
Abstract
Abstract
Background:
Inadequate antibiotic therapy and failure to administer antibiotics in a timely fashion have been associated with substantial mortality rates in patients in the intensive care unit (ICU). We analyzed the infection pattern in solid organ transplant recipients as well as the impact of antibiotic resistance and inadequate antibiotic treatment on mortality rates and morbidity outcomes.
Methods:
Charts of adult solid organ transplant recipients in 2006 from a single institution were reviewed. Data on patients with bacterial and fungal infections acquired within one year after transplantation were compared with the primary outcome of death within 28 days. Statistical analysis included nonparametric tests (Wilcoxon rank sum, Fisher exact, and chi-square) and multivariable logistic regression with p < 0.05 considered significant.
Results:
Of the 366 patients, 114 (31%) had a total of 208 bacterial or fungal infections, and 44 of them (39%) were admitted to the ICU. Our primary endpoint, the 28-day mortality rate, was 8% overall, whereas the six-month mortality rate was 11%. Patients treated inadequately with antibiotics had a significantly higher mortality rate. The leading causes of infection were multiple organisms, coagulase-negative Staphylococcus, and E. coli, of which 76% were resistant to antibiotics. Antibiotic-resistant infections were associated with longer hospital stays (p = 0.04), intravenous antibiotic use prior to infection (p = 0.04), nucleotide synthesis inhibitor use (p = 0.02), ICU admission (p < 0.01), and respiratory failure (p = 0.03). Most infections were treated inadequately initially (69%) but treated adequately at 24 h (56%). Inadequate antibiotic treatment was significantly associated with younger age (p = 0.04), prior intravenous antibiotic use (p = 0.04), longer stay prior to infection (p = 0.05), and cardiovascular shock (p = 0.014). Inadequate antibiotic therapy at 24 h was associated with a higher mortality rate (14% vs. 2%; p = 0.03) and a trend toward longer ICU and in-hospital stays.
Conclusions:
Most bacterial and fungal infections were resistant to antibiotics and were treated inadequately initially. Prior intravenous antibiotic use and longer stay prior to infection were associated with antibiotic resistance and inadequate antibiotic therapy. Failure to provide adequate antibiotic treatment within 24 h had a significant impact on the 28-day mortality rate and was associated with other detrimental clinical outcomes.
Inadequate antibiotic treatment caused by resistance or failure to administer antibiotics in a timely fashion has been associated with increased mortality and morbidity rates in critically ill patients [5], as well as in patients with blood stream infections [6], sepsis and septic shock [7], and ventilator-associated pneumonia [8]. Delayed administration of adequate antibiotics is associated with an incremental increase in the risk of death as early as the second hour after diagnosis in patients with septic shock [9].
There is a paucity of data regarding the morbidity and mortality rates associated with inadequate antibiotic therapy in solid organ transplant recipients. We hypothesized that antibiotic-resistant infections and inadequate antibiotic treatment increase the mortality and morbidity rates in such patients. To determine whether this is correct, we analyzed infection patterns in solid organ transplant recipients admitted to the University of Minnesota Medical Center, Fairview to assess the relation between antibiotic resistance, inadequate antibiotic treatment, and patient outcomes (28-day and six-month mortality rates, hospital and ICU length of stay [LOS], and acquired organ dysfunction).
Patients and Methods
Study design and patient population
The study protocol was approved by the University of Minnesota Institutional Review Board. Charts of adults receiving solid organ transplants in 2006 were reviewed. Patients confirmed to have fungal or microbial infections within one year after transplantation were included in the analysis.
Resistance of cultured organisms to antibiotics and adequacy of antibiotic treatment at the time of diagnosis (T = 0) and at 24 h (T = 24) were correlated with patient outcome. The primary outcome measure was death within 28 days. Secondary outcomes were the six-month mortality rate, hospital and ICU LOS, and acquired organ dysfunction.
Definitions
The U.S. Centers for Disease Control and Prevention definitions of nosocomial infection were used [10]. Resistant bacteria included MRSA, vancomycin-resistant S. aureus (VRSA); coagulase-negative Staphylococcus (CNS) resistant to oxacillin; VRE; Pseudomonas aeruginosa and other non-fermentative gram-negative bacilli resistant to at least ceftazidime, aminoglycosides, extended-spectrum penicillins, carbapenems, or quinolones; Enterobacteriaceae resistant to at least third-generation cephalosporins, quinolones, or carbapenems; and anaerobic bacteria resistant to metronidazole. Resistant fungi were those not susceptible to azoles.
