
Abstract
There are multiple methods to prepare lipoaspirate for autologous fat transfer; however, graft retention remains unpredictable. The purpose of this study was to compare the cellular and protein composition of adipose grafts and the stromal vascular fraction (SVF) resulting from three common techniques to prepare adipose grafts. Adipose grafts were harvested from healthy donors and processed via three techniques: centrifugation (C), a single-filter (SF) device, and a double-filtration (DF) system. Part of each graft was analyzed or further processed to isolate the SVF. Cell viability, surface markers, cytokine, and growth factors were compared between the graft and SVF as well as adipose-derived stem cells (ASCs). Overall, we found variations across the three processing techniques and among the graft components (ASCs, SVF, and fat). Cell viability within the grafts was similar (94.6%, 92.3%, and 93.6%; P = 0.93). The trend was a greater percentage of ASCs from SF versus DF or centrifugation (6.95%, 4.63%, and 1.93%, respectively, P = 0.06). Adipogenic markers (adiponectin and leptin) were similar among all three grafts (P = 0.45). Markers of tissue remodeling were greatest in the SVF compared with fat and ASCs, regardless of processing technique. There was higher relative expression of MMP-9 (2×), Extracellular matrix metalloproteinase inducer (EMMPRIN) (2.5×), endoglin (5×), and IL-8 (1.5×) in the SVF (P < 0.005). Our study identified differences in cytokine expression in adipose grafts and the SVF, particularly in cytokines important in inflammation and wound healing. These secretomes may impact graft retention and fat necrosis and have the potential implications in cell-assisted lipotransfer. There were no significant differences between the final products of any of the processing techniques.
Introduction
Autologous fat grafting is a commonly used procedure in soft tissue reconstruction and augmentation. 1,2 In addition to the structural benefits of fat grafting, there is evidence to support a regenerative effect of prepared adipose grafts, though the underlying mechanism is poorly understood. It is well established that the adipose tissue stroma contains a variety of functionally rich cytokines, growth factors, immune cells (such as macrophages), and progenitor cells, commonly known as adipose-derived stem/stromal cells (ASCs). 3 –5 These “non-adipocyte” functional components can be isolated from adipose tissue or lipoaspirate as the stromal vascular fraction (SVF, Fig. 1). Thus, the reparative effects observed after fat grafting, particularly after breast cancer treatment, such as improved tissue quality, reduced fibrosis, and reduced pain, are thought to be because of the SVF. 6 –9

Illustration of adipose graft components including mature adipocytes, adipose-derived stromal or stem cells (ASCs), macrophages, neutrophils, endothelial progenitor cells, and fibroblasts.
Despite the clinical benefits of fat grafting, current procedures are plagued by graft resorption, especially in suboptimal recipient tissues such as in previously irradiated tissues or scars. 10 There have been several methods developed to streamline the process or enhance the graft during preparation, but there are several steps in the grafting procedure that may have an impact on graft retention or “take.” Graft preparation refers to the processing of the lipoaspirate to purify the tissue for injection and commonly consists of centrifugation, decanting, washing, or filtration, among others. Harvesting the tissue, preparing the lipoaspirate for transfer, and delivery of the graft to the recipient site are all areas of focus to improve engraftment. With this in mind, a review of grafting methodology is beyond the scope of this article, but several reviews have been published. 11,12 Outside of minimal manipulation, graft preparation may include the supplementation of the graft with growth factors, platelet-rich plasma, SVF cells, or ASCs, though these are all restricted to Investigational New Drug/Device applications under Food and Drug Administration (FDA) guidelines. 13,14 Nevertheless, graft preparation will undoubtedly be a means to manipulate the tissue graft to optimize a regenerative effect for targeted tissue therapy. 15
In the meantime, there is no standard technique that has been shown to be superior, 16 and translational data continue to be imperative in understanding the functional capacity of purified adipose grafts. To this end, the purpose of this translational study was to characterize the grafts produced from three commonly used processing methods as well as the resulting SVFs and purified adipose-derived stem/stromal cells.
Methods
Adipose samples
Two healthy women who underwent autologous fat grafting as part of their breast reconstruction following risk reduction prophylactic mastectomy were included in this study. Of note, none of the participants had history of cancer or breast cancer genetic mutation. The study was approved by the University of Texas Institutional Review Board, and consent was obtained for using deidentified, discarded tissues.
