
Abstract
Respiratory assistance is commonly used to treat respiratory system diseases or support postoperative recovery, playing a crucial role in patient rehabilitation. However, existing respiratory assistance devices rely on rigid systems, which may pose risks to the human body. To address this, we propose a novel soft abdominal compression robot for respiratory assistance (SACR-RA), which offers personalized and adaptive support. This novel ability is achieved by dynamically adjusting the pressure applied to the abdomen in real-time on the basis of the user’s respiratory characteristics. First, we developed a pressure-deformation model for soft pneumatic actuators and confirmed its accuracy through experiments. Next, we developed a human respiratory model that links respiratory assistance levels to lung conditions, enabling flexible adjustment of control strategies on the basis of the user’s condition. Accordingly, we designed respiratory pattern control and respiratory intensity control strategies to ensure adaptable support for the user’s respiratory needs. Finally, we validated the effectiveness of SACR-RA through respiratory flow and electromyography experiments. The results demonstrated that SACR-RA significantly improves the exchange of air between the user and the environment and reduces the burden on respiratory muscles.
Introduction
Typically, patients with respiratory disabilities receive treatment using ventilators, which deliver air directly into the lungs via an invasive airway tube or mask. 1 While these devices can provide the precise amount and flow of air needed, they often obstruct the patient’s oral cavity to introduce airflow. Additionally, they are typically limited to patients who can only breathe slightly or cannot breathe at all. 2 Current mechanical ventilators are not well-suited for supporting users in their day-to-day social activities. Moreover, when using these devices, patients must rely on caregivers in their daily tasks, and this increases their hygiene burden. 3 To better serve the needs of patients and reduce the impact of ventilators, respiratory assistance devices can be used for those who still have the ability of autonomous respiration.
Respiratory assistance devices involve the manual or mechanical application of intermittent pressure changes to the body, helping support the function of the inspiratory and expiratory muscles. These devices assist patients in achieving respiratory movements by generating pressure changes around the chest or abdomen. 4 The abdominal muscles play a crucial role in respiration, and without their assistance, patients must rely on their accessory respiratory muscles for respiration. 5 This may lead to a decrease in the volume of air exchanged during inhalation and exhalation, leading to a decrease in heart rate and metabolic rate, followed by symptoms such as hypotension and hypoxia. 6
To simulate the contraction of abdominal muscles and address the drawbacks of mechanical ventilators, researchers have extensively studied respiratory assistance devices that use abdominal compression. Sang-Yoep Lee et al. proposed a belt-driven respiratory rehabilitation and assistance robot, where abdominal pressure is applied via a tension belt controlled by motors around the abdomen. Abdominal contraction is facilitated by regulating the tension on the belt, which aids in the exhalation process. When the tension is released, inhalation occurs due to the body’s recoil and the pressure difference between the atmosphere and the lungs. 7 Zhu et al. assisted patients in movement via a two-degree-of-freedom respiratory training robot, which alleviated pain, reduced respiratory difficulties, and improved respiratory muscle performance. 8 However, the abovementioned rigid-body robots are driven by motors and involve rigid transmission of forces, so safety cannot be guaranteed in practical applications. Additionally, the psychological burden on patients of using these devices is high, and there are disadvantages such as high structural complexity and difficulty adapting to the human body.
To mitigate the risk of injury to the human body by rigid robots, advances in material technology, rapid prototyping techniques, and smart control technology have shifted the focus of robotics research toward soft robots that offer adaptability, safety, and efficiency. These soft robots are made from deformable and stretchable materials, enabling them to undergo large deformations, a large number of degrees of freedom, and advantages such as flexibility, lightweight design, high safety, and strong adaptability. They have found crucial applications in medical rehabilitation, including soft rehabilitation gloves, flexible exoskeletons, and active soft orthoses.9–13 These devices are suitable for daily rehabilitation exercises and help boost patient engagement in their recovery. 14 Moreover, these soft robots may be used to compensate for limited respiratory capacity without interfering unnecessarily with the patient’s body. However, current research on soft robots typically focuses on modeling soft actuators,15,16 whereas modeling the integration between soft actuators and the human body is often overlooked. This oversight may mean that soft actuators do not fully meet the rehabilitation needs of the human body. Additionally, the drive method used in soft actuators typically relies on implementing preestablished models for feedforward control, 17 which cannot be adjusted for the patient’s changing rehabilitation stages. This limitation is problematic for long-term patient use and makes it difficult to achieve the best rehabilitation outcomes.
