of the University of Illinois at Chicago for the technical support, as well as the staff members of the Biological Resources Laboratory at University of Illinois at Chicago for technical assistance with processing blood sample analysis. The authors thank Andres Martin Acosta, MD, from the Department of Pathology at the University of Illinois at Chicago for conducting the histological assessment of tissue samples. We thank the staff members of the Flow Cytometry Core at University of Illinois at Chicago for technical assistance with acquisition of flow cytometry data. The authors would like to thank the BioRender software (RRID: SCR_018361) service, which was used to create Figures 1b and ![]() .
.
Authors’ Contributions
M.S.: Conceptualization, funding acquisition, project administration, resources, supervision, validation, and writing—review and editing. K.B.: Data curation, formal analysis, investigation, methodology, project administration, and writing—original draft. K.S.: Data curation, formal analysis, visualization, writing—original draft, and writing—review and editing. M.C.: Data curation, formal analysis, investigation, methodology, project administration, and writing—original draft. L.C.: Formal analysis, visualization, writing—original draft, and writing—review and editing. K.K.: writing—review and editing.
Author Disclosure Statement
The authors do not have any relevant financial or nonfinancial interests to declare that are relevant to the content of this article. In addition, the authors have no conflicts of interest to disclose.
Funding Information
This work was supported by the