
Abstract
A human stomach is an organ in the digestive system that breaks down foods by physiological digestion, including mechanical and chemical functions. The mechanical function is controlled by peristaltic waves generated over the stomach body, known as antral contraction waves (ACW). The stomach's physiological digestion is essential to sustain nutrition and health in humans. Replicating the digestion process in a robot provides a test environment as an alternative solution to in vivo testing, which is difficult in practice. Stomach robots made of rigid rods and metal cylinders are unrealistic replicas to contract and expand like biological examples. With soft robotics technology, it is possible to translate biological behavior into an engineering context. Soft robotics introduce potential methods to replicate peristaltic waves and achieve a soft-bodied stomach simulator. This work presents a soft robotic stomach simulator's (SoRSS) concept, design, and experimental validation. A pneumatic bellows actuation for linear elongation and a ring of bellows actuation for circular contraction are proposed first. Multi-ring actuators are then arranged to form an SoRSS that generates ACW and antral contracting pressure (ACP). The SoRSS satisfies the specification of human stomach anatomy and motility and finally undergoes experimental validation using videofluoroscopy with the outcomes presenting the ACW, ACP, and the digestion phases during the actuation process. Those are compared with other medical studies to validate SoRSS functionality.
Introduction
The soft robotics field can mimic biological motion with soft actuators. 1 Several soft robots simulate or assist the functionality of human organs such as the heart, 2 esophagus, 3 and stomach. 4 However, stomach robots are still primitive in replicating the stomach's peristalsis (a series of circumferential contractions) and the physiological digestive phases. Stomach robots simulating the peristaltic waves are required for food technology.5–7 The stomach robot serves as a test environment for designing and testing novel food types and medical drugs.8,9
A novel surgical capsule-endoscopy requires a testing robot that is anatomically and functionally correct compared with its biological counterparts.4,10 Recent developments of stomach pacemakers open another demand for stomach robots as the test environment.11,12 Although newly discovered stomach diseases are still under research, a stomach-like robot can help researchers apply concept solutions for stomach disorders.
A healthy stomach undergoes a series of rhythmic peristaltic waves known in the medical literature as antral contraction waves (ACW). 13 The contraction morphology is characterized by specific physical measures, including pressure, frequency, and amplitude.14,15 These measures determine the quality of mixing, grinding, and emptying the stomach content. 16 The ACW is initiated from the pacemaker region, located in the stomach's upper body. The frequency of contractions is three cycles per minute, traveling from the pacemaker to the pylorus by the stomach's smooth muscles.
The average antral contracting pressure (ACP) of the stomach lumen (interior cavity) is measured between 45 and 90 mmHg. 17 The contractions are identified by the occlusion ratio, the ratio of the contracted diameter over the relaxed diameter of a single stomach's section. The ACW travel through the stomach body with an occlusion ratio that gradually increases up to 80% on average,18,19 also 100% of occlusion had been recorded. 20
Supplementary Table S1 in the Supplementary Data compares different stomach robots regarding the actuation method, body structure, and physical digestion phases during ACWs. In developing a stomach-like simulator, soft robotics techniques fit the intricate specifications of a human stomach.21–23 Several dynamic stomach simulators have been produced to duplicate the digestion of food in a human stomach for the food technology field.17,19,24–27 For example, a human gastric simulator was created to provide the ACW of a stomach. 19 The device consists of a latex layer with rollers placed over the layer pushing inward.
The indentations generate contractions with a frequency and pressure similar to a human stomach. The amplitude of contractions and the stomach shape were neglected. A dynamic gastric model was developed with a cone-shaped stretchable layer utilized to emulate the shape of a human stomach.24,25 The model applied pressurized water over the stretchable layer to achieve contractions. A cylinder and piston were coupled to simulate the mixing and grinding functions in a stomach. Another simulator is the TNO intestinal model, which consists of two adjacent glass units and flexible chambers inside the units.26,27
The units provided pressurized water, circling the chambers to push and mix the contents between the two glass units. These robots represent state-of-the-art stomach models and provide fundamental knowledge in this field. However, there is significant room for improvement regarding stomach anatomy and motility function that can be accomplished with soft robotics techniques.