To address the issues mentioned above, we propose a novel soft abdominal compression robot for respiratory assistance (SACR-RA). This device dynamically adjusts the pressure applied to the abdominal muscles, offering personalized and adaptive respiratory assistance. First, we introduce a new type of soft pneumatic actuator, and develop a pressure—strain model for individual actuators. These actuators are then combined to form the soft respiratory assistance device, which is designed to safely interact with the human body and apply pressure to the abdominal muscles. Next, we develop a model that links the control pressure of the actuators to the respiratory conditions of the lungs. By treating the abdomen as a sealed container, we design two control strategies: respiratory pattern control and respiratory intensity control. These strategies enable the device to flexibly adapt to the user’s respiratory needs, both in the short and long term. The respiratory pattern control method regulates the inflation and deflation of the device according to the user’s respiratory pattern, guiding the contraction of the abdominal muscles during exhalation and relaxation during inhalation. Meanwhile, the respiratory intensity control method employs a neural network to map respiratory flow parameters to pressure levels, achieving adaptive pressure adjustments over time. By incorporating these respiratory features with actuator pressure adjustments, the device provides intelligent and efficient respiratory assistance.
Our experiments confirmed the effectiveness of the SACR-RA for providing respiratory assistance. The device significantly improves user both exhalation and inhalation performance, facilitating air exchange between the user and the environment. Electromyography (EMG) measurements revealed a reduction in the burden on respiratory muscles when using SACR-RA, demonstrating its ability to effectively reduce muscle load.
In summary, SACR-RA is an innovative respiratory assistance device that offers effective support for patients with respiratory system impairments through its functional mechanical design and intelligent control strategies.
Design of the Actuator
Design of SACR-RA
During exhalation, the main factors influencing its effectiveness include the weight of the chest cavity, the contraction of the abdominal muscles, and the elastic recoil of the lungs. Among these, the abdominal muscles do not directly interact with the airways. Instead, they are attached to the lower ribs and influence the movement of the chest cavity. When the abdominal muscles contract, they pull the abdominal wall inward, causing the diaphragm to move upward into the chest cavity while also pulling the ribs downward, leading to the exhalation of air from the chest cavity. 18 Additionally, the abdominal muscles, as core components, control intra-abdominal pressure through coordinated action with the pelvic floor muscles, which plays a key role in the exhalation process. 19 Lander et al. suggested that externally compressing the abdomen with a belt increases intra-abdominal pressure, and applying pressure during exhalation can increase lung ventilation. 20 In this way, abdominal muscles assist in exhalation, and by considering their impact on respiration, compensatory forces can be applied to the abdomen to effectively assist respiration. However, current methods typically use rigid components to apply force to the abdomen, which can lead to significant risks of injury if not used correctly. To increase the safety of respiratory assistance, we designed SACR-RA.
SACR-RA consists of three axially expandable compression units, a set of inelastic waistbands, and adjustable ties, as shown in Figure 1. The compression units, which are the primary components, are designed as fully sealed bladders, as shown in Figure 1b. Each unit includes a silicone bladder (made from ELASTOSIL M 4601A/B, Wacker Chemie AG, Germany) and a longitudinally elastic fabric shell (made of polyester and latex). This fabric shell is knitted into a hollow cylindrical shape that wraps around the outside of the silicone bladder as a limiting layer. It stretches only axially and resists deformation in the tangential direction. The silicone bladder is sealed except for three air holes at the bottom, which are connected to air tubes. The end face of the bladder has a flange, and two platens are set on both sides of the flange to press the elastic fabric shell tightly and limit the expansion of the silicone bladder at the bottom. During inflation, the injected air causes the end surface of the compression units to bulge. The bladder undergoes axial elongation due to pressure, with no radial deformation because of the constraints imposed by the elastic fabric. This results in a compressive action on the human body. Each compression unit is mounted on an inelastic waistband made from PVC material (3A 1.5 mm PVC sheet, Shijiazhuang Yisi Qi Daily Chemical Co., Ltd, China), with adjustable ties at both ends, as shown in Figure 1a. The inelastic waistband ensures that, once the device is worn, the length of the SACR-RA does not increase with the elongation of the compression units, thus enabling the desired compression.

Structure of SACR-RA.
In the process of respiration, exhalation is an active process, in which different abdominal muscles are activated to varying degrees. The transversus abdominis muscle is the most active, followed by the obliquus internal abdominis and obliquus external abdominis. 21 Anatomical evidence shows that the four flat muscles: the rectus abdominis, obliquus internal abdominis, obliquus external abdominis, and transversus abdominis, play crucial roles in compressing the abdominal contents. These muscles also serve as accessory muscles for inhalation. 22 The fibers of the obliquus internal abdominis, obliquus external abdominis, and transversus abdominis are arranged in diagonal and radiating patterns. However, the transversus abdominis and obliquus internal abdominis are located deeper within the abdominal cavity, whereas the obliquus external abdominis is the outermost layer. To maximize abdominal contraction, we selected the obliquus external abdominis on both sides of the abdomen and the central rectus abdominis as the areas to apply pressure, as shown in Figure 1c. Before the device is used, it is essential to align the three compression units with the respective points by adjusting the ties, which enables exhalation assistance through abdominal compression.