Inadequate treatment was defined as at least one cultured isolate resistant to all prescribed antibiotics and adequate treatment as administration of at least one antibiotic effective against all cultured isolates. Acquired organ dysfunction was evaluated according to multiple organ dysfunction score definitions [11] and the International Sepsis Definitions Conference [12].
Data collection and statistical analysis
Patients were identified through the Transplant Information Services database, and data were collected from electronic medical records. Demographic data collected included age, weight, and sex. Other patient variables collected were transplant history, immunosuppressive regimen, co-morbidities, rejection episodes, time elapsed from transplant to infection, microbiology results, source of infection, antibiotic use, and LOS prior to infection. The outcome variables collected were adequacy of antibiotic treatment, in-hospital and ICU LOS, 28-day and six-month mortality rate, days on mechanical ventilation, vasopressor use, renal replacement therapy de novo, and acquired organ dysfunction.
Statistical analysis was conducted with non-parametric tests considering the data were skewed: Wilcoxon rank sum test for median comparison and the Fisher exact and chi-square tests for percentages. Stepwise multivariable logistic regression analysis was used to assess the factors influencing survival, antibiotic resistance, and inadequate antibiotic treatment. All tests were two-tailed, with p < 0.05 being considered significant. The SPSS software v. 14 and SAS v. 9.1 (SAS Institute, Cary, NC) were used for the analysis.
Results
Of 370 adult patients receiving solid organ transplants in 2006, four were excluded because of incomplete medical records, leaving 366 for our evaluation. In the year after transplantation, 114 (31%) patients were confirmed to have 208 episodes of bacterial or fungal infections, and 252 isolates were cultured. Admission to the ICU was required by 44 (39%) of the infected patients. Our primary endpoint, the 28-day mortality rate, was 8% overall, whereas the six-month mortality rate was 11%. Patients treated inadequately with antibiotics had a significantly higher mortality rate (Fig. 1). Of the 13 episodes of infection in nine patients that were followed by death within 28 days, 46% were pneumonia and were caused by multiple organisms, and 62% were encountered in liver and lung transplant recipients.
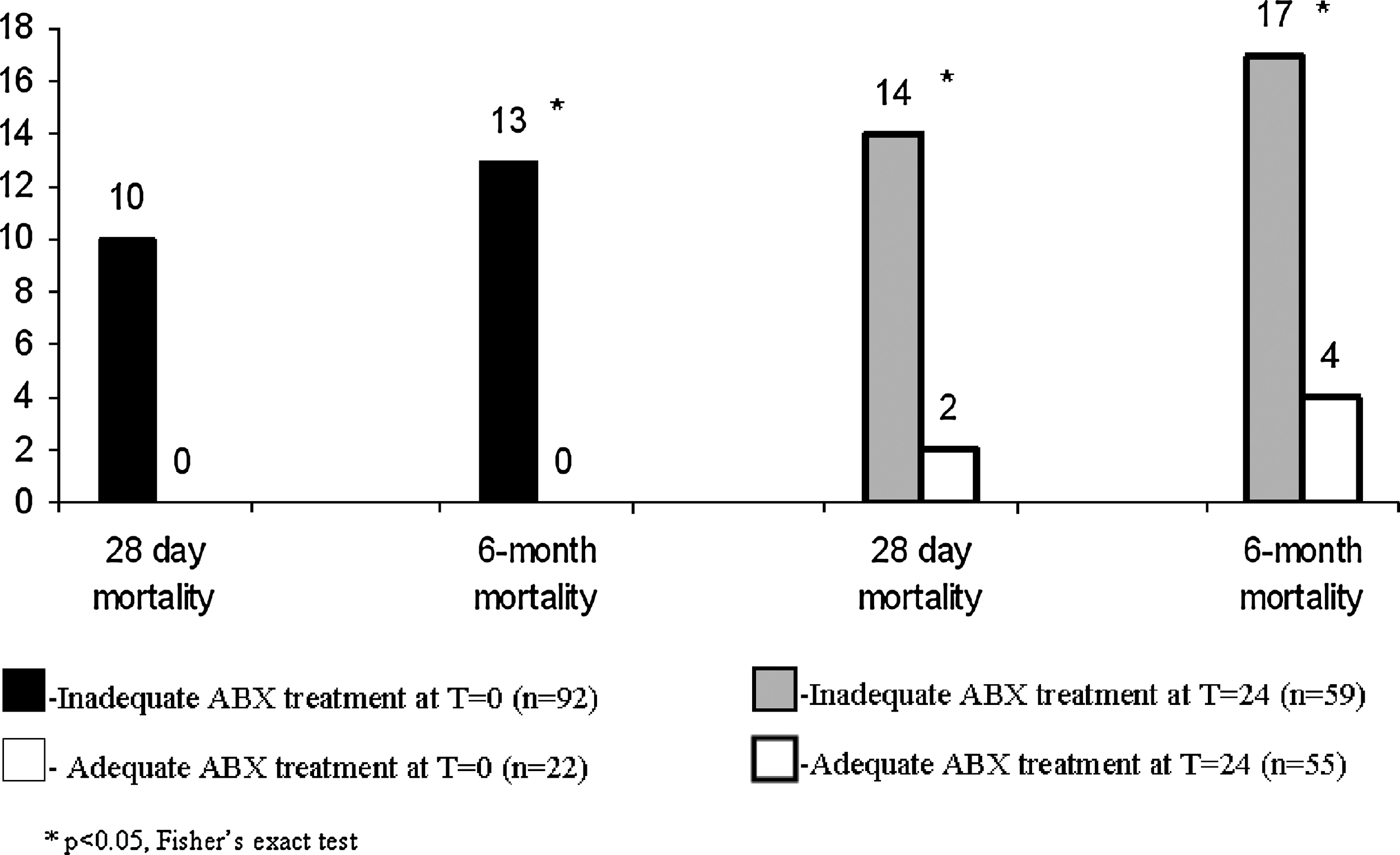
Mortality rate according to adequacy of antibiotic treatment.