A few stomach robots have been developed with anatomically realistic geometries.4,17,22 A silicone stomach model with metal ropes placed over the surface was developed as a test environment for surgical micro-endoscopic robots. 4 The robot's silicone body produces peristaltic motion by continuously pulling four metal ropes, actuated by DC brushed motors. However, the motion of pulled wires in just four sections of the robot's outer shape is unrealistic and not comparable with ACW. Another hybrid robot named the Gastric Simulation Model combines the gastric geometry and the peristalsis for food digestion research. 17
However, the peristaltic motion was not reported. In the previous work, we presented SoGut, a gastric simulator with seven soft ring actuators to simulate ACWs. 22 SoGut's soft actuators were designed in discrete sections. The continuous ACW in the robot lumen were difficult to achieve, which negatively affected the investigation of the physiology of the digestive phases. To overcome this obstacle, the specification of the ACW with the calculated amplitude and width of the traveling wave is required. A continuous contractable conduit design without decreasing the soft actuator is also necessary for providing a smooth and continuous ACW.
To the best of our knowledge, there is no stomach robot that is entirely built from soft material analogous to the stomach anatomy and produces ACWs that provide the physiological digestive process.
This article proposes an in vitro soft robotic stomach simulator (SoRSS), including multiple soft rings of bellows actuators designed within a stomach frame and fabricated by soft robotics development techniques. The SoRSS provides a peristaltic actuation that simulates ACWs by regulating the actuation pattern. Its peristaltic pattern accommodates the transition and the mixing of the content within the robot cavity. The robot generates an occlusion ratio and antral pressure that are validated and compared with the medical literature.
As monitoring the SoRSS actuation is inaccessible with vision systems, its occlusion ratios are investigated by videofluoroscopy. Stomach contractions generate antral pressures that are examined by a catheter and pressure sensors. The digestion process is investigated and compared with a biological stomach by comparing their videofluoroscopy frames.
The Proposed Method of SoRSS
The specifications of ACWs were derived from the literature (Schulze, 14 Kong and Singh, 19 and Kwiatek et al 20 ). They represented the quantification of distal antral contractile motility. These specifications were applied in two soft actuators. The bellows-driven soft pneumatic actuator (SPA) 21 was developed to simulate the amplitude and width of the smooth muscles in the stomach. Subsequently, we developed a soft ring-SPA (RiSPA) 28 that has a number of single degree of SPAs being arranged in the circumference, which is able to mimic a stomach segment with the correct contraction specification and behavior of ACW.
In SoGUT, 22 a stomach segment was modeled by a soft ring actuator that has only a single pneumatic chamber 29 and this ring actuator may result in a random number of folds when being contracted under pressure and thus cannot guarantee the correct contraction specification needed for ACW.
A human stomach's specification is simplified into two parameters, the stomach's average geometry and the stomach lumen contraction. The stomach simulator's shape is based on the stomach anatomy. Different medical scanning techniques, such as magnetic resonance imaging 14 and computed tomography (CT), 30 can produce a realistic stomach image from X-ray films taken from patients. Researchers document the shape, volume, size, and wall thickness by scanning many participants. 13
We presented a 3D anatomically correct stomach model, 23 based on a model constructed by Du et al 30 from a CT image. SoRSS model was prepared in CAD software (CREO) by drawing the stomach's upper and middle curvatures, representing them by two polynomial equations. 23 The middle curve is equal to 300 mm, an average stomach length. We constructed a series of circles perpendicular to the middle curves and diameters that fit the stomach model, the largest at the fundus of 100 mm and the smallest at the pyloric gate of 15 mm. 31 The model's parameters are linked with the average specification reported in the literature, which are summarized and presented in Figure 1a. A 3D model with a volume of 1 L was constructed by adjusting the diameters of the 3D model circles, estimating a stomach's size after an average meal.

The concept of SoRSS compared with a human stomach body.
The stomach's contractions include low frequency, shallow tonic contractions in the upper stomach (fundus), and strong contractions in the lower stomach (ACWs). 32 The ACWs initiate three physiological digestive phases as presented in the literature. 13 The model was divided into different zones depending on the motility (Fig. 1a). The tonic contractions (in the fundus) are translated to a uniform contraction over Zone A. The ACW is split into four zones from the contraction initiation at the pacemaker (Zone B) to the termination before the pylorus at Zone E.