Mechanical characteristics of SACR-RA
To drive SACR-RA, it is essential to model the mechanical characteristics of the compression unit, which can be divided into two main aspects: free elongation characteristics and blocking force characteristics. The free elongation characteristics describe the relationship between the elongation length l and the inflation pressure P when no external force is applied. The blocking force characteristics involve the forces exerted on the body once the compression unit contacts the body surface and undergoes deformation. This relationship is used to establish the connection between inflation pressure P and the output force F.
Free elongation characteristics of the compression unit
We divide the deformation of the compression unit under pressure into two parts: deformation on the top surface and deformation on the side surface, as shown in Figure 2.

Deformation of the compression unit in mechanical characteristics model.
We simplify the top surface as a circular membrane with a radius r0. The edges of the membrane are clamped, while the center is free to expand elastically, as shown in Figure 2a. Assuming that the deformation profile is represented by a surface
The compression unit of the SACR-RA is made from a hyperelastic material, and its mechanical characteristics are described by a hyperelastic model. According to Yeoh theory,
24
the first strain invariant is given by:
The strain energy is given by:
The volume enclosed by the circular membrane during the deformation process is given by:
To establish a relationship between the inflation pressure P1 and the height of the inflation of the circular membrane h, we apply the principle of virtual work:
The left-hand side of Equation (5) represents the virtual change in the total strain energy with respect to the inflation height, while the right-hand side represents the virtual work done by the inflation pressure. To account for manufacturing methods and process-induced errors, we introduce a compensation factor k = 0.75 to eliminate the impact of fabrication discrepancies across different actuators. Ultimately, we obtain:
Equation (6) establishes the relationship between the inflation pressure P1 and the height h of the top surface inflation. Figure 3a shows a comparison between the theoretical and experimental values. The model is fitted well at lower pressure levels, but the errors increase at higher pressures. Since our respiratory assistance device operates within a pressure range below 80 kPa, so the curve effectively captures the actuator’s behavior within this pressure range.
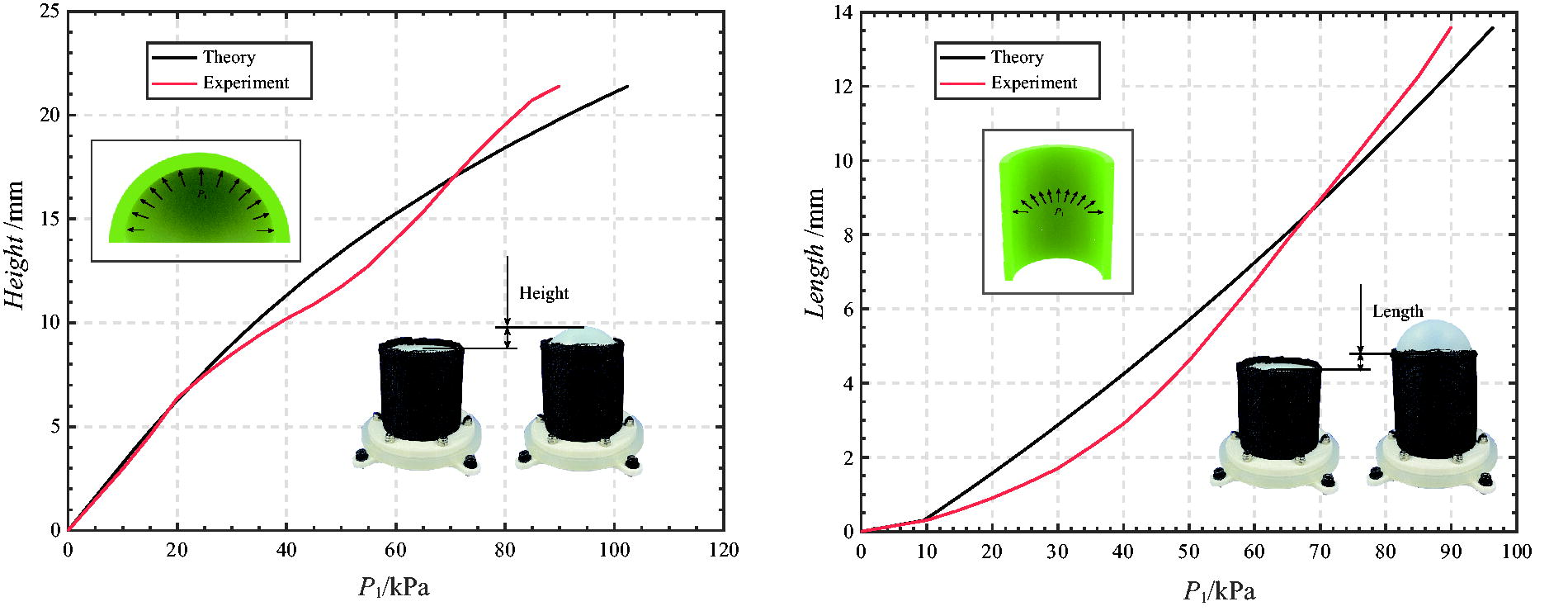
Performance evaluation and actual performance of the compression unit.