Surgical procedure
All participants were under general anesthesia in the operating room as part of their reconstructive procedure. At the time of fat grafting, tumescence solution was infiltrated in the abdomen and flanks per surgeon’s preferred technique (1 L of lactated Ringer’s solution, 30 mL 1% lidocaine, and 1ampule 1:1000 U epinephrine). This was given ∼10 min to take effect. Through the same infiltration site, the liposuction cannulas were introduced. First, 3-mm diameter cannulas connected to 10 cm3 Luer lock syringes were used to obtain fat from the lateral flank for centrifugation per standard Coleman technique. Next, the same cannulas connected to 60 cm3 syringes were used to obtain fat from the opposite lateral flank and the lipoaspirate transferred to a Puregraft250TM system which contains a double-filter (DF) bag. Finally, similar cannulas were connected to the liposuction machine, and fat was harvested using the RevolveTM system, which is comprised of a single-filter (SF) device. Graft preparation proceeded per protocol as previously described. 16 All three techniques were performed per patient. The authors obtained prepared graft via each technique and sent immediately to the lab for analysis.
Stromal vascular fraction preparation
To analyze the SVF, one 10 mL syringe of graft per technique was processed with collagenase digestion as previously described. 17 The resulting heterogenous mix of cells was suspended in phosphate-buffered saline and split for use in fluorescence-activated cell sorting or protein analysis as described below.
Fluorescence activated cell sorting (FACS)
Cells were incubated with 10 μL of Fc receptor blocking agent in the dark for 15 min at 4°C. Surface antibodies included: CD14, CD31, CD34, CD45, CD73, CD105, CD163, CD206, and Human leukocyte antigen–DR isotype. Triplicate data were acquired by using BD LSRFortessaTMCell Analyzer (Becton Dickenson Biosciences, Franklin Lakes, NJ) flow cytometer and analyzed using FlowJo software.
Protein analysis
For the graft samples, 100 mg of tissue was weighed and frozen with liquid nitrogen. The sample was prepared with buffer and a sonicator and placed on ice. Next, it was centrifuged at 12,000 rpm for 10 min to remove cellular debris. A similar-sized tissue graft was subject to collagenase digestion, and the SVF was treated with buffer and high-velocity centrifugation. A pure population of 1 × 106 cultured ASCs expanded to passage 4 was used from controls. One hundred micrograms of lyste were then used for consistency. Protein concentration from the resulting supernatants was measured using the Proteome Profiler Human XL Cytokine Array Kit (R&D Systems, Minneapolis, MN, USA). The images were analyzed using ImageJ software. 18
Statistical analysis
All experiments were performed in triplicate. Data are shown as mean percentage of surface marker expression or relative protein expression (compared with pure ASCs concentration as the referrent). All analysis was performed using SAS statistical software version 9.1 (SAS Institute, Inc). Results with a P value < 0.05 were considered statistically significant.
Results
Fluorescent activated cell sorting
Processed adipose graft and their corresponding SVFs were analyzed for each technique and compared with pure ASCs for reference (Fig. 2). FACS analysis is shown in Figure 3 and demonstrated comparable cell viability in the SVF among the three techniques (Table 1; 94.6%, 92.3%, and 93.6%; P = 0.93). When we looked at progenitor cell markers, namely the presence of CD73 and CD105 in the absence of CD14 and CD31, the trend was toward a greater percentage in the SVF from a SF device compared with a DF system or centrifugation (6.95%, 4.63% and 1.93%, respectively, P = 0.06). CD14+ monocytes were prevalent in all samples, and while these cells largely exhibited the presence of CD206+ among all processing techniques, the proportion of CD163+ expression was higher in the SF processing compared with double filtration and centrifugation (47.2%, 22.8% and 36.2% of the CD14+ pool, respectively; P < 0.05). CD14+ cells that did not express CD206 or CD163 (proinflammatory) were similar among the grafts (44.2%, 50%, and 43.4% of the CD14+ pool, respectively, P > 0.05).