The pylorus (Zone F) works as a flow valve that opens and closes depending on the sequence of the ACWs. Those divisions adapt the division summarized by Jarrett and Glasgow on the biological stomach body. 33 The contractions magnitude and frequency were discussed by Kwiatek et al 20 and were represented by soft ring actuators.21,28
Figure 1b shows the biological stomach's specification translation to the engineering context with soft actuation distributed over an anatomically realistic stomach conduit. The actuation consists of 95 bellows-driven SPAs acting inward to contract the conduit. The bellows-driven SPAs are positioned with a ring design (as previously developed with RiSPA) 28 fitted over the stomach conduit. The distances between RiSPAs are measured from the median curve of the conduit.
The distances between every two adjacent RiSPAs are 20 mm in Zone A, and 10 mm in Zones B to F. Zone A distances are estimated, as the tonic contraction in that zone is shallow. The specification of ACWs suggests the distances in Zone B to F,20,21 where the average width of the ACWs is 10 mm. As the distances between Zone B to F are 10 mm and the bellows were designed with 10 mm in diameter to fit the ACW requirement, a phase-shifted design is necessary, allowing adjacent RiSPAs to scatter over the conduit uniformly without colliding.
Figure 1c shows a single RiSPA previously described. 28 The number of SPAs in a ring was previously calculated, which depends on the diameter of the actuator. 28 The angle between the SPAs is (β = 360/the number of SPAs in a ring). The phase shift angle is (α = β/2). Thus, a phase-shifted design turns every adjacent ring actuator by α angles. Figure 1d shows the fabricated SoRSS body with the pneumatic tubes. The characteristics of the zones in SoRSS are illustrated in Table 1, including parameters that simulate a stomach's segmentation. Supplementary Table S2 in the Supplementary Data compares a biological stomach and SoRSS regarding the anatomical and physiological features.
Soft Robotic Stomach Simulator Zones Characteristics
The material was selected according to the deformation behavior of the ACW, which we presented in two previous studies. The first study focused on creating a soft actuator that simulates the contraction of smooth muscles, 21 whereas the second study represented the development of an actuator representing a stomach segment and mimicked the stomach contractions. 28 The materials of SoRSS consist of elastomers for the soft layer (Ecoflex 00–30 and Slacker; Smooth-on, Inc.), polydimethylsiloxane for the frame (Sylgard 184 silicone elastomer; DOW), silicone adhesive for gluing parts (Sil-Poxy; Smooth-on, Inc.), and silicone pneumatic tubes (bore size 4 and 6 mm), which make the entire stomach simulator soft.
The fabrication of SoRSS incorporated 3D-printed parts (Prusa i3; Prusa Research, Czech Republic) for molding and casting techniques. The CAD files of the moulds were designed in CREO (PTC). The bellows' geometries were specified in previous work. 21 Figure 2shows the fabrication and assembly process of SoRSS.