We simplify the side surface as a hollow thin-walled cylinder with an initial length l0 and initial thickness t0, as shown in Figure 2b. Let the radial, circumferential, and axial elongations of the side surface be denoted by
Since the confinement layer restricts the radial expansion of the actuator, the outer diameter r0 remains constant. Therefore, the circumferential elongation rate of the side surface
The strain energy function is given by
Since the deformation of each point on the side surface is approximately the same during the deformation process, the strain energy is also the same. Therefore, the total strain energy is:
By the principle of virtual work, we can obtain:
As with the top surface, we also compensate for variations in manufacturing methods and process errors via a compensation factor k = 0.75. Additionally, since the side surface elongates only when the inflation pressure is
By combining Equation (8) with Equation (14) and eliminating higher-order terms, we obtain:
By solving for
Force characteristics of the compression unit
Owing to the soft contact between the compression unit and the human body, the body typically envelops the surface bulging from the top of the compression unit. Therefore, the force perpendicular to the abdominal surface is as follows:
Control System of SACR-RA
Abdominal displacement measurement during the respiration process
After the patient dons SACR-RA, the ties need to be tightened to ensure that the three compression units are snug against the body and are vertical aligned on the outer surface of the abdomen. Next, the distance between the compression units must be adjusted to align them with the obliquus externus abdominis and rectus abdominis, specifically targeting the expiratory muscle group for compression. Therefore, it is necessary to experimentally measure the displacement of various points on the abdomen during respiration, which will guide the control of the compression units’ elongation and release. Since the compression units are symmetrically distributed, the elongation on both sides, which compresses the obliquus externus abdominis, will be equal. Thus, the displacement of the pressure points on the rectus abdominis and obliquus externus abdominis must be determined during the respiration process.
We constructed an experimental machine vision platform as shown in Figure 4a. The platform consists of a frame made from profiles, on which two identical cameras (C920e, Logitech, USA) are placed, with white LED light strips arranged around them. We use MultiDIC (an open-source toolbox for multiview 3D digital image correlation) for image processing. 25 The cameras initially underwent distortion correction and stereo calibration. After calibration, the abdomen was covered with white patterned paper to enhance contrast and create a uniform background. Using a 2-mm diameter stamp dipped in black ink, a spot pattern was created on the patterned paper, as shown in Figure 4b. While the participant was breathing, the cameras captured images of the abdomen, generating point cloud data for various points on the abdomen during the respiratory process. This allowed us to determine the displacement of the abdomen during respiration, as illustrated in Figure 4c.

Abdominal displacement measurement experiment.
The displacement of the pressing points on the lateral and middle parts of the abdominal cavity during respiration were 5.0857 and 5.3966 mm, respectively. Therefore, the elongation ratio of the compression units for the obliquus externus abdominis and rectus abdominis during the driving process was 5.09:5.40.
Design of the control system
Human respiratory model
To effectively compress the abdomen, it is essential to establish a relationship between the respiratory assistance level and lung respiratory conditions. Throughout the compression process, we assume that the cross-section of the abdomen is elliptical, and treat the abdomen as a sealed container in which pressure is inversely proportional to volume. During respiratory assistance, the abdomen contracts actively as the compression unit elongates, leading to an overall reduction in abdominal volume. Since compression on the body is achieved mainly through the bulging of the top surface of the actuator, the abdominal volume is reduced by inflating the top surface, as shown in Figure 5a. For simplicity, we consider the abdomen to be a cylinder. The abdominal volume decreases under the stretching and squeezing of the actuator, and the change in volume can be expressed as:
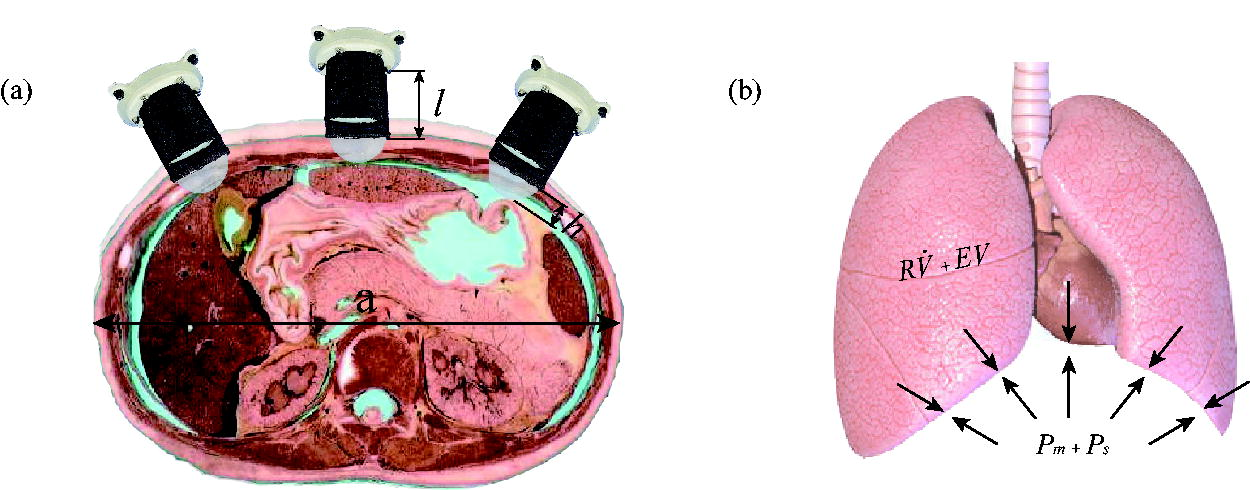
Model of the abdomen and lung.
