
Abstract
Abstract
Background:
A major unanswered question in ventilator-associated pneumonia (VAP) management relates to patient response to therapy. We investigated the use of pulmonary cytokines as biomarkers for response to antibiotic therapy for VAP.
Methods:
Prospective, observational pilot study of 12 critically ill trauma patients with VAP using a bronchoscopic bronchoalveolar lavage (BAL) (≥100,000 colony-forming units [cfu]/mL). All patients underwent repeat BAL after three days of adequate antibiotic therapy. Changes in pulmonary effluent interleukin (IL)-8 and tumor necrosis factor (TNF)-α concentrations measured on diagnostic and repeat BAL were evaluated on the basis of the presence of a microbiologic response (<10,000 cfu/mL on repeat BAL).
Results:
Six post-therapy BAL samples showed a microbiologic response. In responders, IL-8 and TNF-α concentrations decreased significantly (1,303 ± 1,150 ng/mL in diagnostic BAL sample vs. 309 ± 448 ng/mL after response; p = 0.08 and 9.9 ± 18.4 ng/mL in diagnostic vs. 0.1 ± 0.1 ng/mL in post-treatment sample; p = 0.06, respectively). In non-responders, IL-8 (449 ± 426 ng/mL vs. 326 ± 319 ng/mL; p = 0.59) and TNF-α (1.2 ± 1.9 ng/mL vs. 0.3 ± 0.3 ng/mL; p = 0.31) did not change significantly. Clinical response measures did not change or increased in responders, whereas these parameters did not change or decreased paradoxically in non-responders.
Conclusion:
This pilot study indicates pulmonary concentrations of IL-8 and TNF-α decrease in microbiologic responders with VAP. Conversely, clinical response parameters were discordant with the microbiologic response. The utility of pulmonary cytokine behavior in evaluating the effectiveness of antibiotic therapy for VAP should be studied further.
Bacteria infecting the lower airways initiate an acute inflammatory host response. Regulation of this response depends on complex interactions between immune cells and pro-inflammatory and anti-inflammatory cytokines such as interleukin (IL)-8 and tumor necrosis factor alpha (TNF-α) [2]. During pneumonia and critical illness, serum cytokine concentrations do not correlate with pulmonary cytokine concentrations [3–6]. Therefore, the greater specificity of pulmonary cytokine concentrations [7] may offer an opportunity to grade the site-specific response to antibiotic therapy and overcome the nonspecific nature of traditional global signs and symptoms associated with VAP. This pilot study evaluated the relation between pulmonary IL-8 and TNF-α concentrations and the microbiologic response during adequate antimicrobial therapy in critically ill patients with VAP. The relation between cytokine concentration and the gram-stain response of the causative pathogen(s) also was evaluated.
Patients and Methods
Patients
This observational pilot study was conducted in the Level I trauma ICU at the Presley Regional Trauma Center in Memphis, Tennessee. The study was approved by The University of Tennessee Institutional Review Board. Written informed consent was obtained for all patients. Patients were enrolled if they (1) had VAP defined as [a] mechanical ventilation ≥48 h; [b] new or changing infiltrate on chest radiograph; [c] at least two clinical signs of pneumonia (temperature 38°C or higher leukocyte count 10,000/mcL or higher or >10% bands; or macroscopically purulent sputum); and [d] quantitative bronchoalveolar lavage (BAL) culture containing at least one bacterium with growth ≥100,000 colony forming units (cfu)/mL] [8–11]; (2) were ≥18 years of age; and (3) had a repeat BAL performed after three days of adequate antibiotic therapy. Patients were excluded if they had (1) active malignant disease; (2) a leukocyte count <4,000/mcL; (3) chronic use of immunosuppressive medications; (4) acute respiratory distress syndrome [12]; (5) concurrent meningitis; (6) concurrent intra-abdominal infection; or (7) transfer from another hospital ≥48 h after injury.