When all 366 patients were considered, 64% of the pancreas–kidney transplant recipients acquired infection within one year after transplantation compared with 41% of the pancreas, 40% of the lung, 33% of the liver, 29% of the heart, and 24% of the kidney transplant recipients. The characteristics of the 114 patients with infections are summarized in Table 1. Of the 114 patients, 25 were admitted for an acute rejection episode, 13 for immunosuppression toxicity, eight for allograft loss, and three for a chronic rejection episode. Most of the eight graftectomies were associated with intra-abdominal or multiple site infections, with only one case being associated with a decrease in immunosuppression. All patients who underwent graftectomy survived at 28 days.
Of the 208 infection episodes, 68 (32%) urinary tract, 45 (22%) pneumonia, 39 (19%) intra-abdominal, 25 (12%) surgical site, 16 (8%) blood stream, 13 (6%) multiple sites, and two (1%) skin and soft tissue infections. Cardiovascular shock was the most common consequence of infection, occurring in 63 episodes (30%). Acute renal failure occurred concomitantly with 60 infection episodes (29%) followed by acute respiratory failure with 44 (21%), coagulopathy with 37 (18%), Glasgow Coma Scale score <13 with 16 (8%), and hepatic failure with 14 (7%). The median time from transplantation to infection was 36 days (range 0–362 days). Prior to infection, the median LOS was two days (range 1–134 days), the hospital LOS was 13 days (range 1–150 days), and the ICU LOS was eight days (range 1–58 days). Patients required mechanical ventilation for a median of five days (range 1–53 days) and vasopressors for 2.5 days (range 1–6 days).
The culture results for the 208 infection episodes and the susceptibility of the organisms to antibiotics are depicted in Figure 2. The leading etiologies of infection were multiple organisms (19%), coagulase-negative Staphylococcus (16%), and E. coli (13%). Isolates from these three sources were resistant to antibiotics in 76% of cases (77/101). Vancomycin-resistant Enterococcus (5%) and MRSA (1%) caused infection uncommonly. Clostridium difficile and Candida species were the etiologic factors in a similar percentage (8%) and were rarely assessed for resistance to antibiotics. Only two isolates (one each of Burkholderia cepacia and Acinetobacter baumannii) were resistant to all antibiotics tested. Rarely cultured organisms were Citrobacter and Enterobacter spp., Streptomonas maltophilia, Burkholderia cepacia, and Aspergillus fumigatus (5% combined). There were no VRSA isolates.