We obtain
Thus, abdominal compression increases the pressure inside the abdomen, and a portion of this pressure is applied to the lungs.
7
Assuming that there is a constant conversion ratio between the pressure applied by the actuator and the pressure in the lungs, denoted as α, we have
Our goal is to reduce the Pm required for respiration, and we set the control target with a linear combination of
This strategy effectively reduces the required Pm for respiration to
SACR-RA requires real-time monitoring of the user’s respiratory flow during operation. The control system consists of a respiratory flow sensor, a voltage proportional valve, a solenoid valve, a relay, an upper computer (PC), and a lower computer (Arduino Mega2560). Respiratory assistance is a long-term process, and it is crucial to ensure that the patient feels effective compression from the device in each respiratory cycle. Additionally, the device must intelligently adjust the compression mode on the basis of the patient’s recovery status over time. To achieve this, we design different strategies for respiratory pattern control and respiratory intensity control, using the patient’s respiratory flow as feedback, forming a closed-loop control system for respiratory assistance.
Respiratory pattern control
The function of the respiratory pattern control system is to control the elongation and release of the actuator during each step of the breathing process on the basis of the positive and negative values of respiratory flow. This control loop performs the basic function of respiratory pattern control by adjusting the compression unit of SACR-RA during each respiration of the patient. During exhalation, the abdominal muscles contract, pulling the abdominal wall inward and causing the diaphragm to move upward into the chest cavity, facilitating abdominal contraction. During inhalation, the abdominal muscles relax, and the diaphragm moves downward, expanding the chest cavity and causing abdominal expansion. To accommodate the body’s respiratory mechanism, the control system pressurizes the compression units during assisted exhalation, inflating and elongating the bladders while compressing the obliquus externus abdominis and rectus abdominis muscles. This assists in the upward movement of the diaphragm and contraction of the abdominal cavity. During assisted inhalation, the bladder deflates and stops to apply pressure, gradually removing the force to allow for the natural expansion of the abdomen, thus aiding the lungs in inhalation.
We used a respiratory flow meter to measure human respiratory flow. When the participant is wearing the respiratory mask, inhalation and exhalation are represented as opposite amplitudes on the graph, as shown in Figure 6a. We continuously collect respiratory flow signals during the breathing process. The respiratory pattern control system, which is based on the positive and negative values of respiratory flow, controls the on/off status of the electromagnetic valve. When air is released from the air compressor (800W-40L, OUTSTANDING, China), it first passes through the proportional valve (ITV1030, SMC Pneumat, USA), and then enters the compression unit through the electromagnetic valve (10 mm miniature electromagnetic valve, HIGHEND, China). The output pressure of the proportional valve is calculated by the respiratory intensity control system (described in the next section). When powered on, the electromagnetic valve opens, allowing air to enter the compression unit and elongate it. When powered off, the electromagnetic valve closes, releasing air from the compression unit into the atmosphere. The pneumatic system for respiratory pattern control is illustrated in Figure 6b. This method ensures that during exhalation, as the abdomen continuously contracts, the elongation of SACR-RA increases gradually. During inhalation, the system slowly releases pressure, guiding the participant to actively inhale.