Procedures
All patients underwent diagnostic and repeat BAL according to the inclusion criteria. All BAL procedures were performed in a uniform manner by the treating surgeon as part of standard medical care. After blind endotracheal suctioning through the ventilator circuit, the bronchoscope was advanced into the lung segment wherein radiographic changes were seen or into the left lower lobe of patients who had diffuse bilateral infiltrates. With the bronchoscope wedged into the appropriate lung segment, 100 mL of sterile, nonbacteriostatic saline was instilled in five 20-mL aliquots. The effluent was pooled and sent to the hospital microbiology laboratory for quantitative culture [13]. In compliance with the VAP clinical guideline in the trauma ICU, patients in the unit for seven days or less (early VAP) received ampicillin sulbactam 3 g intravenously every 6 h (or equivalent alternative in penicillin-allergic patients), whereas patients in the ICU greater than seven days (late VAP) received cefepime 2 g intravenously every 8 h and vancomycin 20 mg/kg intravenously every 12 h (dose adjusted to maintain steady-state peak serum vancomycin concentrations of 35 to 45 mg/L and trough concentrations of 10 to 20 mg/L). At the treating team's discretion, empiric antibiotic therapy was streamlined according to the susceptibility results for causative pathogens. Repeat BAL was not conducted until the patient had received at least three days of adequate antibiotic therapy.
Approximately 5–10 mL of the diagnostic or repeat BAL sample was centrifuged, and the supernatant liquid was stored at −70°C until analysis. The IL-8 and TNF-α concentrations were determined using enzyme-linked immunosorbent assay (ELISA) kits (EH2IL8; Pierce Endogen, Rockford, IL and HSTA00C; R&D Systems, Minneapolis, MN, respectively) [14]. In conjunction with plasma urea nitrogen concentration (BUN) from daily laboratory reports, the BAL urea concentration was determined using a spectrophotometric kit (Stanbio Laboratories, Boerne, TX) and used to correct for the dilutional effects of the BAL effluent. Urea and cytokine assays were modified for BAL fluid analysis using previously validated methods [15]. Corrected cytokine concentrations were calculated using the following equation:
Patients were classified on the basis of repeat BAL culture results. Microbiologic responders had repeat BAL samples wherein all bacteria demonstrated growth <10,000 cfu/mL, whereas microbiologic non-responders had persistent growth of ≥10,000 cfu/mL of the original pathogen [16]. A new VAP episode was diagnosed if a different pathogen demonstrated ≥100,000 cfu/mL on repeat BAL [8–11].
Diagnostic and repeat BAL cytokine concentrations as well as clinical parameters were compared using a paired Student t-test or Wilcoxon signed rank test, as appropriate. Continuous data are reported as mean ± standard deviation (SD). All statistical analyses were performed using SigmaStat v. 2.03 (Systat Software Inc., Richmond, CA). As this small pilot study was intended as hypothesis generating, p < 0.1 was considered statistically significant.
Results
A total of 12 patients underwent 24 BALs (one diagnostic, one repeat). In all but two patients, the diagnostic BALs were for the patients' first VAP episode. Patient characteristics and the pathogens causing the initial VAP episodes are provided in Table 1. The mean time to repeat BAL was 3.25 ± 0.97 days (SD). Of the 12 paired BALs, six (50%) demonstrated a microbiologic response, two (17%) no response, and four (33%) a new VAP. As indicated in Table 1, one microbiologic responder was infected only with a gram-positive pathogen, two were infected only with gram-negative pathogens, and three were infected with both types. Three of the patients with a new VAP initially were infected only with gram-positive pathogens, whereas one was infected initially only with a gram-negative organism. Both microbiologic non-responders were infected only with gram-negative pathogens. Although total bacterial colony counts (sum of all counts for all identified pathogens in the BAL samples) and IL-8 and TNF-α concentrations were higher in microbiologic responders in the diagnostic BAL, the cytokine concentrations correlated poorly with total bacterial colony count (IL-8: R 2 = 0.12; TNF-α: R 2 = 0.19). All patients were treated successfully and survived their hospital stays.
