
Abstract
Abstract
Background:
Recent data suggest that the timing of fluid resuscitation and the type of fluid used to treat hemorrhagic shock contribute to the inflammatory response as well as cell death.
Methods:
Rats were bled of 40% of their total blood volume and then resuscitated in either early or delayed fashion. Treatment was assigned randomly and consisted of lactated Ringer's solution, normal saline, bicarbonate Ringer's solution, hypertonic saline, or no resuscitation. The first four groups were subdivided into early and late resuscitation. After a 5-h observation period, lung and liver samples were evaluated for apoptosis, and blood was collected for measurements of the cytokines interleukin (IL)-6, IL-10, and IL-1β.
Results:
The rats that were not resuscitated had significantly more apoptosis in liver tissue. In the lung, bicarbonate Ringer's solution, when given early, was associated with significantly less apoptosis. Non-resuscitated rats had significantly higher IL-6 concentrations than all other groups. Animals receiving hypertonic saline early had significantly higher IL-6 concentrations than those given any other fluid. The concentration of IL-1β was significantly higher in the non-resuscitated rats than in those receiving bicarbonate Ringer's, lactated Ringer's, or normal saline for early resuscitation. Interleukin-10 was elevated significantly in non-resuscitated rats.
Conclusions:
Cellular destruction and a pro-inflammatory response follow hemorrhagic shock. Early resuscitation with isotonic crystalloid fluids decreases these responses.
The treatment protocols used today for hemorrhagic shock are based on many clinical and basic science studies. It is recommended that early treatment include control of external bleeding and administration of crystalloids through a large-bore needle [6]. Previous experiments have shown the benefits of such treatment, including maintenance of tissue perfusion, attenuation of cytokine production, and reversal of cellular swelling and injury [7–13]. In a recent study, crystalloid resuscitation caused less interference with thrombin generation, clot formation, and platelet activation than did resuscitation with hyper-oncotic solutions [14].
However, over the last two decades, clinical trials and experimental models of hemorrhagic shock have challenged the current standard of care [15–17,20]. A major debate continues regarding the timing of fluid resuscitation. Some studies have led many to believe that early fluid infusion, prior to surgical control of hemorrhage, may increase bleeding secondary to elevated blood pressure, disruption of the clot forming at the site of vascular injury, and dilution of clotting factors [15,16,21]. However, other studies suggest benefits of early fluid infusion after hemorrhagic shock. We previously reported decreased interleukin (IL)-6 concentrations, increased urinary output, and a lower mortality rate with early resuscitation [22]. In a recent study by Lee et al., production of pro-inflammatory cytokines correlated directly with the time delay necessitated by resuscitation [23]. Also supporting early fluid infusion are results from a study of uncontrolled hemorrhagic shock, in which intestinal apoptosis was less extensive in animals receiving early resuscitation [24].
In addition to the timing of resuscitation, many are puzzled about which type of fluid to administer. Resuscitation with crystalloid has a long history of success [7–14]. There are more recent reports revealing other benefits of crystalloid use, such as decreased systemic apoptosis and a higher glomerular filtration rate and renal blood flow within the first 60 min after hemorrhage [25,26]. Conversely, resuscitation with hypertonic saline is gaining support through a purported association with such qualities as better gut protection, attenuation of neutrophil activity, and balanced profile of T-lymphocyte subpopulations [27–31]. Resuscitation using hydroxyethyl starch solutions in animal models indicated a protective effect on the intestines and less oxidative stress [32,33]. Another alternative, hemoglobin-based oxygen carriers, improved hemodynamic parameters, reversed anaerobic metabolism, and decreased transfusion requirements in swine models of controlled and uncontrolled hemorrhage [34–39]. Despite the many favorable results using an assortment of fluids, they all have been linked to some negative side effects, making the selection of the optimal fluid even more perplexing [25,40,41].
We hypothesized that early fluid resuscitation results in less systemic injury than delayed resuscitation when an appropriate anesthetic and volume of fluid is utilized to treat hemorrhagic shock. This study evaluated several systemic responses to early and delayed resuscitation using various types of fluids.
Materials and Methods
Animals
The Institutional Laboratory Animal Review Board for the care and use of animals approved this study. All research was conducted in compliance with the Animal Welfare Act and other federal statutes and regulations relating to animals and experiments involving animals, and the study adhered to the principles in the National Research Council Guide for the Care and Use of Laboratory Animals.