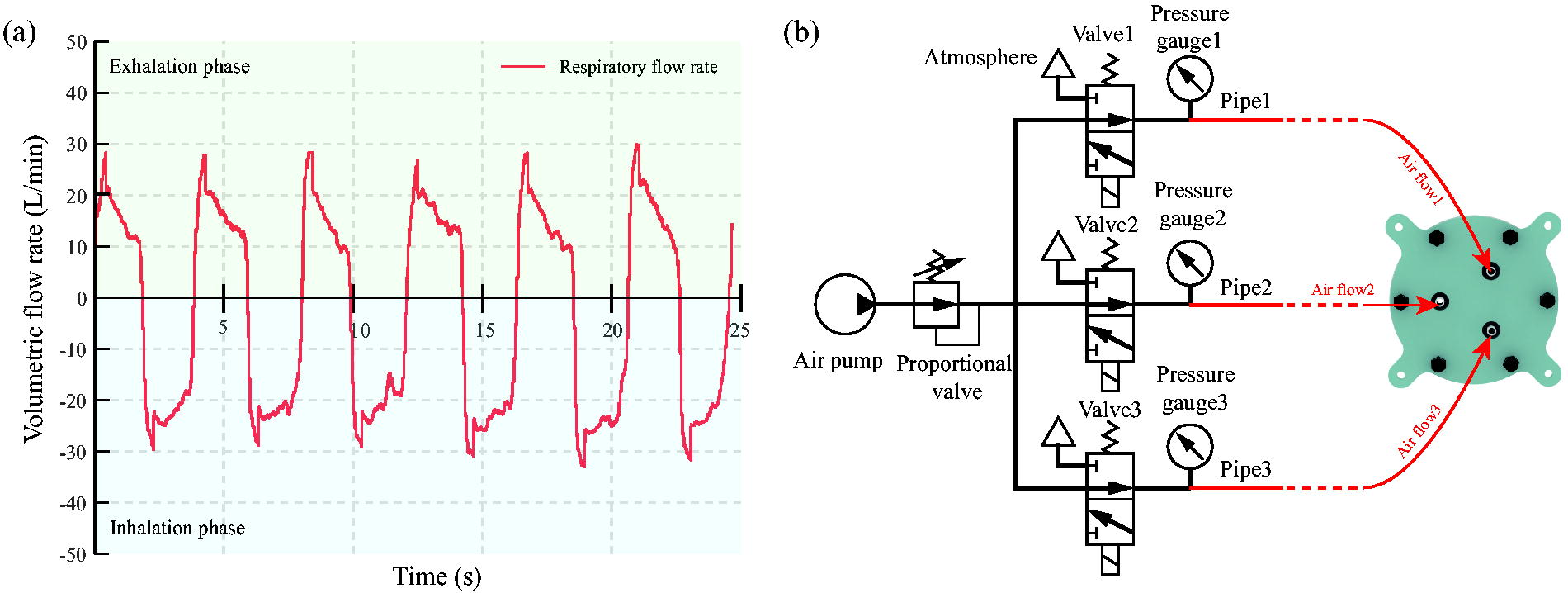
Respiratory pattern control strategy.
To achieve independent control of the different units, we incorporated control switches for each unit in the respiratory pattern control system. Each unit has three air inlets, as shown in Figure 1b, with each inlet controlled by a separate relay. By regulating the intake of air through these inlets, we can vary the inflation speeds of individual compression units and control the inflation sequence across multiple units. During assisted respiration, if the patient’s exhalation time is too long, the system switches from using three inlets to two for intake (a flow rate of 16 L/min) and one for exhaust (a flow rate of 23 L/min). This adjustment slows down the elongation of the compression units, guiding the participant to initiate inhalation.
Respiratory intensity control
The respiratory intensity control system adjusts the output air pressure of the proportional valve on the basis of the participant’s respiratory performance during 1 min, thereby controlling the elongation length of the compression unit. To tailor the compression intensity to the participant’s respiratory condition at various stages, we developed a neural network that correlates the respiratory flow parameters with the air pressure Passt. The participant’s respiratory flow data are first processed using median filtering, and the filtered data are then sent to the respiratory intensity control system for further analysis. The normal respiratory rate for individuals is around 15–20 breaths per minute, and patients with respiratory system diseases typically have slightly higher respiratory frequencies. As such, we selected the first 15 peak values from the minute-by-minute respiratory data as inputs for the algorithm. Compression intensity is categorized into five levels, corresponding to air pressures of 95, 100, 105, 110, and 115 kPa. On the basis, we created a pressure selection neural network for respiratory intensity control, as shown in Figure 7a. We collected a dataset correlating respiratory flow with air pressure. When the respiratory flow is weak, a higher air pressure is chosen, whereas a lower air pressure is selected when respiratory flow is stronger.

Pressure selection neural network.
After the respiratory data are input into the network, forward propagation is performed via Equation (24).
Here, yi represents the output vector of the i-th layer, Ai is the weight matrix for forward propagation in the i-th layer, xi is the input of the i-th layer, and bi is the bias matrix of the i-th layer. The ReLU function is used as the activation function.
In the final layer, the output is converted into probabilities for the five categories, with the highest probability being selected as the baseline pressure Passt. Figure 7b shows the results using a network with five layers, a learning rate of 0.0001, a dropout rate of 0.5, and training over 400 epochs. The network can effectively adjust the pressure based on the participant’s respiratory condition within an acceptable error range (less than 15%), enabling intelligent control of the compression effectiveness.
Before using the SACR-RA, preexperiments are conducted on participants to determine the maximum driving pressure they can tolerate without discomfort. Once the baseline pressure
The control system selects a voltage proportional to the valve output pressure over the long term and controls three compression units separately in the short term. The complete control system is illustrated in Figure 8.