Ab = Acinetobacter baumannii; APACHE = Acute Physiology and Chronic Health Evaluation; Ax = Achromobacter [Alcaligenes] xylosoxidans; BAL = bronchoalveolar lavage; Ec = Escherichia coli; GBS = group B Streptococcus; Hi = Haemophilus influenzae; ICU = intensive care unit; ISS = Injury Severity Score; LOS = length of stay; MRSA = methicillin-resistant Staphylococcus aureus; MRSE = methicillin-resistant Staphylococcus epidermidis; MSSA = methicillin-susceptible Staphylococcus aureus; MV = mechanical ventilation; Ns = Neisseria spp.; Pa = Pseudomonas aeruginosa; Pm = Pasteurella multocida; Sm = Serratia marcescens; VAP = ventilator-associated pneumonia; VS = viridans streptococci.
The six microbiologic responders demonstrated a significant decrease in IL-8 and TNF-α concentrations on repeat BAL (IL-8: mean 1,303 ± 1,150 ng/mL in the diagnostic sample vs. 309 ± 448 ng/mL after treatment; p = 0.08 and TNF-α: mean 9.9 ± 18.4 ng/mL vs. 0.1 ± 0.1 ng/mL; p = 0.06)(Fig. 1). Microbiologic non-responders or those with new VAP demonstrated non-significant changes in IL-8 and TNF-α concentrations (IL-8: mean 449 ± 426 ng/mL vs. 326 ± 319 ng/mL; p = 0.59 and TNF-α: mean 1.2 ± 1.9 ng/mL vs. 0.3 ± 0.3 ng/mL; p = 0.31). Additionally, Figure 1 illustrates the changes in total bacterial counts in microbiologic responders and non-responders or patients with a new VAP.
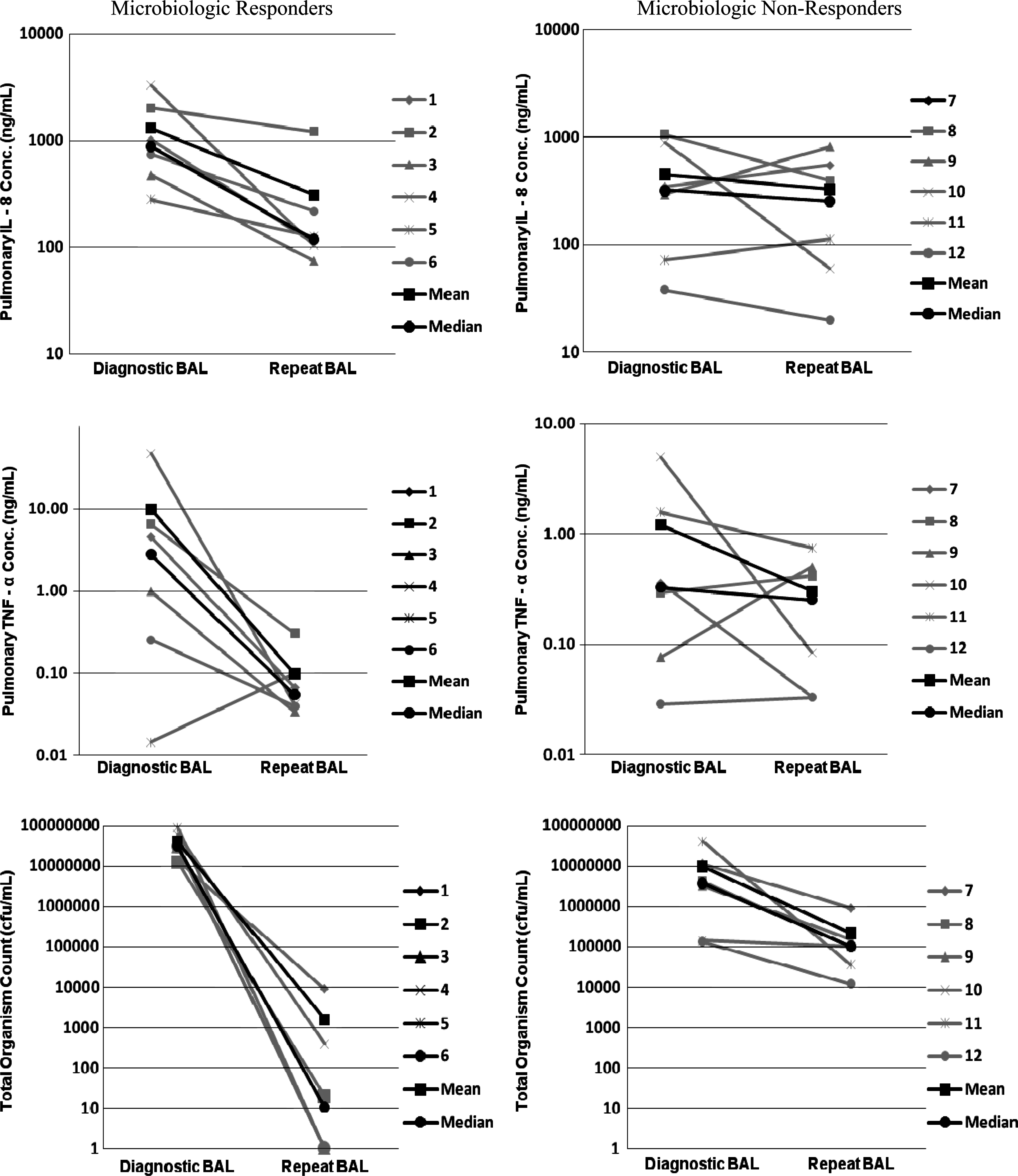
Changes in pulmonary interleukin-8, tumor necrosis factor-α, and bacterial count at repeat brochoalveolar lavage (BAL) categorized by microbiologic response. Patients with a new ventilator-associated pneumonia (VAP) are included in the non-responder group. The mean and median for all patients in each category also are presented. Cfu = colony forming units.