Male Sprague-Dawley rats weighing 250 to 400 g were anesthetized with an intraperitoneal injection of sodium pentobarbital (50 mg/kg), and 1% lidocaine was injected at the surgical site to achieve local anesthesia. Animals were maintained on small doses (5 mg) of pentobarbital as needed throughout the experiment. Using aseptic technique, a tracheostomy was performed, followed by cannulation of the right common carotid artery and the right internal jugular vein with Intramedic polyethylene catheters (PE 50; BD Diagnostics, Franklin Lakes, NJ) filled with heparin 10 U/mL. The mean arterial pressure (MAP) was monitored by connecting the arterial catheter to a pressure transducer (Harvard Apparatus, Holliston, MA). Animals were allowed to breathe spontaneously for the duration of the experiment. A mini-laparotomy was performed and the liver parenchyma exposed for measuring resting membrane potentials utilizing a modified Ling-Gerard microelectrode [42,43]. The animals were kept on a temperature-controlled surgical board (37° ± 1°C) for the duration of the experiment.
After systemic heparinization (250 U/kg), animals were bled from the carotid catheter over 20 min to remove 40% of their blood volume. The blood outflow was one-third of the total in the first 5 min, one-third in the second 5 min, and the final one-third over the last 10 min [24].
The animals were randomized into the following groups: No resuscitation (NR), lactated Ringer's solution (LR), normal saline (NS), hypertonic saline (HTS), and bicarbonate Ringer's solution (BR). Animals in the LR, NS, BR, and HTS groups were then subdivided into two sets. In the first set, resuscitation began 15 min after hemorrhagic shock was induced (early group). In the second set, resuscitation began 60 min after hemorrhagic shock (delayed group). The LR, NS, and BR groups received fluids 80 mL/kg via the venous line over 20 min. The HTS rats received 7.5% NaCl at 5 mL/kg over 10 min. A normal control (NC) group (anesthesia only) and a sham-treatment group (surgery, no hemorrhage, and no resuscitation) were included. There were 11 animals per group.
Fluid administration
The components of the fluids are shown in Table 1. The BR and HTS solutions were filtered (0.22 micron, polyestersulfone; Millipore, Billerica, MA) and tested for pyrogens by the Limulus assay (Limulus Amebocyte Lysate ACL-1000; Lonza Inc., Rockland, ME). All fluids were infused at room temperature.
The pH was 6.0–7.5 for all fluids.
Five states were studied: Pre-shock, early shock, late shock, fluid resuscitation, and recovery (5 h after hemorrhage). The following parameters were evaluated: MAP, body temperature, and resting transmembrane potential of the liver. Hepatic resting membrane potentials were measured at baseline, end of hemorrhage, and 180 min and 300 min post-hemorrhage. Liver and lung tissue (0.5–1 g) were collected 5 h after the hemorrhage. Blood samples were collected at baseline (1.0 mL) and 90 min (1.0 mL) and 300 min (4–6 mL) post-hemorrhage. The amount of fluid needed to replace the loss was returned 90 min after blood sampling so as to not affect the percent of blood loss. The NR and sham-treatment groups received NS at this time point. Animals were euthanized with an overdose of pentobarbital.
DNA isolation and analysis
Genomic DNA was extracted from lung and liver tissue using the MasterPure DNA Purification kit (Epicentre Technologies, Madison, WI) [44]. Tissues were homogenized in lysis buffer (proteinase K [50 mcg/mL] and tissue and cell lysis solution) and incubated at 65°C for 15 min, with vortexing every 5 minutes. Samples were treated with RNase A (5 mcg) at 37°C for 30 min. Nucleoproteins were precipitated with the addition of MPC Protein Precipitation Reagent followed by centrifugation at 10,000 × g at 4°C for 10 min. The DNA was precipitated with isopropanol followed by centrifugation at 10,000 × g at 4°C for 10 min. The resulting DNA pellet was washed twice with 70% ethanol, air dried, and resuspended in TE buffer (10 mmol/L Tris HCl, 1 mmol/L ethylenediaminetetraacetic acid, pH 8.0). The DNA concentration was determined by ultraviolet spectrophotometry (OD260).