Control system. The system consists of respiratory intensity control and respiratory pattern control systems. The respiratory intensity control system sets the respiratory pressure Passt, whereas the respiratory pattern control system regulates the compression units. Pram is the air pressure delivered to the compression unit on the rectus abdominis muscle and Poea is the air pressure delivered to the two compression units on the obliquus externus abdominis. After entering the proportional valve, high-pressure air is converted into the Pram and Poea outputs that are suitable for the patient’s current respiratory condition.
Experiment
To confirm the effectiveness of the device, we constructed an experimental platform for respiratory assistance, as shown in Figure 9a. Using Python, we built a neural network on a PC that continuously collects participant respiratory flow information within a 1-min cycle. This information is processed by the neural network to determine the proportional valve pressure Passt, which is then converted into air pressure Pram (the air pressure delivered to the compression unit on the rectus abdominis muscle) and Poea (the air pressure delivered to the two compression units on the obliquus externus abdominis). The respiratory pattern control system was used to elongate the compression units during exhalation and contract them during inhalation, providing respiratory assistance. The local Ethics Committee approved the study (ZZUIRB 2024-103). The study conformed to the ethical standards in the Declaration of Helsinki as revised in 2013, and each participant signed a consent form to participate in the study.

Comparison of respiratory performance when assisted and not assisted by SACR-RA.
In this study, five healthy individuals (both males and females) were selected as participants. Data were collected in real-time during each experiment to compare the respiratory performance with and without the SACR-RA. The dynamic respiratory conditions of all participants were analyzed on the basis of the VFR monitored by the flow sensor (CAFS4000B-100 L/min, Xihe Minjiang Instrument, China) and the MAV, which was obtained by integrating the VFR. The participants exerted maximal breathing effort both when wearing and when not wearing the SACR-RA device. The same SACR-RA device was used by all participants throughout the experiment.
Respiratory assistance performance
The primary application of this device is for respiratory assistance. We evaluate its performance through changes in VFR and MAV. During the experiments, the participants lay on a mat and exerted maximal breathing effort for 1 min while being guided by a timer, maintaining a respiratory frequency of 2 s for both inhalation and exhalation. Real-time respiratory flow rate data were continuously collected throughout the experiment. Prior to the data collection, each participant had the opportunity to familiarize themselves with the SACR-RA through free usage.
The experimental results are shown in Figure 9. The changes in VFR and MAV during the experiment clearly revealed that SACR-RA significantly increased the exhalation parameters of the participants. The exhalation VFR increased from 0.47 ± 0.05 to 0.73 ± 0.07 L/s, a 55.3% improvement. Additionally, the device improved inhalation performance, with the inhalation VFR increasing from 0.52 ± 0.04 to 0.80 ± 0.06 L/s, a 53.8% increase. The MAV of respiration also increased from 0.78 ± 0.10 to 1.04 ± 0.05 L/s, a 33.3% increase, indicating significantly improved air exchange with the environment. The respiratory performance data of all participants are presented in Table 1, indicating that the SACR-RA is more effective for participants with weaker respiration, whereas its effectiveness is lower for those with stronger respiration.
Respiratory Performance of Participants
MAV, moved air volume; SACR-RA, soft abdominal compression robot for respiratory assistance; VFR, air volume flow rate.
Muscle EMG performance
To eliminate potential participant-related factors in the respiratory flow experiments, we conducted EMG measurements to verify the impact of SACR-RA on respiratory muscles. Since the SACR-RA primarily affects the external oblique and rectus abdominis muscles, which facilitate diaphragmatic movement, we collected EMG signals from the diaphragm during the respiratory assistance process to validate the effectiveness of the device. Although the diaphragm is an internal muscle, the activity of its rib fibers can be detected on the surface in the seventh and eighth intercostal spaces on the right side of the chest and abdomen. Electrodes were placed in this area, avoiding the nerve supply region due to the muscle’s internal location and its innervation by the phrenic nerve. 27 In the experiment, we used an EMG acquisition system (Trigno, DELSYS INC., USA) and attached EMG electrodes to the surface of the participant’s muscles. Multiple respiratory experiments were conducted to compare the EMG performance when SACR-RA was worn and not worn under similar respiratory intensity conditions, as shown in Figure 10.