Figure 2 shows the clinical response measures at the time of diagnostic and repeat BAL. For responders, the mean maximum temperature (Tmax) did not change significantly (103.3 ± 1°F vs. 102.3 ± 1.1°F; p = 0.13). The white blood cell (WBC) count showed a significant increase (11 ± 6/mcL vs. 16 ± 7/mcL; p = 0.05), and PaO2:FIO2 did not change significantly (249 ± 82 mm Hg vs. 254 ± 72 mm Hg; p = 0.86). In the six non-responders/new VAP, the Tmax decreased significantly (103.2 ± 1.4°F vs. 101.2 ± 1.6°F; p = 0.08), whereas the WBC count demonstrated a non-significant increase (11 ± 5/mcL vs. 13 ± 4/mcL; p = 0.52), and PaO2:FIO2 showed a non-significant decrease (258 ± 70 mm Hg vs. 245 ± 40 mm Hg; p = 0.73).

Changes in clinical parameters at repeat brochoalveolar lavage (BAL) for individual patients categorized by microbiologic response. Patients with a new ventilator-associated pneumonia (VAP) are included in the non-responders group. The mean and median for all patients in each category also are presented.
Data were stratified by the gram-stain results of the organism(s) causing VAP and were classified as only gram-positive, only gram negative, or both gram negative and gram-positive (Table 2). The small number of patient samples precluded statistical analysis, but changes in bacterial counts and IL-8 and TNF-α concentrations appear similar to the overall analysis.
Mean ± standard deviation unless stated otherwise.
Values for individual patient.
BAL = bronchoalveolar lavage; IL = interleukin; N/A = not available; TNF = tumor necrosis factor; VAP = ventilator-associated pneumonia.
Discussion
The results of this pilot study describe differences in pulmonary concentrations of IL-8 and TNF-α measured at diagnosis of VAP and during adequate antibiotic therapy. In patients demonstrating a microbiologic response to therapy, there was a 76.3% decline in IL-8 and a 98.9% decrease in TNF-α despite persistent clinical signs of infection. Although pulmonary cytokine concentration is increased at the time of VAP diagnosis [4, 17–19], this is the first report of the potential of these markers to indicate patient response to antibiotic therapy. These results are strengthened by the use of quantitative BAL culture results that identify the presence of VAP more accurately [1, 9–11].
