
Abstract
Abstract
Background:
Ventilator-associated pneumonia (VAP) is one of the leading causes of morbidity in critically ill surgical patients. Certain pathogens (e.g., methicillin-resistant Staphylococcus aureus, Pseudomonas aeruginosa) have been associated with an excess mortality rate from sepsis in several studies, but not in the surgical setting specifically or when protocol-driven antibiotic therapy is administered.
Purpose:
We sought to determine which factors and, in particular, whether the individual pathogen affected the mortality rate in our surgical intensive care unit (ICU), where a rotational antibiotic system has been employed continuously since 1997. We hypothesized that the type of pathogen and illness severity were the primary influences on the mortality rate of patients with VAP.
Methods:
A total of 198 consecutive patients from a university surgical ICU, with clinical signs of VAP confirmed by quantified isolation of significant numbers of a pathogen (≥104 colony-forming units [cfu]/mL) from bronchoalveolar (BAL) fluid obtained by fiberoptic bronchoscopy, were identified prospectively from January 2001 to November 2004. The data collected were age, sex, Acute Physiology and Chronic Health Evaluation (APACHE) III score, multiple organ dysfunction score, unit day of diagnosis, time (h) to antibiotic administration (TTA), appropriateness of initial therapy (AIT), unit and hospital length of stay, and mortality rate. Pathogens were classified as non-lactose-fermenting gram-negative bacilli (NGNB), lactose-fermenting gram-negative bacilli (LGNB), methicillin-sensitive Staphylococcus aureus, methicillin-resistant S. aureus, yeast, community-acquired pneumonia (e.g., Streptococcus pneumoniae), or other pathogens. Patients with a polymicrobial isolate were placed in the “other” category.
Results:
The overall mortality rate was 32.3% vs. 55% as predicted by APACHE III normative data. The overall AIT was 92%. The mortality rate for NGNB infections was 35.6% vs. 29.4% for LGNB infections (p = NS). By logistic regression, neither TTA, AIT, nor pathogen influenced the mortality rate.
Conclusions:
The type of pathogen does not influence death in surgical ICU patients with VAP diagnosed rigorously and treated by a rotational antibiotic system. The high proportion of AIT as a result of the rotational antibiotic administration system optimizes bacterial killing and negates the impact of bacterial resistance, contributing to better outcomes.
Controversy surrounds the diagnosis and management of VAP, including the optimum method of diagnosis [6–10], duration of therapy [11], effect of specific pathogens [12–14], and whether excess deaths can be attributed to it [4,15] or to other factors such as patient gender [16,17]. In many centers, quantitative sputum culture has supplanted other methods of diagnosis of VAP because of the recent demonstration of superior specificity by quantitative cultures [6,7]. Because of the heterogeneity of VAP cases and widespread institutional bias, optimal diagnosis and therapy have been difficult to define, leading to recently updated guidelines [18].
We sought to determine which factors and, in particular, whether the individual pathogen affected the mortality rate of VAP treated by a rotational antibiotic system. We hypothesized that the type of pathogen and illness severity were the primary influences on the mortality rate in patients with VAP.
Patients and Methods
Consecutive patients from a university surgical ICU with VAP diagnosed by the presence of ≥104 colony-forming units (cfu)/mL in bronchoscopic bronchoalveolar lavage (BAL) fluid were identified prospectively from January 2001 to November 2004. Only patients who had positive cultures of BAL fluid more than 72 h after the initiation of mechanical ventilatory support were included.
Data collected included age, gender, Acute Physiology and Chronic Health Evaluation (APACHE) III score [19], multiple organ dysfunction score (MODS) [20], unit day of diagnosis (DOD), time from diagnosis to initial antibiotic administration (TTA), antibiotics administered, appropriateness of initial therapy (AIT) as noted by in vitro culture data, duration of antimicrobial therapy, and ICU (ULOS) and hospital (HLOS) length of stay. Pathogens were classified as non-lactose-fermenting gram-negative bacilli (NGNB) (e.g., Pseudomonas aeruginosa, Stenotrophomonas maltophila, Acinetobacter spp.), lactose-fermenting gram-negative bacilli (LGNB) (e.g., most members of the Enterobacteriaceae), methicillin-sensitive S. aureus (MSSA), methicillin-resistant S. aureus (MRSA), yeasts, community-acquired pneumonia (CAP) (e.g., Streptococcus pneumoniae), or “other.” Patients with a polymicrobial isolate were placed in the “other” category.