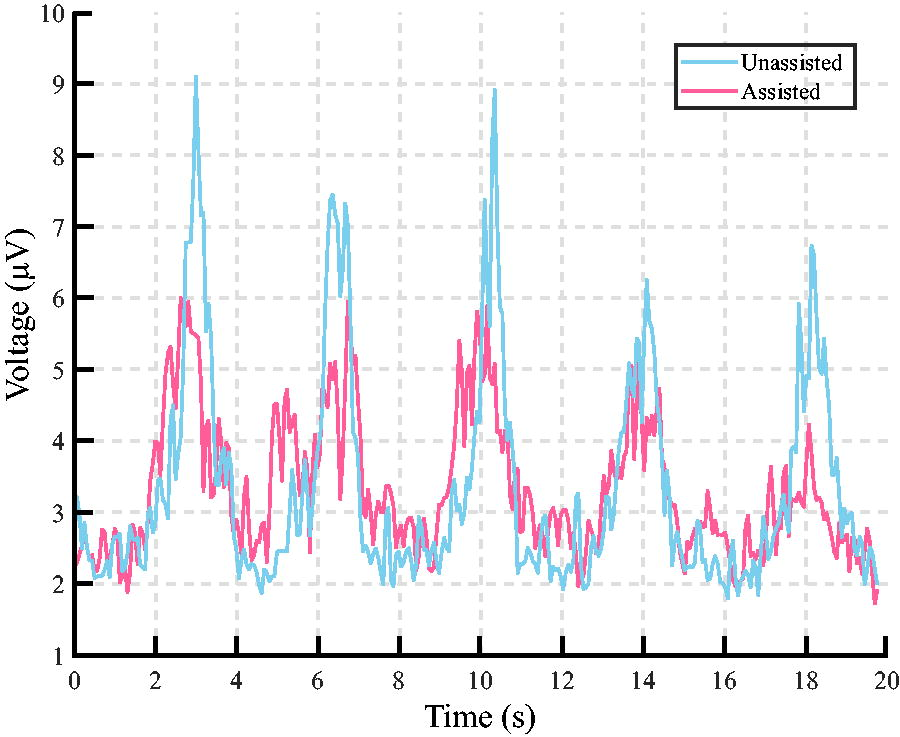
EMG during respiration. We collected the EMG signals of the participants during respiration through two experiments and compared the amplitudes of the signals for the same respiratory intensity. EMG, electromyography.
The experimental data were processed using bandpass filtering between 50 and 250 Hz, and the root mean square of the curve was calculated for plotting. The results show that, under similar respiratory intensity conditions, wearing SACR-RA reduced the peak EMG value of the diaphragm from 7.6785 ± 1.42 to 5.12 ± 0.89 μV, a 33.3% reduction. This experiment confirmed that SACR-RA can effectively reduce respiratory effort and alleviate the burden on respiratory muscles.
Conclusion and Discussion
In this study, we propose and develop a novel SACR-RA to aid individuals in respiratory rehabilitation. The aim of SACR-RA is to provide personalized and adaptive respiratory assistance by dynamically adjusting the pressure applied to the abdominal muscles on the basis of the user’s respiratory characteristics.
We model the top and side surfaces of the compression unit via Yeoh’s hyperelastic model and strain energy theory. The accuracy of the model was experimentally validated, and we established the relationships between the elongation of different compression units during abdominal respiratory experiments. By incorporating a human respiratory model, we developed a connection between the compression unit pressure and the lung condition, confirming the effectiveness of compression and control objectives.
We developed an integrated control system that combines both respiratory pattern control and respiratory intensity control strategies to provide effective and adaptive respiratory assistance. Respiratory pattern control adapts to the user’s respiratory pattern in real-time, whereas respiratory intensity control adjusts the compression intensity on the basis of the patient’s respiratory status at different stages. This dual-control system ensures that SACR-RA can effectively meet the evolving respiratory needs of users, both in the short and long term.
Our experiments demonstrated the effectiveness of SACR-RA for respiratory assistance. The device increased participants’ exhalation VFR by 55.3%, inhalation VFR by 53.8%, and respiratory MAV by 33.3%, significantly improving their air exchange. Additionally, EMG measurements revealed a reduced respiratory muscle burden when participants wore SACR-RA, indicating its ability to effectively reduce the load on respiratory muscles.
The research results suggest that SACR-RA has broad applications in respiratory rehabilitation, offering a multifunctional and adaptable solution for individuals with different respiratory conditions. Its real-time personalized assistance and capacity to adjust to long-term changes make it a valuable tool for promoting respiratory rehabilitation.
Patients with respiratory disorders typically rely on ventilators for treatment, which deliver air directly to the lungs through invasive airway tubes or masks. While these devices provide precise air volume and flow needed, they often impede the natural introduction of airflow into the patient’s mouth and are primarily suited for individuals with severe respiratory impairment, making them less ideal for supporting daily social activities. In contrast, for patients with milder respiratory dysfunction, SACR-RA offers a promising alternative for both hospital-based respiratory training and daily life, as it allows users to retain their ability to breathe autonomously. Future research could focus on expanding participant groups and conducting more extensive clinical trials to validate the effectiveness of SACR-RA across a broader population. Additionally, analyzing the interaction between the device and the human body through indicators such as blood oxygenation, carbon dioxide levels, and diaphragm thickness would provide valuable insights, while exploring its impact on the pelvic floor to ensure safe and effective respiratory assistance.
Footnotes
Author Disclosure Statement
There are no competing financial interests.
Funding Information
This work was supported by the National Key Technologies Research and Development Program of China (No.2022YFB4703202).