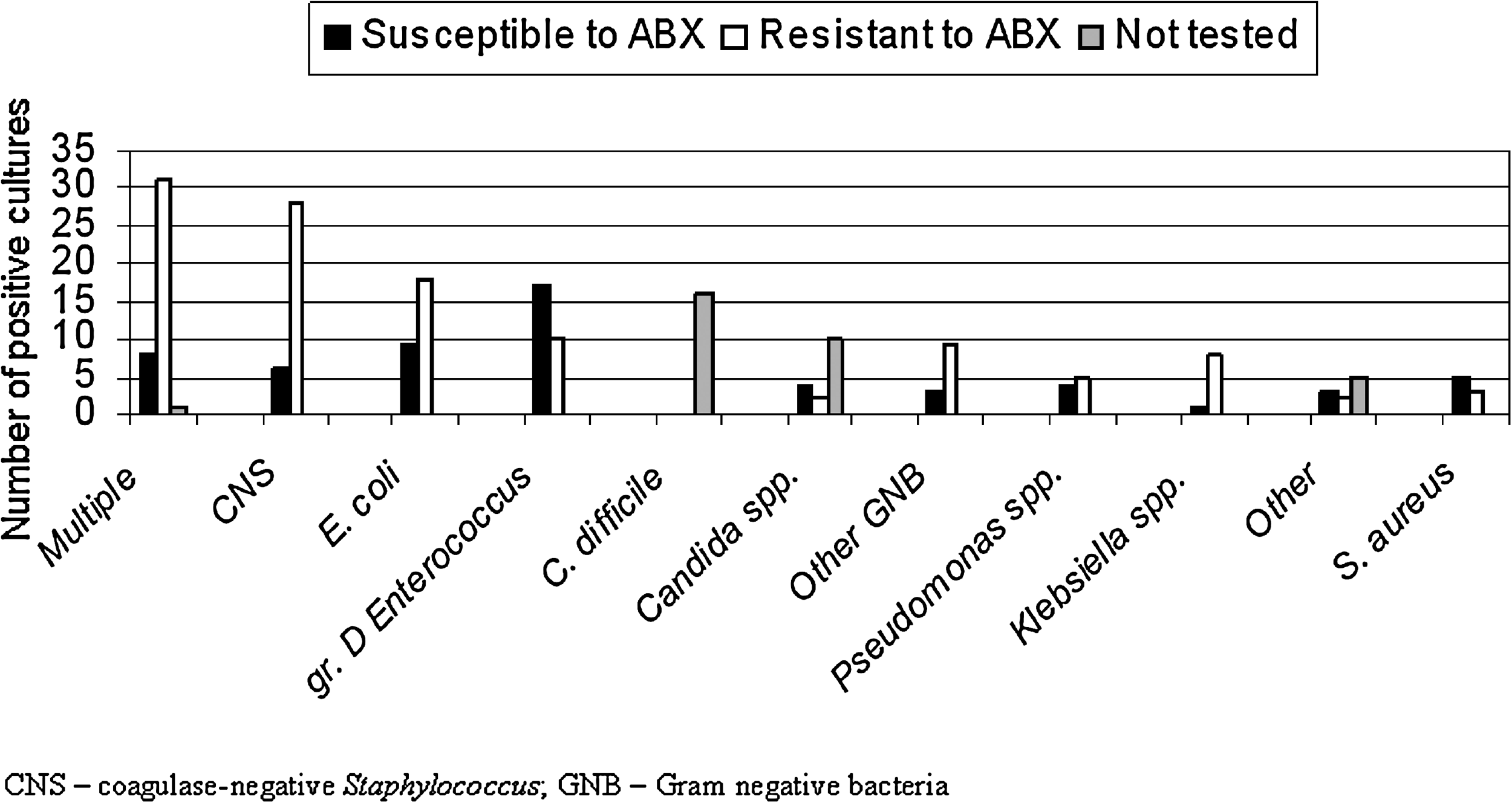
Number of positive culture results, organisms isolated, and antibiotic resistance for 28 episodes of infection. CNS = coagulase-negative Staphylococcus; GNB = gram-negative bacillus; gr. D. Enterococcus = enterococci.