The diagnosis of VAP was made according to a systematic diagnostic approach in accordance with guidelines of the Society of Critical Care Medicine and the Infectious Diseases Society of America [21,22]. Evaluation usually was triggered by fever or leukocytosis, but occasionally by aspiration of purulent sputum during routine pulmonary toilet or a new chest radiographic infiltrate. However, patients with acute respiratory distress syndrome (ARDS) underwent surveillance bronchoscopy because of the high incidence of VAP complicating ARDS and the difficulty in the diagnosis of VAP in patients with ARDS. Sputum was collected by fiberoptic bronchoscopy with BAL from all patients with an artificial airway (endotracheal or tracheostomy tube). The airways were inspected and lavaged with non-bacteriostatic physiologic saline. Directed lavage sometimes was based on the location of purulent secretions in the airway and the appearance of the chest radiograph, but all lung lobes were lavaged with 20 mL of saline. The aliquots were admixed, and a minimum 100 mL of BAL fluid was forwarded to the microbiology laboratory for quantification. A bacterial count of ≥104 cfu/mL of a single pathogen in the fluid was considered consistent with a diagnosis of VAP.
Empiric antibiotics for initial therapy were rotated monthly according to an established schedule among cefepime, ciprofloxacin or levofloxacin (a hospital formulary change was initiated during the study period), imipenem/cilastatin or meropenem (the latter was utilized for patients with renal insufficiency or central nervous system illness or injury), and piperacillin/tazobactam [23]. For suspected pneumonia, vancomycin could be co-administered empirically, but empiric therapy directed against MRSA was not rotated. Synergistic aminoglycoside therapy was administered seldom because of the lack of evidence documenting its utility in immunocompetent adults with pneumonia. Metronidazole was not added to cefepime or levofloxacin to treat pneumonia. Antibiotics were tailored or de-escalated at 48–72 h when microbiologic culture and susceptibility data became available, including discontinuation if infection was not confirmed.
Univariable analysis of coordinate variables was performed by chi-square with the Fisher exact test, and univariable analysis of continuous variables was performed using the Mann-Whitney U test. Another non-parameteric test (Kolmogorov-Smirnov) was used to test differences in data that were not normally distributed according to determination of skewness and kurtosis (i.e., ULOS and HLOS). Changes in continuous variables with respect to time were analyzed by repeated measures analysis of variance (ANOVA) with Bonferroni correction, and correlations were made by the Pearson method. The influences on death of parameters significant by univariable analysis were tested by multiple logistic regression analysis. Statistical significance was defined as α = 0.05.
Results
One hundred ninety-eight patients with VAP were identified during the study period, for a crude incidence of 32.2% for all ventilated patients (Table 1). The mean APACHE III score was 79 points. The overall mortality rate was 32.5% compared with 55% as predicted by normative standards for the APACHE III score [24]. The demographics of patients with VAP stratified by pathogen also are depicted in Table 1. There were no differences in the severity of illness, the development of MODS, or mortality rate according to this stratification. A comparison of APACHE III score and mortality by class of pathogen is sham in Figure 1.
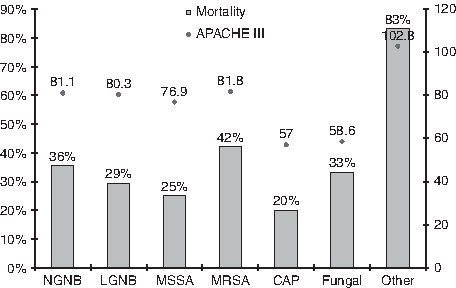
APACHE = Acute Physiology and Chronic Health Evaluation III score; MOD = cumulative multiple organ dysfunction score; AIT = appropriate initial therapy covering recovered pathogens; NGNB = non-lactose-fermenting gram-negative bacilli; LGNB = lactose-fermenting gram-negative bacilli; MSSA = methicillin-sensitive Staphylococcus aureus; MRSA = methicillin-resistant S. aureus; CAP = community-acquired pneumonia.