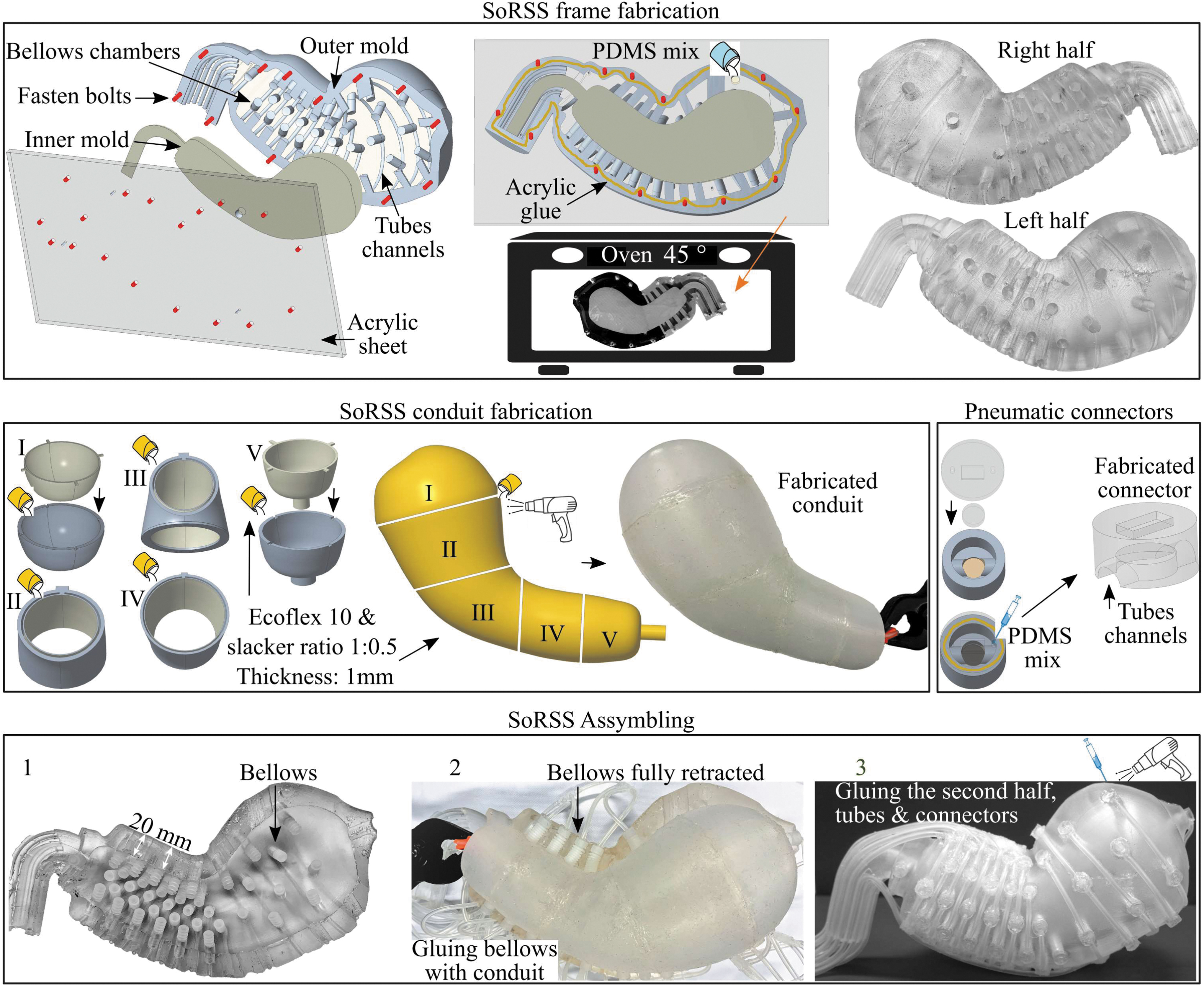
The fabrication of three parts of SoRSS: the frame, the conduit, and pneumatic connectors. The frame is fabricated into two halves. The conduit is fabricated into five sections, and then all sections are glued with the same material mix and a heat gun for material consistency. The pneumatic connectors are fabricated for each bellows (95 connectors). The assembly of SoRSS begins with installing bellows in the chambers while silicone glue is applied (1). For the first half of the frame, temporary pneumatic plugs are fitted to the installed bellows, and vacuum pressure is supplied to retract all bellows. Silicon glue is applied to the retracted bellows' caps; then, the conduit (filled with air) is placed on the first half of the frame over the bellows' caps (2). The second frame follows steps (1) and (2). Both frames adhered together (3). Finally, the fabricated pneumatic connectors and silicone pneumatic tubes are attached to the frames. PDMS, polydimethylsiloxane.
The SoRSS platform was designed to be portable for the clinical validation experiment outside the lab. The robot body was elevated on a platform for the videofluoroscopy experiment (Fig. 3a). The electro-pneumatic system consists of five proportional valves (three positives and two negative valves, ITV00 series; SMC, Japan), thirteen 3/2-way solenoid valves (005 series; Koganei, Japan), a vacuum generator (ZK2A10K5TL-08; SMC), a controller that uses LabVIEW scripts (NI myRIO1900; National Instruments), and a custom electrical circuit.

The experiment setup of SoRSS.