Factors significantly associated with antibiotic resistance by univariable analysis are summarized in Figure 3. Age, weight, sex, transplant history, co-morbidities, rejection episodes, days from transplantation to infection, microbiology results, source of infection, and adequacy of antibiotic therapy were similar in the antibiotic-resistant and -susceptible infections. Greater LOS, intravenous antibiotics, and nucleotide synthesis inhibitor use prior to infection were associated with a significantly higher percentage of antibiotic-resistant infections. Respiratory failure and ICU admission both were more frequent in antibiotic-resistant infections. We found little difference in other outcomes in resistant vs. susceptible infections, including hospital LOS, 28-day and six-month mortality rates, renal replacement therapy de novo, and acquired organ dysfunction other than respiratory failure. Although the differences were not statistically significant, outcomes that may have clinical relevance because of their being more common in resistant than in susceptible infections were longer ICU LOS (median 5 vs. 4 days; p = 0.93), longer mechanical ventilation duration (median 4.5 vs. 2 days; p = 0.56), and longer vasopressor treatment (median 3 vs. 2 days; p = 0.16).
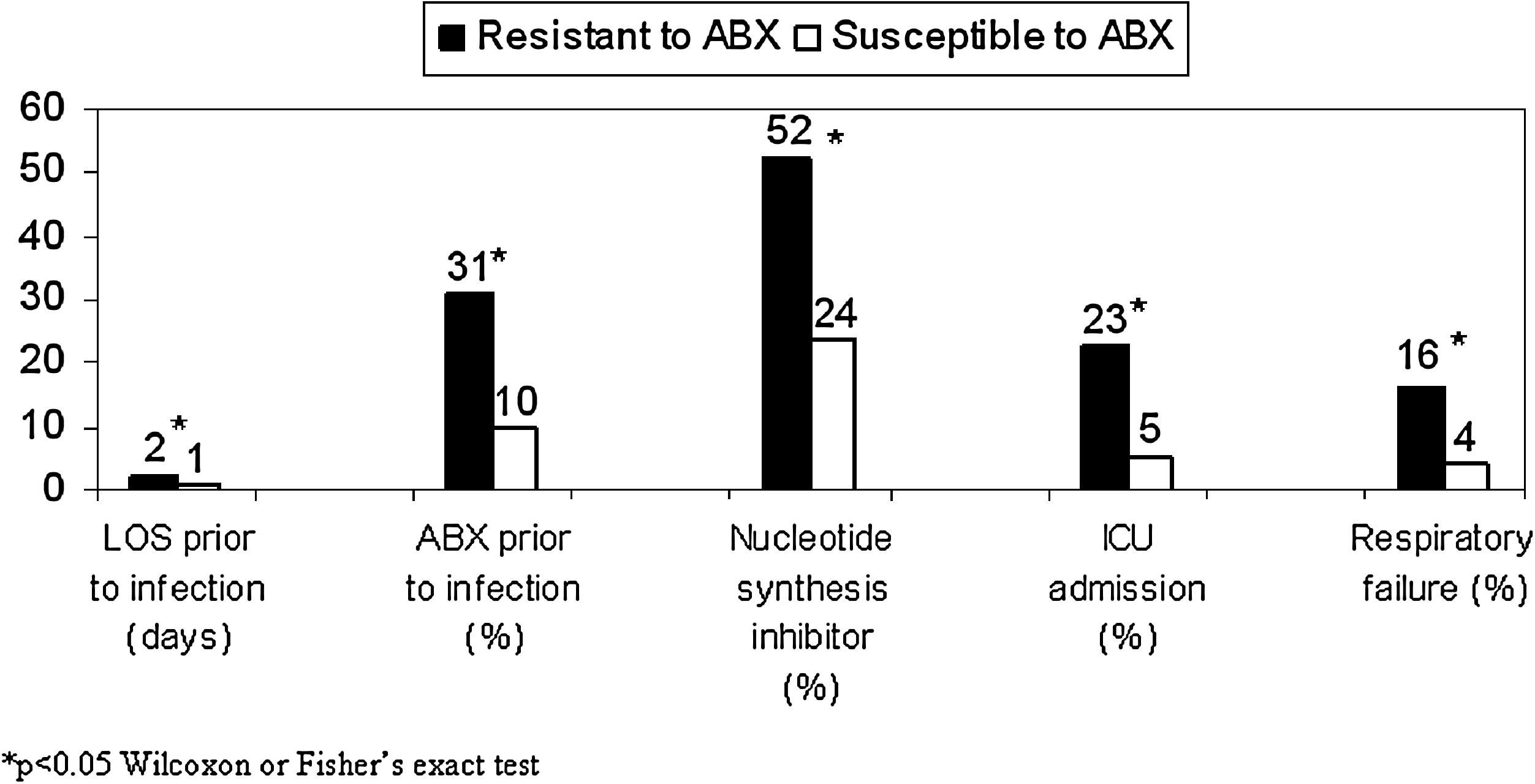
Factors associated with antibiotic resistance in 208 infections. ABX = antibiotic therapy; ICU = intensive care unit; LOS = length of stay.