The bacteria isolated are listed in Table 2. The most common isolate was S. aureus. Notably, the incidence of MRSA was only 30.2%. However, collectively, NGNB were nearly as common as staphylococci. Some characteristics of the six cases in which polymicrobial flora was isolated are shown in Table 3; there were five deaths despite universal AIT. The initial empiric antibiotics administered are depicted in Table 4. Administration of vancomycin was most common, followed by the agents in the rotation schedule. There was no difference in the percentage of appropriateness for individual antibiotics (data not shown but alluded to in Table 1). Overall, the AIT was 92.3% and did not differ by pathogen (Table 1).
MODS = multiple organ dysfunction score; AIII = Acute Physiology and Chronic Health Evaluation III score; AIT = appropriate initial therapy covering recovered pathogens; ULOS = intensive care unit length of stay; DX = diagnosis; N/A = not available.
The characteristics of survivors and non-survivors are summarized in Table 5. By logistic regression analyzing APACHE III, age, AIT, TTA, and pathogen by class, only the APACHE III score independently predicted death (p = 0.046; confidence interval [CI] 1.0, 1.027; odds ratio [OR] 1.013). When performing a logistic regression using AIT, TTA, age, APACHE III score, and pathogen by individual species, no individual parameter, not even APACHE III score, predicted death.
APACHE = Acute Physiology and Chronic Health Evaluation III score; MODS = multiple organ dysfunction score; AIT = appropriate initial therapy covering recovered pathogens; ULOS = intensive care unit length of stay; TTA = time from diagnosis to antibiotic administration; Dx = diagnosis; NGNB = non-lactose-fermenting gram-negative bacillus; MSSA = methicillin-sensitive Staphylococcus aureus; MRSA = methicillin-resistant S. aureus.
Specific attention was given to certain pathogens compared with other pathogens within their own class. Table 6 depicts the demographic data of patients with gram-negative pneumonia subdivided into LGNB and NGNB. Although the NGNB pneumonia patients were older, the mortality rate was equal in the two groups. Table 7 examines patients with gram-positive pneumonia and compares patients with MSSA and MRSA pneumonia. No significant differences were noted in the two groups, although the mortality rate of MRSA pneumonia trended slightly higher.
LGNB = lactose-fermenting gram-negative bacilli; NGNB = non-lactose-fermenting gram-negative bacilli; APACHE = Acute Physiology and Chronic Health Evaluation III score; MODS = cumulative multiple organ dysfunction score; AIT = appropriate initial therapy covering recovered pathogens; ULOS = intensive care unit length of stay; Dx = diagnosis; TTA = time from diagnosis to antibiotic administration.
MSSA = methicillin-sensitive Staphylococcus aureus; MRSA = methicillin-resistant S. aureus; APACHE = Acute Physiology and Chronic Health Evaluation III score; MODS = cumulative multiple organ dysfunction score; AIT = appropriate initial therapy covering recovered pathogens; ULOS = intensive care unit length of stay; Dx = diagnosis; TTA = time from diagnosis to antibiotic administration.
Discussion
Our findings suggest the type of pathogen does not influence the outcome of surgical ICU patients with VAP diagnosed rigorously and treated by a rotational antibiotic system. Inappropriate initial empiric antibiotic therapy has been associated with a higher mortality rate in several clinical studies of sepsis [25–30]. We hypothesize that the high proportion of appropriate initial antibiotic therapy enhanced by antibiotic rotation contributed to the relatively favorable outcomes in our cohort of patients.