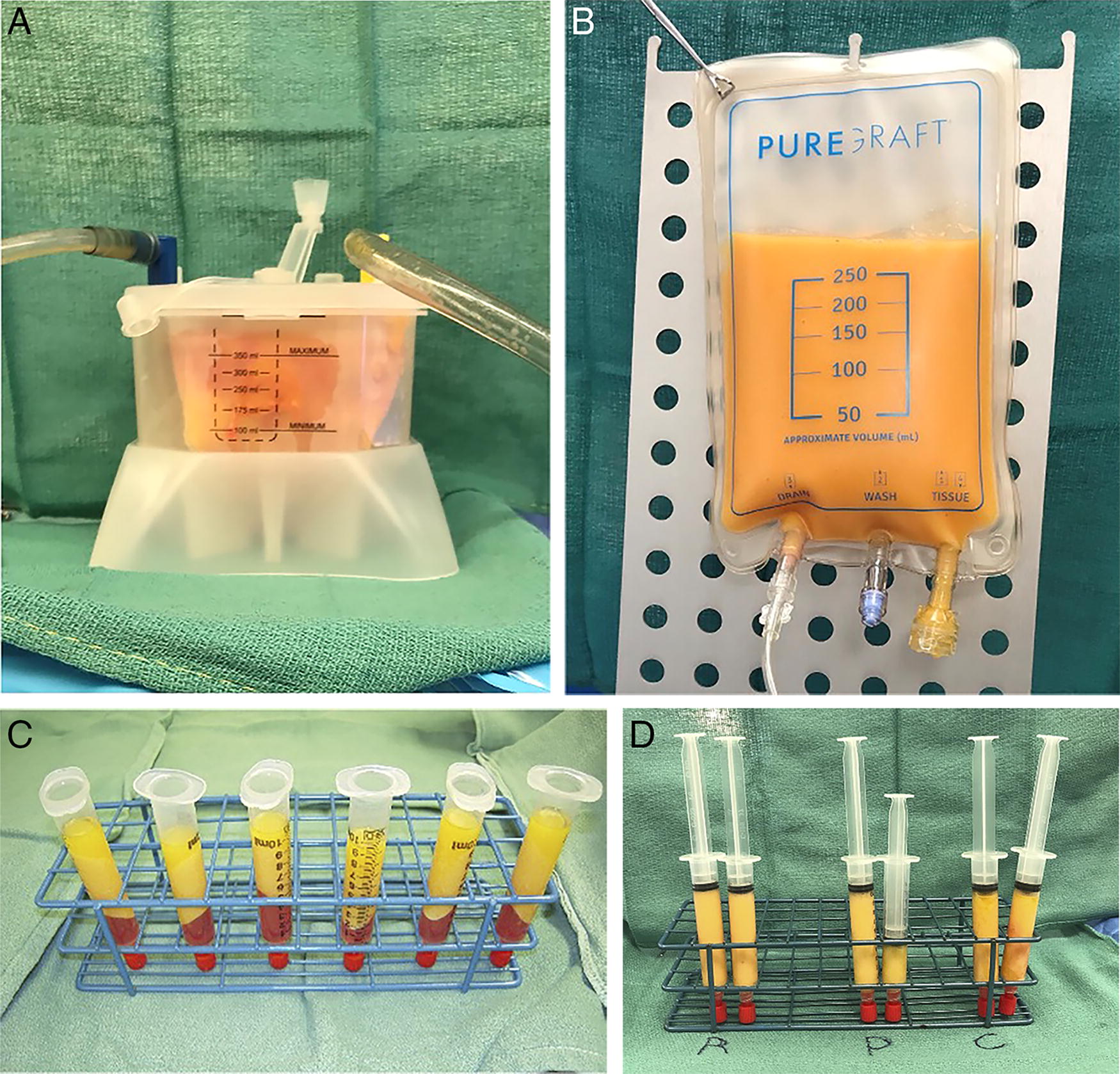
Representative photographs
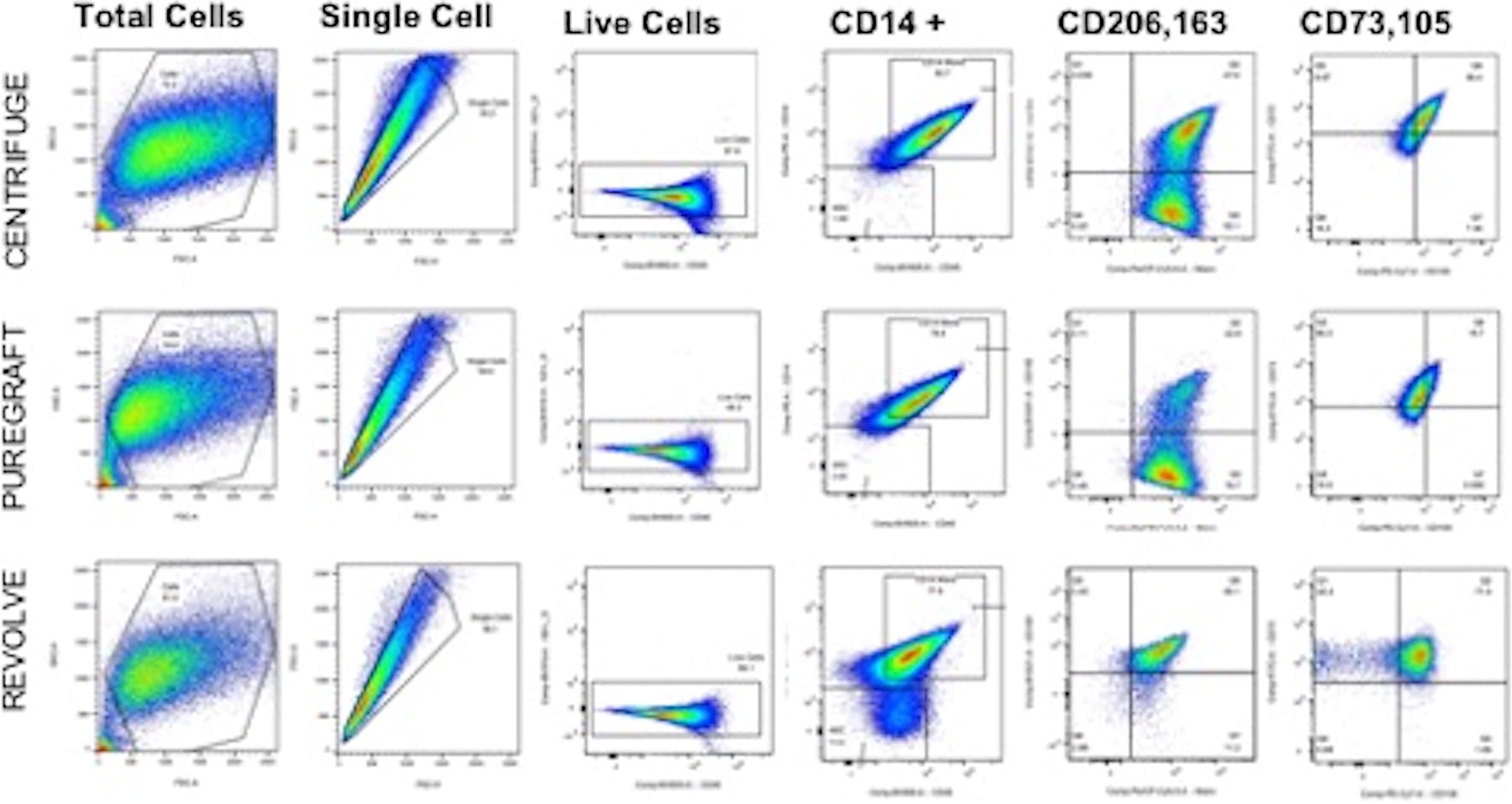
Fluorescent-activated cell sorting (FACS). Gating strategy and isotype control panels for CD14+ cells also expressing CD163 or CD206. Progenitor cells were identified through expression of CD73+ and CD105+.
Summary of Cell Viability, Progenitor Markers, and Macrophage Phenotype in Processed Adipose Tissue Grafts from Three Commonly Used Techniques.
Table 1. Summary of Graft FACS Analysis
DF, double-filter; FACS, fluorescent-activated cell sorting; SF, single-filter.
Protein analysis
Overall, we found statistically different protein patterns in the processed adipose grafts compared with the SVF and pure, culture expanded ASCs (Fig. 4). When we compared within the types of samples to determine a difference based on processing technique, there was some variability described below; however, there was no statistical difference in any of the cytokines or growth factors isolated within the graft or the SVF based only on processing technique. A summary table is included, and all values are of expression relative to the pure population of ASCs (Table 2).