Each proportional valve controls a single zone where the shallow contraction zones (tonic contraction) (Zone A) and ACWs after the pacemaker (Zone C) are controlled by two negative valves. The three positive proportional valves control the higher contraction zones (B, D, E). The distribution of the valves follows the specification to replicate correct ACWs with the stomach robot actuators (RiSPAs). The thirteen switch valves control the switching between layers of zones C to F. Figure 3b shows the connections of the electro-pneumatic system with SoRSS.
Experimental Setup of SoRSS
SoRSS performed experiments to evaluate the functionality by validating three aspects: the lumen antral contraction, ACWs, and the three digestive phases, which are discussed next.
SoRSS lumen contractions
The ACP in a human stomach is usually investigated at the antrum, where the lumen is highly contracted. Similarly, SoRSS's ACP testing was performed in zones D and E (middle and terminal antrum). A standard method to define ACPs in the medical field utilizes a catheter with a balloon at its end, which can be inflated. In this method, a catheter is inserted into the antrum and then inflated by a syringe. Pressure on the catheter balloon is induced by ACPs and measured by a pressure sensor connected to the catheter.
This method was used to measure SoRSS ACPs with a customized catheter equipped with LED light and a pressure sensor, as shown in Figure 4a. The catheter used in this work is a two-way standard specialty foley 10 mL (Bard Medical). The LED light assists of locating the balloon inside the lumen (Fig. 4b). The balloon was inflated with 10 mL of air. The catheter was inserted from the pyloric valve and then aligned to the center of the targeted zone. Each zone (D and E) is about 40 mm in length, and the catheter balloon is 20 mm in balloon length. The ACP's area was assumed to be uniform over the catheter balloon as the forces exerted by the same bellows geometries. The measurement of ACP was performed during the actuation of the stomach with the ACWs. The experiment was repeated five times for reproducibility. The sampling frequency was 20 Hz.

The experimental setup for the ACP
As the robot lumen is inaccessible, videofluoroscopy was used to quantify the robot's lumen (Fig. 4c). The videofluoroscopic device has a sampling frequency of 30 frames per second. These frames were edited with a customized MATLAB script and an image processing tool.
SoRSS lumen contents
SoRSS was filled with three liquids with different viscosities to serve as stomach contents for experimental purposes: water (thin), nectar-thick (mildly thick), and pudding-thick (extremely thick). The thickness (viscosities) levels were decided by the international dysphagia diet standardization initiative. The three contents were selected for their relative similarities to stomach contents. Also, they are medically used as food bolus for testing on dysphagic cases. The use of the three contents is to validate the proposed robot functionalities.
Nectar-thick and pudding-thick contents were made from a food thickener in powder form (Altrix Rapid Thickener; Douglas Nutrition Ltd.). The product manufacturer suggests the powder and water mixing ratio to produce nectar-thick (3.5 scoops [3.6 g] in 700 mL of water) and pudding-thick (14 scoops in 700 mL of water). The contents were quantitatively evaluated in the literature, where water is 0.001 Pa/s, nectar-thick is 0.325 Pa·s, 34 and pudding-thick is 1.36 Pa·s. 22 Barium liquid (Liquibar) was used as a contrast agent for videofluoroscopy examinations by mixing the agent of about 100 mL with the three prepared contents as recommended by the radiographers.
Peristaltic Waves Generation
To generate a peristaltic wave in the SoRSS lumen, we send a sequence of signals of input pressure to the robot's zones, which are divided by each zone's propagation speeds and occlusion ratios. Figure 5shows relative signals applied to the system. The biological stomach has an average of three ACWs that coincide with the stomach body, and they are repeated every 20 s. 32 Therefore, zones B, C, D, and E in SoRSS imitate a human stomach's ACWs with a continuous actuation every 20 s. The signal in Zone A is a sinusoidal wave to mimic the tonic contraction. The signal for zones B to D is a ramp function that increases the pressure from −75 to 100 kPa.

The applied signals to each zone in SoRSS. The applied tonic contraction of a sine signal
The pressure increases in ring actuators progressively, which increases the contractions on those actuators. A steady signal of 100 kPa is applied for all the layers in Zone E. The fast contractions between the layers in this zone imitate the fast stomach propagation in the terminal antrum. This peristaltic signal is represented by a piecewise function of Equation (1),
where f(t) is the input pressure, and t is time in seconds.