Apoptosis was assessed with the ligation-mediated polymerase chain reaction (LM-PCR). This assay uses PCR to amplify nuclear DNA fragments resulting from apoptosis [45]. The apoptosis-generated DNA fragments have blunt ends to which oligomers are ligated. Nuclease-free water, Takara 10 × ligase buffer (Fisher Scientific, Pittsburgh, PA), 24-bp nucleotide oligomer (5′-AGCACTCTCGAGCCTCTCACCGCA-3′; Sigma-Aldrich, St. Louis, MO [500 pmol]), and 12-bp nucleotide oligomer (5′-TGCGGTGAGAGG-3′; [500 pmol]), which constitute the ligation mix (35 mcL), were added to the genomic DNA (0.5 mcg). The reaction mixture was heated to 55°C for 10 min in a thermal cycler (Model PTC-100; MJ Research Inc., Watertown, MA) followed by a gradual temperature ramp down to 10°C over a 1-h period followed by a final 10°C incubation for 10 min prior to addition of ligase. Takara T4 DNA ligase (200 units/reaction; Fisher Scientific) was added to reaction mix and incubated at 16°C for 16 h. The 24-bp oligomer was ligated to the 5′-phosphorylated end, whereas the 12-bp nucleotide oligomer complementary to it was situated at the 3′-hydroxyl end. Because only the 24-bp oligomer was actually ligated at the 5′ end, the 12-bp oligomer was released by heating the product in the thermal cycler, leaving a 24-bp 5′ overhang. Adaptor-ligated DNA (50 ng from lung or 150 ng from liver) was added to nuclease-free water, 10 × cDNA PCR reaction buffer, 50 × dNTP mix (32 nmol each), 50 × Advantage cDNA polymerase mix, and 24-bp oligomer (124 pmol) to act as primer for a 100-mcL amplification volume. Amplification was then performed by PCR, at 23 cycles of 1 min at 94°C and 4 min at 72°C with a post-cycling extension for 15 min at 72°C. Prior to each experiment, PCR control samples were run using glyceraldehyde-3-phosphate dehydrogenase (G3PDH) to ensure an equivalent amount of sample DNA was used for each experiment. Nuclease-free water, 10 × cDNA PCR reaction buffer, 50 × dNTP mix (10 nmol each), G3PDH primer set (20 pmol each), and 50 × Advantage cDNA polymerase mix was added to genomic DNA (0.5 mcg) for a 50-mcL control reaction volume. Control samples were run at 26 cycles of 1 min at 94°C, 1 min at 70°C, and 1 min at 72°C. Polymerase mix, cDNA PCR buffer, dNTP mix, and G3PDH primers were obtained from Clontech (Mountain View, CA).
The nuclear DNA laddering effect was seen by resolving the PCR products on a 1.2% agarose gel, followed by incubation of the gel with Sybr Green (Lonza). Semi-quantitation of apoptosis in the samples was done using VisionWorks Image Acquisition Software (UVP Inc., Upland, CA).
Cytokine assays
Three cytokines (IL-1β, IL-6, and IL-10) were measured in serum samples using a commercially available multiplex bead immunoassay kit (Rat Cytokine 10-Plex and Rat Cytokine IL-6 singleplex kit; Invitrogen, Camarillo, CA). All samples were read in a Luminex 200TM instrument (Luminex Corp., Austin, TX) and analyzed using Starstation software (Applied Cytometry Systems, Sacramento, CA).
Statistical analysis
All data are presented as a group means ± standard error of the mean. The SPSS statistical software program (SPSS, Chicago, IL) was used to perform a power analysis to determine the number of animals per group as well as one-way analysis of variance with post-hoc Bonferroni and Dunnett tests for multiple comparisons between groups for mean MAP, hepatic membrane potentials, and apoptosis. A one-tail t-test was used for all the cytokine analyses. A p value of ≤ 0.05 was considered statistically significant.
Results
Pre-shock MAP values were not significantly different from normal in any group. At the end of hemorrhage (shock), MAP was significantly lower in all groups than in the sham-treated animals (Table 2). At the 35-min time point, the MAP in the animals resuscitated early by any method had increased to near-baseline values and was significantly higher than in the NR rats. For the delayed fluids, because resuscitation had not yet begun, MAP results at 35 min were essentially equivalent to those of the shock period. At both the 80- and 180-min time points, all early resuscitation groups had MAP values significantly higher than the NR rats but significantly lower than the sham-treated rats. At 80 min (equivalent to the end of delayed resuscitation), all delayed resuscitation groups had significantly higher MAP values than the NR group. Early resuscitation groups had significantly higher MAP than the NR rats, but significantly lower values than the delayed and sham-treatment rats. This can be explained by the fact that delayed fluid resuscitation (i.e., volume expansion) had just been completed. In the case of the BR rats, however, there was no significant difference between early and delayed resuscitation. This may indicate that the animals given BR early had better maintenance of intravascular volume. At 180 min, the values for the sham-treated animals were significantly higher than those for all others, and NR was lower than all others except the LR group. The animals having early and delayed resuscitation had equilibrated and were not significantly different. At 300 min, the blood pressure measurements were the same for all groups except BR. The MAP was significantly higher than in the NR animals, but significantly lower than in the sham-treated rats. Rats resuscitated early with BR had a significantly higher MAP than NR rats and those given the fluid in a delayed fashion, but the difference was not significant compared with sham treatment, indicating a return to baseline. When the fluids were compared, BR produced significantly higher MAP than NR, LR, or HTS.