The emergence of multi-drug resistant bacteria is raising concern about the effectiveness of therapy for many nosocomial infections and some of community onset [31]. Staphylococcus aureus is the most common pathogen encountered in contemporary ICUs; more than 60% of S. aureus isolates in the United States currently are MRSA [32]. Clinical studies indicate that death is twice as likely with infections caused by MRSA as with MSSA infections [33], although it is debated whether the adverse outcomes are attributable to the virulence of the pathogen or the susceptibility of the host. Pseudomonas aeruginosa is the second most common pathogen in the ICU, and is associated with the highest mortality rates [34]. Pseudomonas aeruginosa now is resistant to many antibiotics, and resistance to carbapenems and, especially, fluoroquinolones is a rapidly growing problem [32,35], although not in our surgical ICU. Other resistance problems that are encountered increasingly in ICUs are multi-drug-resistant Acinetobacter baumannii and Klebsiella spp. and Escherichia coli that produce extended-spectrum beta-lactamases (ESBLs). Paterson et al. documented a higher mortality rate from blood stream infections caused by ESBL-producing Klebsiella spp. [36], lending credence to the possibility that highly resistant bacteria are indeed more virulent.
Kollef et al. examined retrospectively the question of inadequate initial empiric therapy in a cohort of more than 3,000 patients [26], finding that the overall mortality rate increased more than four-fold (52.1% vs. 12.2%) and that infection-related deaths more than doubled (42.0% vs. 17.7%) when initial therapy was inadequate. Therapy was considered adequate in only 44% of cases; the pathogens that were least likely to be covered initially were P. aeruginosa, S. aureus, and Acinetobacter spp. Notably, a prior course of antibiotic therapy during the hospitalization increased the risk of inadequate initial therapy (OR 3.39), implying that antibiotic resistance contributed to inadequacy. Mueller et al. [30] looked retrospectively at 82 critically ill trauma patients who had multiple episodes of VAP. Overall, 39% of episodes (78/200) were associated with inadequate empiric antibiotic therapy in 66% (54/82). The OR for death associated with multiple episodes of inadequate therapy was 4.28 (95% CI 1.44, 12.71).
Although guidelines exist for therapy of VAP [18], there is no clear single choice of antibiotic, nor is there information as to the optimal method by which antibiotics should be administered. Among many questions is whether synergistic therapy with a beta-lactam agent and an aminoglycoside is optimal anti-pseudomonal therapy [37,38]. A recent meta-analysis discourages the addition of an aminoglycoside to beta-lactam monotherapy because there is no improvement in survival or decrement in resistance with this approach, but there is greater nephrotoxicity [47]. Also debated is whether linezolid should supplant vancomycin as first-line therapy for VAP caused by MRSA [48]. What may be most important is the timeliness of administration of well-chosen antibiotics that ultimately prove effective against the offending pathogen. Kumar et al. demonstrated that each 1-h delay in the administration of effective antimicrobial therapy increased the risk of death by 12% [49], and we demonstrated a 4% hourly increase in the risk of death with delayed administration of antibiotics, although our patients were less severely ill than those of Kumar et al.
Ibrahim et al. [27] described protocol-driven therapy instituted to remediate their poor antibiotic selection process. The rate of appropriate therapy increased dramatically, from 44% to 94%; cure rates improved, duration of therapy decreased, and the incidence of recurrent pneumonia decreased also. Other antibiotic management strategies have been described in addition to “protocol-driven therapy,” including antibiotic rotation or “cycling” [39,40], “heterogeneity,” “computerized decision support” [41], “de-escalation” [42], and formulary restriction [41]. There is an emerging consensus not only that initial therapy must be focused, but that therapy should be completed using a short course [11,43] and the narrowest-spectrum agent(s) possible [42]. There still is debate as to which of the above-mentioned strategies, alone or in combination, will best achieve those goals. It may prove to be important that our “best” antimicrobial agents all be used early, rather than being held in reserve; “de-escalation” and formulary restriction may be fundamentally at odds.