With regard to the adequacy of antibiotic treatment, patients having 144 (69%) infection episodes received inadequate therapy at T = 0 and 91 (44%) at T = 24. Univariable analysis and variables associated with inadequate antibiotics are summarized in Table 2. Transplant history, co-morbidities, rejection episodes, days from transplant to infection, microbiology results, source of infection, and number of immunosuppressants used were similar in adequately and inadequately treated infections. A significant association with inadequate antibiotic treatment was found for younger age, longer intravenous antibiotic use prior to infection, and greater LOS prior to infection. Failure to administer adequate antibiotic therapy initially was associated with acquired organ dysfunction, and inadequate antibiotic treatment within 24 h was related significantly to cardiovascular shock.
Statistically significant differences are indicated by boldface type.
Wilcoxon rank sum, chi-square, or Fisher exact test.
ICU = intensive care unit; LOS = length of stay.
Immunosuppression was altered in view of the clinical course of the patients, with the general approach being to remove calcineurin inhibitors, reduce antimetabolites, and adjust corticosteroids to stress-dose amounts. There was a trend toward increased use of nucleotide synthesis inhibitor, antibody immunosuppressants, and calcineurin inhibitors in inadequately treated infections at T = 0. Episodes of infection inadequately treated at T = 24 were associated with a clinically relevant longer ICU and hospital LOS. The antibiotic therapy differed widely, with piperacillin-tazobactam and vancomycin being the most frequently administered. Trimethoprim-sulfamethoxazole was used commonly as prophylaxis, and fluconazole was the predominant drug administered for fungal infections.
Multivariable logistic regression was performed to identify factors associated with infection resistant to antibiotics, inadequate antibiotic treatment, or death within 28 days or six mos. Admission to the ICU was significantly associated with an increased percentage of infections resistant to antibiotics (odds ratio [OR] 3.23; 95% confidence ratio [CI] 1.44, 7.25; p = 0.004). Intravenous antibiotic use was the only factor associated significantly with inadequate treatment at T = 0 (OR 3.32; 95% CI 1.56, 7.05; p = 0.001). Increased LOS prior to infection was related significantly to inadequate antibiotic treatment at 24 h (OR 1.042; 95% CI 1.007, 1.078; p = 0.033). Antibiotic resistance by itself was not a significant predictor of death. The presence of heart failure at admission (OR 16.21; 95% CI 2.48, 105.76; p = 0.003), and more acquired organ dysfunctions (OR 10.02; 95% CI 3.43, 29.20; p < 0.0001) were associated significantly with a higher 28-day mortality rate. Factors associated with the six-month mortality rate were a higher number of acquired organ dysfunctions (OR 5.45 95%; 95% CI 2.86, 10.40; p < 0.0001) and inadequate antbiotic treatment at 24 h (OR 3.07; 95% CI 1.40, 6.73; p = 0.020).
Discussion
We found that 31% of adult patients receiving a solid organ allograft had a confirmed infection within one year and 39% of these patients were admitted to the ICU for the infection episode. Most of the bacterial and fungal infections were resistant to antibiotics and were treated inadequately initially. Inadequate antibiotic treatment at 24 h was associated with a higher 28-day mortality rate (14% vs. 2%; p = 0.03). Multiple organisms were the predominant pathogens causing infection after transplantation, followed by CNS and E. coli.
Our infection rates by type of transplant are similar to those reported in the literature. The incidence of infection in pancreas–kidney transplant patients is approximately 50%, with gram-negative bacilli being the primary causative organism [13] and infection the most common cause of death [14]. In pancreas transplant recipients, the incidence of bacteremia and intra-abdominal infection ranges from 12–26% [15,16]. Lung transplant recipients acquire infection in 35–70% of cases in the first month after transplantation, and Pseudomonas aeruginosa is the predominant organism [17,18]. Forty percent of living-donor liver transplant recipients acquire infections in the first month post-transplant, and CNS is the main pathogen [19]. Surgical site infections are a complication in 5% of heart transplant recipients [20]. The likelihood of infection after kidney transplantation differs widely, from 15%–71%, with Enterococcus spp. and E. coli being the most prevalent organisms [21,22].