Hepatic resting membrane potential results are shown in Table 3. For measurements obtained at shock, 180 min, and 300 min, all treatment groups had significantly higher potentials than the sham-treatment group. Thereafter, the potentials trended toward but never reached baseline values, with NR maintaining the greatest distance from baseline and NS-E coming closest. Only HTS-E animals continued to have a higher potential, which was similar to that in the NR group at 300 min, and HTS was the only fluid producing values not significantly different from NR at 300 min.
Apoptosis is expressed in percent difference from the NC rats. When the liver samples were analyzed, among the animals that were resuscitated early, there was no significant difference in apoptosis according to the fluid used (Fig. 1). However, NR rats had significantly more apoptosis than all resuscitation groups, as well as the NC and sham-treated rats. With delayed resuscitation, NR rats had significantly more apoptosis than the NC, sham-treated, NS-D, and LR-D animals. The HTS-D rats also had significantly more apoptosis than the NC rats. Each fluid was compared in its early and delayed applications, and for NS and LR, the only difference was that all fluids were associated with significantly less apoptosis than was found in the NR rats. The BR-E group had significantly less apoptosis than the NR rats, and the BR-D rats had significantly more apoptosis than the NC rats. This was also the case for the HTS rats.
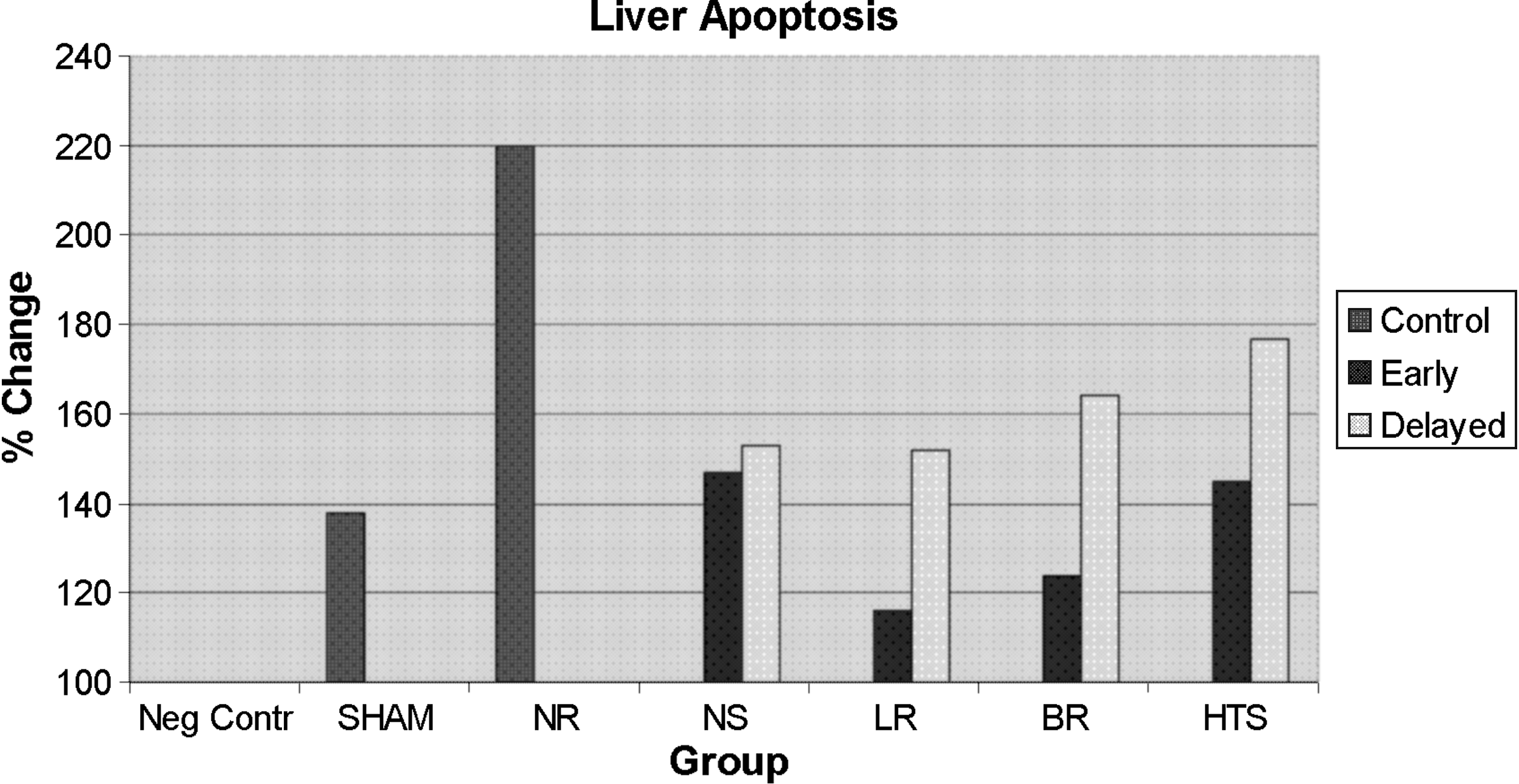
Apoptosis in liver tissue. (See text for abbreviations.)