We have employed a rotational antibiotic system since July, 1997, coincident with relocation into a new physical plant. Our rotation schema is exempt from our institutional antibiotic control program. Adherence to the protocol is high, as is the appropriateness of initial therapy (e.g., whether the antibiotic(s) chosen for initial therapy is active against the pathogen(s) identified subsequently) [23]. The 92% appropriateness of VAP therapy in the present study compares favorably with the 94% figure we reported previously for the overall program [23], considering that VAP is more likely to be associated with multi-drug-resistant pathogens than is perforated viscus with peritonitis, which constitutes the second most common indication for empiric antibiotic therapy in our practice [44]. Appropriateness was high because antibiotic rotation, along with careful adherence to infection control principles, succeeded in minimizing antimicrobial resistance in our surgical ICU. Appropriateness was enhanced by the fact that only three cases of fungal pneumonia occurred, only one of was managed by appropriate empiric therapy in anticipation of the diagnosis [45].
Rarely have studies in VAP patients examined the effect of the pathogen on the patients' outcomes [51]. A recent study by Vidaur et al. did observe in a cohort of 60 patients with VAP that the presence of MRSA contributed to a longer resolution for hypoxemia, but prediction of death was not a focus of this particular study [52]. We found that the individual pathogen did not affect the outcomes of our patients with VAP. Many potential explanations can be offered. Perhaps we simply have a Type II error and not enough patients were studied. Despite equivalent severity of illness, our study is underpowered (39% power) for the observation that mortality rates of VAP attributable to MSSA and MRSA are not different. For 80% power to detect a true difference in identical populations and mortality rates would require 220 patients (198 patients if the proportion of MRSA-infected patients is 60%).
Our BAL technique also may have contributed notably to our results. We used a standardized technique to collect BAL fluid, but there is no consensus as to the optimal technique, and bias could have been introduced by the size of the aliquot sent to the laboratory. To diagnose pneumonia, we used a cut point of 104 cfu/mL, as is common in the literature, although others have recommended using a cut point of 105 cfu/mL [8]. In choosing the lower value, we could be making an occasional false-positive diagnosis of pneumonia, thereby reducing the power of the study, but we doubt this was the case because few of the bacterial counts we observed in this study were between 104 and 105 cfu/mL. We also tried to enhance our specificity for pneumonia by limiting our diagnostic BALs to patients who were most strongly suspected of harboring pneumonia. We grouped gram-negative bacteria arbitrarily according to metabolic attributes that are detected in the laboratory; a different grouping might have yielded other results.
A variety of other issues may contribute to patient outcome in pneumonia. The appropriateness of initial therapy does enhance positive outcomes. Our unit-specific antibiogram is followed closely by our intensivists to ensure that our empiric therapy maintains clinical strength. Other clinicians have contended that nosocomial pneumonia in surgical patients is merely a marker of host immunosuppression and poor outcome, and that the higher mortality rate cannot be attributed to pneumonia per se [46]. Heyland et al. [15] documented deaths attributable to pneumonia in a cohort of critically ill medical patients, but not critically ill surgical patients. Of course, the non-rigorous diagnosis of pneumonia (no quantitative microbiology) is commonplace in clinical practice and older clinical trials, and routine sputum cultures, which are more often positive than those obtained by bronchoscopic BAL, lead to false-positive diagnoses and over-treatment [50]. Over-treatment, in turn, may increase the risk of later failure should a nosocomial infection caused by a multi-drug-resistant organism supervene. Either scenario could lead ultimately to error in estimating the cause of death attributed to pneumonia.
In summary, treatment of healthcare-associated pneumonia under a rotational antibiotic treatment schema was associated with a correct choice of empiric therapy in 92% of cases. The mortality rate was lower than was predicted by the admission severity of illness and unaffected by the particular pathogen identified by bronchoscopic BAL and quantitative microbiology. Further studies are needed with larger groups of patients to determine conclusively whether the individual pathogen rather than the clinical status of the afflicted patient has a greater role in influencing survival.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
*
Presented at the 25th Annual Meeting of the Surgical Infection Society, Miami, Florida, May 6, 2005.