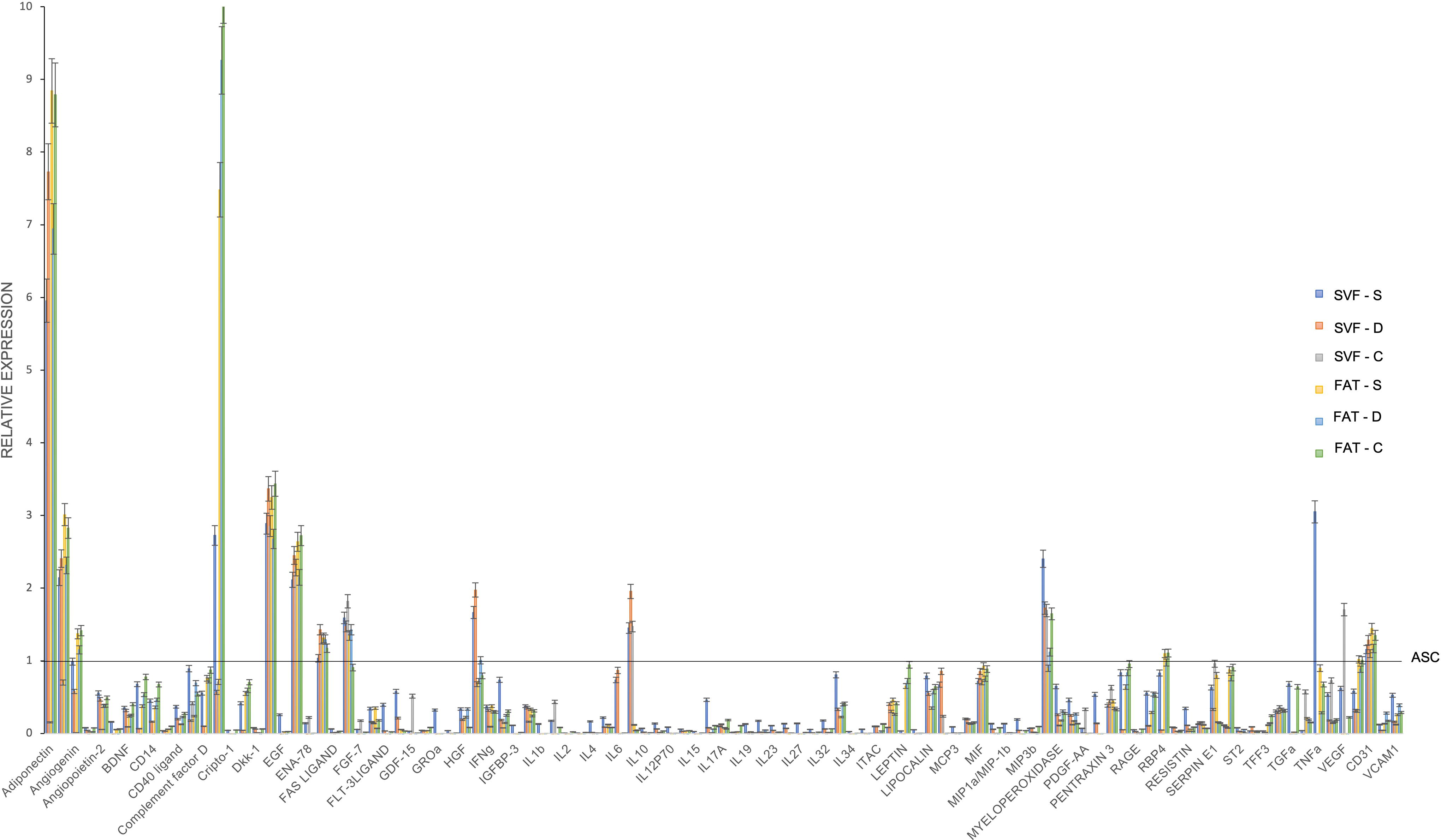
Relative expression of proteins in adipose grafts (FAT) and the resulting stromal vascular fraction (SVF) from three different processing techniques including a single-filter device (S, Revolve TM), a double-filter system (D, Puregraft 250), and centrifugation (C). Expression from pure ASCs is indicated by the horizontal line at 1.
