
Abstract
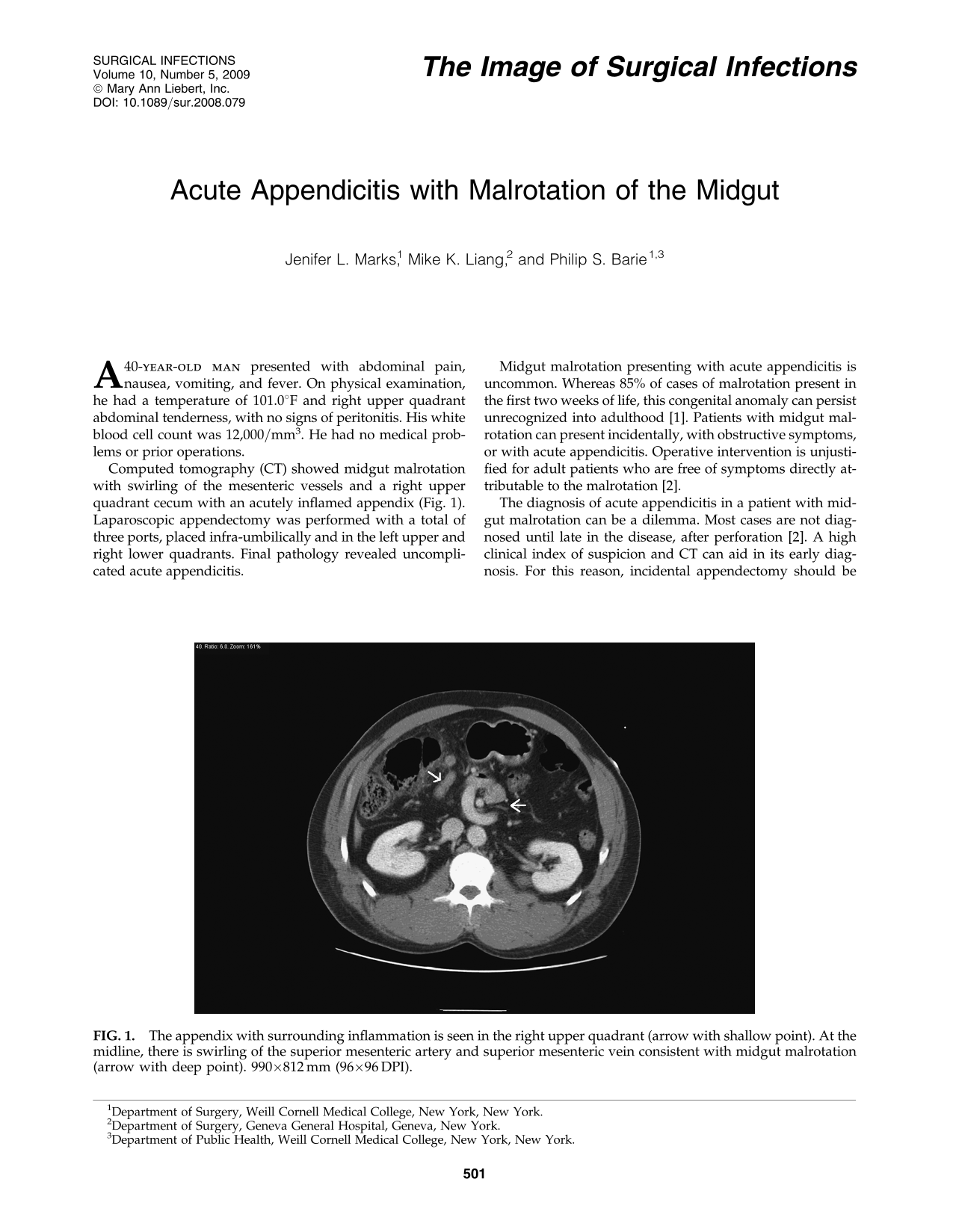
Computed tomography (CT) showed midgut malrotation with swirling of the mesenteric vessels and a right upper quadrant cecum with an acutely inflamed appendix (Fig. 1). Laparoscopic appendectomy was performed with a total of three ports, placed infra-umbilically and in the left upper and right lower quadrants. Final pathology revealed uncomplicated acute appendicitis.

The appendix with surrounding inflammation is seen in the right upper quadrant (arrow with shallow point). At the midline, there is swirling of the superior mesenteric artery and superior mesenteric vein consistent with midgut malrotation (arrow with deep point). 990 × 812 mm (96 × 96 DPI).
Midgut malrotation presenting with acute appendicitis is uncommon. Whereas 85% of cases of malrotation present in the first two weeks of life, this congenital anomaly can persist unrecognized into adulthood [1]. Patients with midgut malrotation can present incidentally, with obstructive symptoms, or with acute appendicitis. Operative intervention is unjustified for adult patients who are free of symptoms directly attributable to the malrotation [2].
The diagnosis of acute appendicitis in a patient with midgut malrotation can be a dilemma. Most cases are not diagnosed until late in the disease, after perforation [2]. A high clinical index of suspicion and CT can aid in its early diagnosis. For this reason, incidental appendectomy should be performed in patients with midgut malrotation undergoing intra-abdominal surgery for other reasons. The typical treatment for intestinal obstruction with midgut malrotation is a Ladd procedure and appendectomy [3].
Footnotes
Author Disclosure Statement
J.L. Marks, M.K. Liang, and P.S. Barie have no disclosures.