The results for lung apoptosis are shown in Figure 2. Here, NC rats had significantly less apoptosis than all others except BR-E. The BR-E animals had significantly less lung apoptosis than either NR or BR-D rats.

Apoptosis in lung. (See text for abbreviations.)
The NC animals had significantly lower IL-6 concentrations than the other groups, the cytokine being undetectable in these animals (Fig. 3). In animals resuscitated early, only sham-treated rats had significantly lower concentrations of IL-6 than the HTS-E rats. All three other fluids (NS-E, LR-E, and BR-E) were associated with significantly lower IL-6 concentrations than HTS-E. When delayed resuscitation protocols were compared, however, only the NS-D rats had IL-6 concentrations similar to those in the sham-treated animals, whereas the LR-D, BR-D, and HTS-D rats all had significantly higher IL-6 concentrations. The HTS-D animals had significantly higher IL-6 concentrations than those given NS-D or LR-D. When early resuscitation was compared with delayed fluids, BR-E was significantly lower than BR-D.
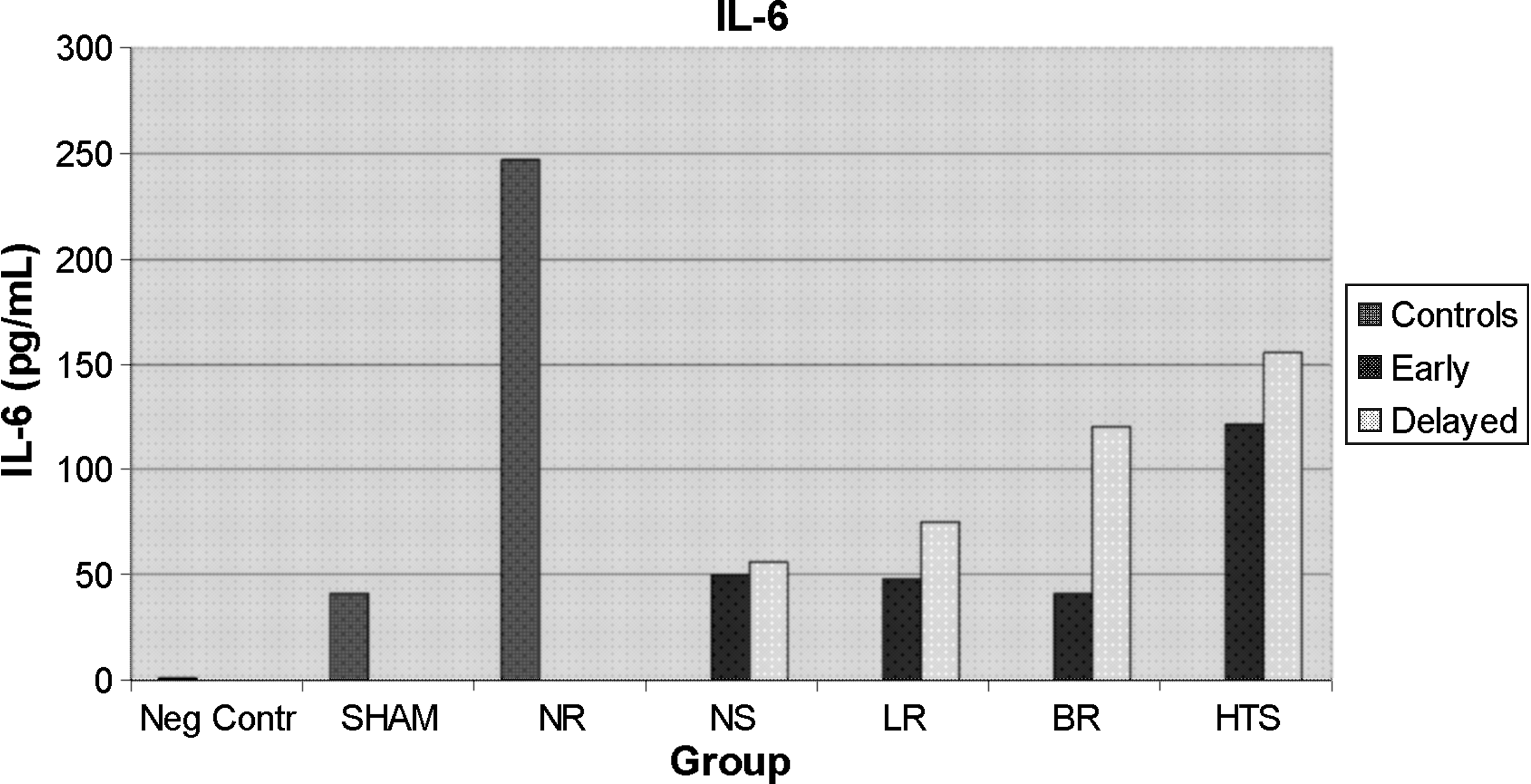
Concentration of interleukin-6 in rats during shock and resuscitation. SHAM = sham treatment; NR = no resuscitation; NS = normal saline; LR = lactated Ringer's, BR = bicarbonate Ringer's; HTS = hypertonic saline.