Summary of Secretome Patterns of Interest Comparing Adipose Components and Processing Techniques
Significance P < 0.05.
ASC, adipose-derived stem/stromal cells; C, centrifugation; CRP, C-reactive protein; DF, double filtration system (Puregraft); FGF, fibroblast growth factor; HGF, hepatocyte growth factor; ICAM, intracellular adhesion molecule; IFN, interferon gamma; IL, interleukin; MMP-9, matrix metalloproteinase-9; SF, single filtration system (Revolve); SVF, stromal vascular fraction; TGFb, transforming growth factor beta; TNFa, tumor necrosis factor alpha; VEGF, vascular endothelial growth factor.
Adipogenic markers
Proteins that demonstrate functional adipogenesis were similar among all of the processed grafts. There was no difference in the concentration of adiponectin subtypes or leptin in the graft product. These proteins were found in minimal concentrations in the SVF or pure ASCs.
Vasculogenic proteins
Angiogenin, CD31, and vascular endothelial growth factor (VEGF) were used as markers for vasculogenesis. CD31 is a surface marker expressed on endothelial cells, and its concentrations were similar among all adipose graft and SVF samples. Angiogenin, a potent stimulator of angiogenesis, was similarly expressed among all samples, with slightly higher relative expression in grafts and slightly lower in SVF compared with ASCs though this did not achieve statistical significance (P = 0.06). VEGF concentrations were slightly higher in the SVF and adipose graft processed via centrifugation and relatively low in both of the filtration systems, with the highest expression being in pure ASCs. There was essentially no difference in the VEGF expression in the SVF or fat obtained through filtration. An unexpected finding was a fourfold higher expression of endoglin in the graft and SVF samples compared with pure ASCs. Endoglin plays a role in endothelial regulation and angiogenesis. 19
Markers of inflammation
C-reactive protein (CRP) was found in similar concentrations in the adipose grafts from the three techniques. However, concentrations in the adipose grafts were nearly 10 times higher (7.4–10.3 × RE) than those in the corresponding SVF (P < 0.0005), pointing to the inflammatory properties of fat in situ. Conversely, IL-8 expression was significantly higher among the SVF samples and pure ASCs compared with the adipose grafts (P < 0.05 for both). EMMPRIN expression was nearly three times higher in the SVF and graft (all techniques) compared with the ASCs (P < 0.005). EMMPRIN has been implicated in both inflammation homeostasis as well as matrix remodeling.
Tissue regeneration and repair
In addition to EMMPRIN, proteins such as hepatocyte growth factor (HGF), fibroblast growth factor (FGF), and matrix metalloproteinase 9 (MMP-9) were similarly variable between samples. FGF was comparably high among all processing techniques in adipose grafts and SVF, both with higher expression than pure ASCs (P < 0.05). Concentrations of HGF were similar in the SVF and grafts prepared with the filtration systems but seemingly negligible in the samples prepared through centrifugation. HGF was significantly higher in the pure ASCs (P < 0.005). MMP-9 was highest in the SVF compared with ASCs (2× RE, P < 0.05) and similar to fat (P = 0.10), with no difference among processing techniques.
Discussion
The number of autologous fat grafting procedures continues to increase in the clinic and indications are also expanding beyond structural support to capture the regenerative potential of adipose tissue. Still, graft take or retention remains an unpredictable outcome of the surgical procedure, and the regenerative mechanisms are not fully understood. Furthermore, given the variety of means to harvest, process, and deliver the adipose graft tissue, there are no universally accepted superior techniques or best practices. Several devices to streamline the process of graft preparation are on the market. 20 Thus, it is critical to fully evaluate the composition and functional properties of graft products for each of these techniques, particularly when discussing use in an oncologic setting. To this end, the authors performed an analysis of cell viability, percentages, and relative protein expression in adipose grafts and their corresponding SVF prepared from three different commonly used processing techniques from healthy participants. While overall cell viability was the same, there are different products yielded from each device or technique in terms of cell types and functional proteins detected. Ongoing studies are underway to determine the clinical relevance of these findings.