Three studies have examined pulmonary cytokines in VAP [4, 17, 18]. Shütte et al. reported that pulmonary IL-6, IL-8, and TNF-α measured at 0–2, 3–10, and >10 days after intubation did not decrease until >10 days post-intubation [18]. A different study of 12 patients with VAP measured IL-6, IL-1β, and TNF-α at VAP diagnosis (day 1), day 3, and day 7. The concentration of IL-6 in the BAL sample had declined significantly on days 3 and 7 [17] Conversely, Millo et al. reported minimal change over time in pulmonary IL-6, IL-1α, IL-1β, and TNF-α in nine patients with VAP [4]. Although two of these three studies demonstrated a general decrease in pulmonary cytokines after VAP diagnosis, none evaluated the association between cytokine changes and the microbiologic response to antibiotic therapy.
The second important finding of this study was that clinical signs did not correspond to the microbiologic response. Indeed, the leukocyte count increased significantly in responders. Other investigators likewise have shown that infective measures in VAP are highly variable and slow to return to normal after therapy. Furthermore, individual parameters such as leukocyte count can remain elevated for as long as 28 days after diagnosis [20, 21]. Recent attempts to validate the utility of clinical signs (clinical pulmonary infection score [CPIS]) for VAP diagnosis in trauma patients were disappointing, and such measures are unlikely to be useful in determining the response to therapy [22]. Interestingly, microbiologic non-responders had lower bacterial inocula, but also lower IL-8 and TNF-α concentration at diagnosis. Perhaps the lower cytokine concentrations and the subsequent lesser change in these markers and bacterial inocula during antibiotic therapy reflect a state of relative immunoparalysis otherwise unaccounted for by global clinical response measures.
The apparent discordance between clinical and microbiologic responses supports the need for more objective determinations of antibiotic therapy duration. Even though shorter durations of therapy for VAP (7–8 days) are becoming more accepted for many patients, longer durations still are recommended in certain scenarios including infection with non-fermenting gram-negative bacilli, persistent signs and symptoms, or inadequate empiric antibiotics [16, 21]. Antibiotic durations often are arbitrary in these situations. A more objective determination of response would be a major improvement in VAP management that would result in shorter duration of therapy for many responding patients and perhaps earlier decisions to modify therapy in non-responders. Interestingly, the two non-responding patients were infected with non-fermenting gram-negative bacilli. Although they eventually cleared their VAP, it is notable that patients such as these may require longer durations of antibiotic therapy [16, 21]. Indeed, recent evidence demonstrated delayed eradication of Pseudomonas aeruginosa strains that produce at least one type III secretion system protein [23]. As such, treatment of patients infected with these strains may require non-traditional monitoring for response.
The primary limitation of this study is its small size. However, the promising results from this pilot study have prompted a larger study, currently underway. Additionally, the level of significance (p < 0.1) provided sufficient pilot-level confidence (i.e., 90%) in detecting differences in intra-patient pulmonary cytokine concentrations. Other limitations include the arbitrary timing of repeat BAL collection and the stringent cutoff threshold for response, requiring all pathogens to be <10,000 cfu/mL whatever the initial count. However, we believe these criteria are reasonable in view of previous reports showing that most (88%) lower respiratory tract infections are eradicated or, at least contained, by day three of antibiotics [24]. Finally, this study did not evaluate cytokines in comparison with other biomarkers that have demonstrated promising results for guiding the duration of antibiotic therapy. Serial monitoring of serum procalcitonin reduces antibiotic duration in patients with community-acquired pneumonia [25] or sepsis [26] and infections in surgical ICU patients [27]. A decreasing serum procalcitonin concentration also correlates with survival after a diagnosis of VAP [28], whereas persistence of an elevated serum concentration (>0.5 ng/mL) on day seven was an independent marker of an unfavorable outcome [29]. Unfortunately, pulmonary procalcitonin concentration is not as helpful as the serum concentration in VAP [30], and this study was focused on pulmonary biomarkers in relation to response to antibiotic therapy.
Conclusion
This pilot study indicates pulmonary concentrations of IL-8 and TNF-α decrease in microbiologic responders. Conversely, clinical response parameters are discordant with the microbiologic response. The utility of pulmonary cytokine behavior in evaluating the effectiveness of antibiotic therapy for VAP should be studied further.
Author Disclosure Statement
No conflicting financial interests exist.