The NR rats had significantly higher IL-1β concentrations than BR-E, LR-E, NS-E, and NC animals (Fig. 4). The NS-E rats had significantly lower IL-1β concentrations than either sham-treated or LR-E rats or the NR animals. Sham-treated rats had significantly lower IL-10 concentrations than HTS-E, LR-E, NR, and NC rats (Fig. 5). In addition, NR rats had significantly higher IL-10 concentrations than NS-E, LR-E, and BR-E animals.

Concentration of interleukin-1β in rats during shock and resuscitation. Abbreviations as in Fig. 3.
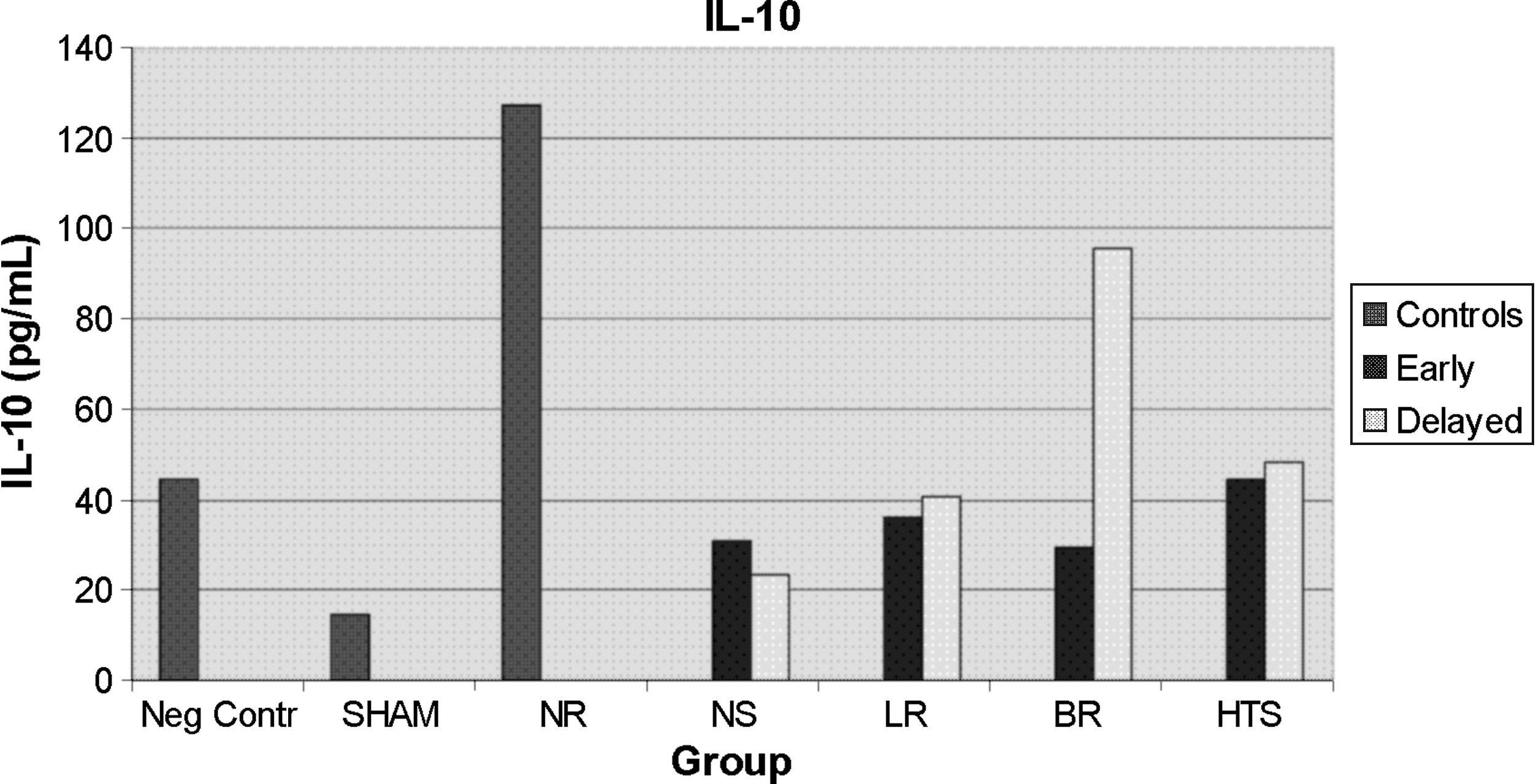
Concentration of interleukin-10 in rats during shock and resuscitation. Abbreviations as in Fig. 3.