The indications of autologous fat grafting continue to expand, and future directions will undoubtedly include supplementation of the graft. 15 When considering standard grafting techniques, outside of supplementation, we demonstrate an overall similar cell viability among all processing techniques and similar progenitor cell populations. The clinical relevance of the variability in the actual graft product yielded by each of the three techniques investigated here is not known. While focus should be made on the delivery of the graft to optimize take, the choice of processing technique is frequently determined by cost, convenience, and surgeon preferred method. 12,21 When it comes to additional processing with minimal manipulation, such as microfat or nanofat, removing the structural adipocyte component could theoretically concentrate the regenerative proteins and progenitors but not beyond what is found within the tissue in situ.
There is debate in the translational literature regarding the optimal enhancement in these engineered grafts, particularly a pure population of ASCs versus the heterogenous SVF. 22,23 From a logistical standpoint, using the patient’s own SVF within the same surgical procedure minimizes the additional cost, processing, time, and potential risk compared with purified ASCs. 13,14 To adequately answer this question, further preclinical and well-designed clinical studies need to be performed. 24 The data obtained in this study demonstrate the different characteristics of processed grafts, SVF, and pure ASCs that could direct specific functionalities in the setting of cell-assisted lipotransfer. For example, filtration yields a graft with less free lipid or cellular debris compared with centrifugation; combine this finding with the higher concentrations of reparative proteins EMMPRIN, endoglin, and MMP-9 found in the SVF isolated from filtration that can occur in the same surgical procedure and one could design a protocol to proactively promote tissue repair, as in the case of radiation injury. Many proteins may affect more than one pathway during engraftment, and our lab is actively working through this orchestrated mechanism. For example, endoglin has been shown to promote angiogenesis but in a manner that regulates vessel formation. 19 Beyond endothelial endoglin, data suggest an effect on epithelial proliferation. In particular, with breast cancer models, endoglin may have a tumor suppressive effect. 25 EMMPRIN was first of interest for its role in tissue remodeling and induction of MMPs; however, the protein has also been shown to recruit cells to the site of inflammation and development and activation of T cells, which may have downstream effect in multiple pathologies, including cancer and autoimmune dysfunction. 26 As we are clinically expanding cell-assisted lipotransfer techniques, understanding these differences will be critical in designing targeted therapeutic grafts. 15
There are several limitations to this study to discuss. The authors included two healthy participants who were of similar age, body mass index, and overall health in order to limit participant variability. In reducing the variability in patients, the study does not account for differences that may arise in patients with comorbidities, medications, or external factors that may affect adipocytes or stromal cell function. For graft preparation, the instructions were followed per manufacturer’s directions and therefore the grafts were of different consistency. We are all aware that filtering longer will take some of the additional fluid off, effectively concentrating the graft. Conversely, retaining more liquid or having a less viscous graft will make it easier to inject; however, that could mean fewer cells within the sample as well as more fluid resorption translating to less perceived graft take. In essence, the quantitative assessments obtained here will only apply to grafts processed according to the manufacturer’s directions.
The samples analyzed in this study were produced in the same surgical procedure and enzymatically digested to yield a purified SVF pellet, a technique that is designated as more than minimal manipulation by the FDA. While this is an interesting starting point, ongoing work in our lab includes similar analysis with mechanical processing to microfat and nanofat, as well as in vitro work looking at the changes that occur in the setting of engraftment, or cell supplementation over time as opposed to time point zero in the current study.
Conclusions
As use of autologous fat grafting is increasing and the field is moving toward more advanced regenerative therapeutics such as supplemented grafts, it is necessary to thoroughly investigate the composition and functional properties of product yielded with different lipoaspirate processing. While there were many similarities in cell populations and proteins, our study identified differences in cytokine expression both in the graft and the associated SVF, particularly with proteins that play a major role in inflammation and wound healing. We do not know the exact impact of these secretomes on graft retention or fat necrosis; however, these differences may have direct implications in the clinical utility of cell-supplemented engineered grafts.
Footnotes
Acknowledgment
The authors thank Veena Papanna for assistance through the Advanced Cytometry & Sorting Facility at MD Anderson Cancer Center. This ACSF was supported by NCI P30CA016672.
Author Disclosure Statement
The authors have no financial conflicts of interest.
Funding Information
This work was funded in part by the