There was no association between the microbiology results and the type of transplant in our study except for lung transplant infection episodes, which were caused by multiple organisms in 70% of cases. Multiple organisms represented the predominant cause when all solid organ transplant infections were considered. The most common infections caused by multiple organisms were pneumonia (44%) and urinary tract infection (28%).
Reports of the impact of antibiotic resistance on transplant patient outcome have differed and generally are based on retrospective analysis. Lung transplant recipients treated in North America who were colonized with antibiotic-resistant bacteria had a lower survival rate [23], whereas similar patients in Australia did not [24]. The risk of death or graft loss doubled in a Spanish single-center cohort of kidney or double-transplant recipients when multi-resistant bacteria were isolated [25]. The overall mortality rate from bacterial infection in kidney transplant recipients remained constant at 57% at the above center over a ten-year period, whereas the mortality rate from viral infections decreased to 7% and the mortality rate from fungal infections increased to 36% [26]. Liver transplant recipients with VRE infection in Cincinnati had a lower survival rate and used more hospital resources [27], whereas multiple drug-resistant bacterial infections in a similar cohort in Brazil did not influence survival significantly [28]. Liver transplant recipients who acquired VRE after transplantation had a significantly higher mortality rate and longer LOS than those colonized with VRE prior to transplantation or those without VRE [29]. In our study, antibiotic-resistant infections were associated significantly with increased antibiotic use, longer LOS, and nucleotide synthesis inhibitor use prior to infection. Our population of solid organ transplant recipients had a worse clinical outcome if infected with antibiotic-resistant organisms, a situation associated with a higher percentage of respiratory failure and ICU admission. On the other hand, the presence of antibiotic-resistant organisms covered by appropriate antibiotics had no impact on the mortality rate.
In our study, younger age was associated with inadequate antibiotic treatment, whereas in most studies, older age has been a risk factor for developing infections. We did not find a relation between female sex and a higher mortality rate, contrary to what was seen 15 years previously at our institution [30]. Increased antibiotic use was associated with inadequate antibiotic treatment initially, and a longer LOS prior to infection was associated with inadequate antibiotic therapy at 24 h. Patients treated inadequately initially were more likely to have received antibody and other immunosuppressants. The impact of inadequate antibiotic treatment at 24 h on the 28-day mortality rate was statistically significant, and its impact on ICU and in-hospital LOS was clinically relevant.
The limitations of our study include its retrospective design in a single center where multiple physicians provided care to a heterogeneous transplant population. Although all transplant patients seen during the year were screened for inclusion, only 114 met the entry criteria, so caution must be used in extending our results. We applied well-recognized definitions of infection and resistance, but in clinical practice, not all information required for these determinations is recorded, as would be done in a prospective trial. Given the retrospective nature of this study, we were not able to control the alterations of immunosuppression when an infection was suspected or documented, and these changes were not guided by a single protocol. Ethical concerns preclude conducting a randomized study to evaluate the impact of inadequate antibiotic treatment on survival. Our results did not support a negative impact on the mortality rate attributable only to the presence of resistant organisms in culture. However, when inadequate antibiotic therapy was provided initially and at 24 h after diagnosis, the impact on the mortality rate was significant. All patients with lethal outcomes at 28 days were treated inadequately with antibiotics initially.
Conclusions
Inadequate antibiotic therapy at 24 h had a significant impact on the 28-day mortality rate. A majority of infections in solid organ transplant recipients were resistant to antibiotics and were treated inadequately initially. Prior intravenous antibiotic use and greater LOS prior to infection were associated with antibiotic resistance and inadequate antibiotic therapy. Failure to provide adequate antibiotic therapy within 24 h was associated with a detrimental clinical outcome. In case of pneumonia or in a clinical setting suggesting multiple organisms in lung or liver transplant recipients, early broad-spectrum antibiotic therapy designed to cover resistant organisms should be instituted followed by de-escalation when culture results are available.
Footnotes
Acknowledgments
The authors thank David Radosevich, RN, PhD, Director of Transplant Information Services, University of Minnesota, for providing support in identifying the transplant patients screened for infection.
Author Disclosure Statement
No competing financial interests exist.
*
Presented at the 28th Annual Meeting of the Surgical Infection Society, Hilton Head Island, South Carolina, May 7–9, 2008.