Discussion
Recently, interest in delaying fluid resuscitation for hemorrhagic shock has been renewed because of concerns that early crystalloid resuscitation may increase hemorrhage when surgical hemostasis has not yet been achieved. That is, some authors believe that large boluses of fluid can increase blood pressure, which may disrupt clot, as well as dilute clotting factors [46]. Varicoda et al. studied a model of hemorrhagic shock created by a splenic and vascular injury, a realistic replication of a common injury resulting from blunt trauma. These investigators were unable to document any increase in blood loss with resuscitation with LR from that seen with hypertonic saline with dextran or in untreated control animals [47]. The untreated controls in their report correspond reasonably well to the delayed resuscitation groups in the current trial. Thus, Varicoda et al. refuted the claim that early resuscitation, particularly with isotonic crystalloids, is associated with greater blood loss.
Recent studies using hypertonic saline for resuscitation in hemorrhagic shock have touted multiple benefits over isotonic solutions [48–51]. For example, Chen et al. described an increase in pro-inflammatory mediators in association with isotonic fluid resuscitation in an animal study of hemorrhagic shock that was not seen with hypertonic saline or hyper-oncotic fluids [48]. Gurfinkel et al. found that pulmonary perivascular edema was less severe with hypertonic saline resuscitation, which also was associated with a decrease in both IL-6 and tumor necrosis factor (TNF)-α in a rat model of hemorrhagic shock [50]. Powers et al. studied neutrophil counts in bronchoalveolar lavage fluid in an animal model of hemorrhagic shock followed by lipopolysaccharide administration [51]. This group of investigators described higher concentrations of the anti-inflammatory cytokine IL-10 and less pro-inflammatory mediator, tumor necrosis factor (TNF)-α, after resuscitation with hypertonic saline.
In the current model of hemorrhagic shock, for a number of reasons, we chose to use a controlled blood loss model. First, we wanted to ensure accurate calculations for resuscitation fluid volumes. Second, this model enabled us to induce a more severe shock state than was used in prior studies [22,25]. Third, this model more closely replicates a common clinical scenario in which massive transfusion protocols are recommended.
In this study, we demonstrated more liver apoptosis in NR rats than in resuscitated rats when the fluids were given early. This finding indicates that more apoptosis is associated with the shock state alone, not with a particular resuscitation fluid. Furthermore, when hypertonic saline was given, apoptosis was more common than with all other fluids. Although delayed resuscitation in the BR-D and HTS-D groups was associated with more apoptosis in the liver than was seen in NC animals, there was no difference in apoptosis rates from that in the sham-treated rats. In the lung, we found the least apoptosis in the BR-E resuscitated animals, with little difference in the other groups. Similar to our current results, we previously reported that apoptosis and cell death occur as a result of the shock state itself, not in relation to the resuscitation fluid [25]. This is evidenced by greater extents of apoptosis in NR rats than in animals resuscitated using a variety of fluids [25]. Lu et al. evaluated dosing of fluid resuscitation and how it may affect uncontrolled hemorrhage. In their research, fluid doses of 40 mL/kg decreased apoptosis in liver, kidney, and small intestine compared with a more aggressive 80 mL/kg dose in a model with either controlled or uncontrolled hemorrhage [24,52]. That model supports the theory that controlled resuscitation with smaller doses of fluid should be given, even prior to surgical hemostasis [24,52]. Gonzalez et al. created a model to study how standard resuscitation may worsen ischemia–reperfusion injury by occluding the superior mesenteric artery and administering various resuscitation fluids after reperfusion. Although those investigators found less mucosal injury on histologic sections in the animals treated with hypertonic saline, they documented more apoptosis in the same animals [53]. This result is similar to the increases in apoptosis seen in association with hypertonic saline in the current study.