The maximum occlusion ratio examination was performed by specifying a single ring actuator located in each zone, which are A4, B, C4, D4, and E4. The pyloric valve (Zone F) was closed during the entire experiment to retain the contents. The peristaltic wave was pneumatically generated with the prescribed pressure for each zone in SoRSS. The tests were repeated three times for each liquid content.
To generate ACWs that occur in a biological stomach for experimental purposes, we coordinated the actuation sequence for multi-RiSPAs according to the medical literature that describes stomach motility.14,19 In the videofluoroscopic experiment, we ran the robot for five peristaltic waves (5 min) to analyze the recorded videos with the repeated cycles. The recorded videos from the experiment were processed by abstracting ten frames for each full cycle of the peristaltic wave.
During the peristaltic waves, three digestive phases occur in a human stomach: propulsion, emptying, and retropulsion. Videofluoroscopic videos were used to validate the three phases of digestion, as explained in the literature. 32 Those phases were examined when the robot was filled with pudding-thick content. Also, biological stomach digestive phases were compared with SoRSS by evaluating both videofluoroscopic results.
Results and Discussion
Input pressure
The results in Figure 6show SoRSS's responses relative to the input pressure to verify the actuation quality. The input pressures were measured by the valves' built-in pressure sensor. Zone A had a good response with a standard deviation of 2%. Also, Zone B had similar results with a 1.5% standard deviation. The low standard deviation indicates minimal air leakage during actuation. The leakage usually occurs from fabrication errors, and it is challenging to fix any leakage that occurs during the hospital experiments.

The results of the proportional valves in all zones to realize the quality of the actuation. The actuation signals from Zones B to E show each zone's lifespan, mimicking the peristaltic wave. The measured responses are obtained by the built-in sensors in the proportional valves.
In zones C, D, and E, each proportional valve had four switch valves controlling four layers in each zone. During the actuation between RiSPAs, some spikes occurred in the proportional valves' response while switching from a vacuum state to follow the specific zone's ramp function. The duration of these spikes is less than a second. This effect does not influence the actuator's overall performance, as the valves respond quickly. The standard deviation was 2%, 3%, and 10% for zones C, D, and E, respectively.
We considered the responses of zones C and D to be of good performance with minimal error. Four valves were switched on in Zone E simultaneously, adding a more significant pressurizing error. Thus, the proportional valve stabilizes all the leakage issues encountered with a stable state with an error of 5 kPa less than the required pressure. Therefore, the reference applied pressure was increased from 100 to 105 kPa to compensate for the input pressure error, while the required input pressure of 100 kPa was achieved.
Characterization of ACP
The results of ACPs are shown in Figure 7 as a function of time. The input pressures for zones D and E are also shown to realize the trend of the ACP. The ACP measurements were within the estimated measurements reported from a human stomach's medical literature between 45 and 90 mmHg. 17 In Zone D, the ACP increases after the ramp function of applied pressure with a spike from switching between layers in the zone. The ACP increases in Zone E until about 100 kPa (48 mmHg). The trend of the ACP in Zone E is similar to the one shown in Figure 6. As the pressure developed in the four layers of the zone over time, the pressure deviated between 45 and 48 mmHg.

The ACP of SoRSS in Zone D
However, this deviation is considered minor and does not influence the overall performance. The measured ACP also confirms the lumen contraction, which is challenging to comprehend with only the built-in pressure sensors of the proportional valves. From the results, SoRSS can simulate the ACP of a human stomach. Such functionality can aid in the mixing and emptying of the stomach contents.
Characterization of the maximum occlusion ratio
The ACWs' occlusion ratios represent how the stomach walls are changing regarding their diameters. The occlusion ratio is influenced by stomach contents, condition, and digestion phases. The proposed robot follows the stomach function by distributing occlusion ratios from 0% to 80% over the robot body. The selected frames from videofluoroscopy show the conduit's deformation inside the robot (Fig. 8a–c). The occlusion ratio is

The characterization of the occlusion ratio of each zone in SoRSS by selected layers: A4, B, C4, D4, and E4. These layers can be seen in Figure 1.
The middle and terminal antrums (layers D4 and E4) produce a maximum occlusion ratio of 78% and 82%, respectively. These results are like the reported function of a human stomach. The proximal antrum (layer C4) achieves the required response of about 40% with a standard deviation of 5%. It was noted that the maximum occlusion ratio of the nectar-thick content was unattainable as the visibility was inadequate. This is related to the barium-laced content that might be leaked between the conduit and the robot frame.
Also, Zone C has fewer SPAs that induce some challenges to film an apparent contraction with the applied horizontal setup of the X-ray. The results of layer C4 with the other contents are sufficient to identify the maximum occlusion ratio. Zone B and layer C4 results are under 20% of the occlusion ratio. The pyloric actuator in Zone F was fully actuated to keep the content in the robot's lumen during testing. The results slightly vary among the three liquid contents (Fig. 8g–i). The difference in the density of the three contents may influence the performance of the occlusion ratio, but there is no exact correlation between the occlusion and contents.
Emulation of the ACWs
The propagation of the SoRSS peristaltic wave to simulate ACWs of a human stomach is shown in Figure 9. The contractions start at Zone B and propagate downward to Zone E with a complete peristaltic cycle in 60 s. Each zone has a repeated contraction every 20 s. The ring actuators' responses in each zone are shown on the left side of Figure 9a, c, and e. The results show the propagation of the contraction over time. In Zone E, the applied pressure is a steady 105 kPa, while the actuators' responses increase with time. This response coincides with Zone E, influencing the proportional valve by providing a faster-regulated response.

The simulation of the ACWs in SoRSS. The ring actuators' responses in each zone are shown on the left column
Each zone's overall response is presented on the right side of Figure 9b, d, and f. The responses of the zones show the propagation of the contraction waves. The peristaltic contraction of the robot exhibits a similar pattern to the behavior of a human stomach ACW. The results validate that SoRSS can emulate the biological ACWs by applying regulated and overlapped pressure in SoRSS to generate contracting force, amplitude, and frequency. Therefore, SoRSS can serve as a test environment for digestion and food technology research.
Biomimicking the digestive phases
The results of the three digestive phases through empirical analysis are shown in Figure 10. Each phase consists of a model to illustrate each zone's sequence, a videofluoroscopic screenshot from a biological stomach (adapted from Ehrlein and Schemann 32 ), and a videofluoroscopic screenshot of SoRSS. The biological stomach screenshot and the Supplementary Video S1 illustrate and show the relative behavior of the robot with the biological example.

The replication of the three physical digestion phases during the ACW in SoRSS as compared with a biological stomach.
32
The phase of propulsion is illustrated in a model in
In the propulsion phase, Zone C contracts to transport the food to the middle and terminal antrum. In the second phase of emptying, Zone D starts to contract to propel the stomach content toward the terminal antrum and empty some of the contents while the pyloric is open. In the third phase of retropulsion, Zone E contracts faster than the other two zones, and all the layers in this zone are contracted simultaneously. This behavior creates a pumping pressure that mixes and grinds the content while pushing the remaining contents back to the stomach as the pyloric valve is closed.
We developed SoRSS to mimic an average healthy human stomach's functionality, and the controller follows a regular ACW. In Zone C (proximal antrum), the contractions appear slight, as the actuators in this zone are scattered around the greater curvature of SoRSS. In Zone D (middle antrum), the contractions are increased to push and empty the content while the pyloric valve is open (10 mm in diameter). In this zone, actuators are not fully retracted between cycles. This issue is related to the vacuum generator, which could not simultaneously manage all the actuators, mainly from the small leakages.
This issue can be resolved by applying sufficient vacuum to SoRSS. In Zone E (terminal antrum), the occlusion ratio is at a maximum of 80%, which forces back the remaining contents to the stomach conduit while the pyloric valve is closed. It was seen that some contents remained in a gap between E4 and the pyloric valve, where there is no actuator. This gap was followed by medical literature, as the ACWs end before the pyloric about 7 mm. 8 In SoRSS, the gap is 10 mm for the robot's consistency. SoRSS can simultaneously transport, empty, and force back stomach contents, mimicking all three digestive phases. These phases were validated by correlating the biological stomach with SoRSS as abstracted from literature.17,32,34
SoRSS consists of bellows-driven SPAs 21 and RiSPAs. 28 Both actuators established the fundamental actuation method for simulating the stomach contraction by translating the ACW specifications. The robot's design was abstracted from a medical scan of a human stomach and scaled with average anatomy to serve as an in vitro simulator to mimic the in vivo motility of the biological stomach. The soft layer in SoRSS assisted with the continuous peristaltic wave while RiSPAs were under actuation. This behavior shows the benefit of soft robots over rigid stomach models.