Cytokines have significant roles in the early host response to shock [22]. Interleukin-6 is a pro-inflammatory cytokine involved in immunoglobulin production along with inflammation. Higher IL-6 concentrations or greater IL-6 to IL-10 ratios correlate well with injury severity and the development of organ dysfunction [23]. Interleukin-10 concentrations, on the other hand, are associated with anti-inflammatory mechanisms, including inhibition of the production of pro-inflammatory cytokines. Contrary to our results, some researchers have found decreased pro-inflammatory cytokines or higher concentrations of anti-inflammatory cytokines with hypertonic as opposed to isotonic solutions [48–51]. However, one such study, by Gurfinkel et al., used MAP as an indicator for shock instead of ensuring a shock state by bleeding the animals a set amount [50]. Hoyt points out that use of blood pressure or urine output as the only endpoint for resuscitation may lead to under-resuscitation [49]. Also, the animals in the study by Gurfinkel et al. were resuscitated rapidly (in approximately half the time we used). Finally, those investigators continued to treat all animals with normal saline to maintain a certain blood pressure during the observation period. This makes it difficult to determine whether their results truly are attributable to hypertonic saline resuscitation or to isotonic maintenance [50]. Other studies have used similar rapid infusion rates, or have had a small number of animals in each group, without any comment on power of analysis [54]. Others actually report no significant difference in cytokine concentrations according to the fluid given [30].
Many other researchers have results that support our theories and are consistent with the findings of this laboratory. Lee et al. recently investigated the effects of early vs. delayed fluid resuscitation on cytokine concentrations and histopathologic effects in lung tissues in a volume-controlled hemorrhagic shock model. They found significantly a higher concentration of IL-6 in the groups in which resuscitation fluid was delayed by 45 or 60 min [23]. In previous studies, we examined both different doses of fluid resuscitation and the timing of resuscitation [22]. In that study, we found that IL-6 concentrations were lower in the early resuscitation groups whatever the fluid composition. Early fluid resuscitation also maintained urine output and hepatic resting membrane potential better than did delayed resuscitation, and resulted in a lower mortality rate. In the present study, a higher IL-6 concentration was seen only in early resuscitation with hypertonic saline. This modulation of cytokines with hypertonic saline calls into question other studies that indicate hypertonic saline is associated with better immune function. The delayed fluids did not have quite the same effect, however. Here, all the animals except those resuscitated with NS-D had significantly higher IL-6 concentrations than sham-treated rats. However, the HTS-D animals had even higher concentrations than those receiving other fluids in delayed fashion, reaching significance compared with NS-D and LR-D. Therefore, all animals resuscitated early and even most of those resuscitated in a delayed fashion had lesser inflammatory responses than those given hypertonic saline, with IL-6 concentrations being similar to those in sham-treated animals. Although the concentrations of IL-10 were significantly higher in the NR group, the IL-6 concentrations were elevated more dramatically. Thus, the ratio of IL-6 to IL-10 was greater in the NR animals than in the resuscitated animals, resulting in a more intense pro-inflammatory response.
Despite the concerns about the effects of early fluid resuscitation on tissue, the effects of prolonged shock on patients who have fluid resuscitation delayed cannot be overlooked. The results in the delayed resuscitation groups in the present study may be explained in part by ischemia–reperfusion injury. Resuscitation after shock likely is an initiating factor in the pro-inflammatory response [53]. In addition, concerns regarding the disadvantages of hypertonic saline cannot be ignored. Hypertonic saline may cause poorer outcomes because of dehydration, existing hypernatremia, or volume overload [55]. In this study, ten rats died prior to the end of the study period: Three NR rats, one LR-D rat, three HTS-E rats, and three HTS-D rats. Thus mortality rate clearly was higher in association with resuscitation using hypertonic saline at either time in this model.
The fluid debate likely will continue because of the variations in models of hemorrhagic shock and the complexity of the physiology associated with them. For a large majority of patients, current approaches using isotonic crystalloid solutions likely are safe and effective [56]. This animal study supports the view that the benefits of early fluid resuscitation clearly outweigh the risks. These benefits are evidenced by restoration of MAP and the impacts on hepatic membrane potential, the amount of apoptosis, and the balance of pro-inflammatory and anti-inflammatory cytokines. Additionally, we saw no benefit to the use of hypertonic saline. The resuscitative fluid with the best formulation is likely yet to be delineated, and additional clinical trials are needed to confirm the encouraging findings found in animal models of resuscitation from hemorrhagic shock.
Footnotes
Acknowledgments
This paper is dedicated to the memory of Dr. G. Tom Shires, who guided and inspired the work done in this laboratory for many years.
We thank April Johnson, Ayoub Ayoub, Michael Benassi, David Holland, Gayle Johnson, Vanessa Stevens, and Christopher Madsen for their technical assistance in the completion of this work.
No competing financial interests exist for any of the authors.
Author Disclosure Statement
No conflicting financial interests exist.
Presented at the Memorial Celebration and Festschrift for Doctor G. Tom Shires, New York, New York, October 25, 2008.