The advantages of SoRSS over previously developed SoGut 22 are the continuous ACWs and simulating the three digestive phases. SoGut has a limited number of actuators in the robot, providing discontinuous ACWs. The emulation of the digestive phases was not found in the previous stomach simulators. Therefore, it is a significant contribution that advances knowledge for digestion, food technology, and soft robotics.
SoRSS is an in vitro simulator that can perform testing for food technologies and present a new testing method for analyzing peristaltic simulators in soft robotics. The robot was controlled to generate a pattern of healthy ACWs. However, the controller can also be programmed to mimic disordered motility patterns. Therefore, SoRSS is customizable to generate a series of quantitative controllable patterns through the robot's soft actuators. Experiments of newly developed drugs and food for ill patients require a test environment that closely functions like a stomach. Another application that requires in vitro testing is endoscopic capsules to understand their performance in a dynamic stomach environment.
While soft robotics is in the fundamental stage of development, SoRSS can add to the field by implementing advanced available control techniques to achieve soft actuation that closely mimics human stomach contractions in a closed-loop manner. In addition, the design and functionality, such as peristaltic waves, can benefit the field.
For testing on SoRSS, the videofluoroscopic technique is excellent to measure the internal contraction of the robot. It is a valuable technique for enclosed robots that vision systems cannot characterize. A drawback of this method is the availability of such a device, usually found in hospitals. The environment and time are significant factors to be considered when experiments are performed in hospitals.
Conclusion
SoRSS was tested and validated by examining four aspects: the antral contracting forces, occlusion ratios, ACWs, and digestive phases induced by ACWs. The robot was validated and compared with medical literature to validate its similarity to a biological stomach. Results showed relative measurements to those found in the biological stomach. The generated ACWs present the physiological digestion phases of transporting, emptying, and grinding stomach contents. The evaluated results indicated that SoRSS could serve as a test environment for simultaneous measurable experiments.
The existing state-of-the-art stomach simulators were either rigid robots with unrealistic shapes or simulators with stretchable conduits replicating the contractions by rigid actuators. In both scenarios, these robots were not anatomically realistic, and the drawback was the inadequacy of research correlated to a stomach's in vitro testing. Although it is challenging to simulate stomach behavior and only a few stomach models are available in the literature, the previous studies of stomach robots provided the fundamental knowledge for this work.
The novelty of SoRSS can be illustrated by an entirely soft-bodied with realistic shape and functionalities comparable with the biological example. SoRSS benefits from soft robotics techniques to translate actual stomach specifications to a soft robotic setup that emulates the digestive phases through peristalsis patterns. Such functionality advances the soft robotics field by introducing soft actuators that mimic the stomach's smooth muscles via a series of radial contractions.
Despite the achievements of SoRSS, a few limitations were defined in the performance. SoRSS was validated with liquids of different viscosities, though solid foods have not been tested, and the influence of the contractions on the digestion of the food requires further investigation with the implementation of stomach juices. As the stomach is made of silicone and silicon is resistive to stomach juices, the implementation of stomach juices is applicable. Emptying functionality of solid and liquid contents needs further examination.
In addition, the absence of a stretchable sensor over the conduit restricts online assessments of the robot's lumen. The development of a stretchable sensor laid over the conduit can be the solution, but stretchable sensors are challenging to design. Moreover, although the peristaltic actuation was achieved with the current setup, the actuators' retraction was not fully attained, and another vacuum ejector could be applied. The robot was validated and compared with the medical literature to validate its similarity to a biological stomach. Our future work will focus on engineering research and clinical assessment to further validate the capability of the robot's functions as a simulator to investigate the human digestion process involving liquid and solid food boluses, including emptying the chyme.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.