
Abstract
Abstract
Background:
Streptococcus suis is a common infection of pigs. Human infection is often related to accidental inoculation through skin injuries during occupational exposure to pigs and pork. The disease may present as meningitis, bacteremia, and less commonly endocarditis, arthritis, or bronchopneumonia.
Methods:
Case report and review of the literature.
Results:
We report a case of bacteremia and severe sepsis caused by S. suis serotype 2 complicated by septic arthritis in a 56-year-old male with history of a prior contact with unprocessed pork. The causative agent was isolated from blood cultures and aspirated synovial fluid. The patient's condition improved after treatment with penicillin, but he was found subsequently to have an abdominal aortic aneurysm, confirmed by computed tomography (CT) scan. The mycotic aneurysm was successfully repaired using an in situ graft reconstruction. Tissue samples analyzed using polymerase chain reaction identified S. suis serotype 2 as the causative organism. After completion of two weeks of parenteral antibiotics, an oral form of ciprofloxacin (0.25 g twice a day) was continued for one month. The patient was discharged from our institution after uncomplicated recovery. Clinical review, a CT scan, and inflammatory markers nine months after surgery revealed no evidence of infection.
Conclusion:
This is the first report of mycotic aneurysm caused by S. suis, which may be an etiologic agent of mycotic aneurysms, especially when complicated by bacteremia in adults with a recent history of contact with pigs or unprocessed pork.
Case Report
A 56-year old male was admitted to the Chiang Mai Provincial Hospital with a history of fever and painful left knee swelling. Cultures of blood and aspirated fluid from the left knee joint grew S. suis. The patient had a history of consuming unprocessed pork. After four weeks of intravenous penicillin G (3 million units intravenously q 4 h), his fever and knee swelling subsided, he could walk normally, and he was discharged. Two weeks later, he presented with a pulsating, painful, central abdominal mass. Abdominal ultrasonography revealed the presence of an infrarenal abdominal aortic aneurysm (AAA), and the patient was referred to our institution for surgical intervention. The period between bacteremia and occurrence of the AAA was six weeks.
Upon admission, the patient complained of central abdominal pain. His initial temperature was 38.2°C, with blood pressure of 140/90 mm Hg and a heart rate of 110 beats/min. Physical examination revealed a palpable, tender, pulsating central abdominal mass (4x4 cm). He had a WBC count of 7,500/mm3 (63% neurophils and 20% lymphocytes), a hemoglobin concentration of 12 g/dL, and a platelet count of 263,000/mm3. C-reactive protein was 110 mg/L, with an erythrocyte sedimentation rate of 120 mm/h. Electrolyte concentration and renal function tests were within normal limits. A contrast computed tomography (CT) scan of the abdomen revealed a 37 mm diameter fusiform abdominal aortic aneurysm located just above the aortic bifurcation without iliac artery involvement but with surrounding inflammation (Fig. 1) Transthoracic echocardiogram revealed no evidence of endocarditis.
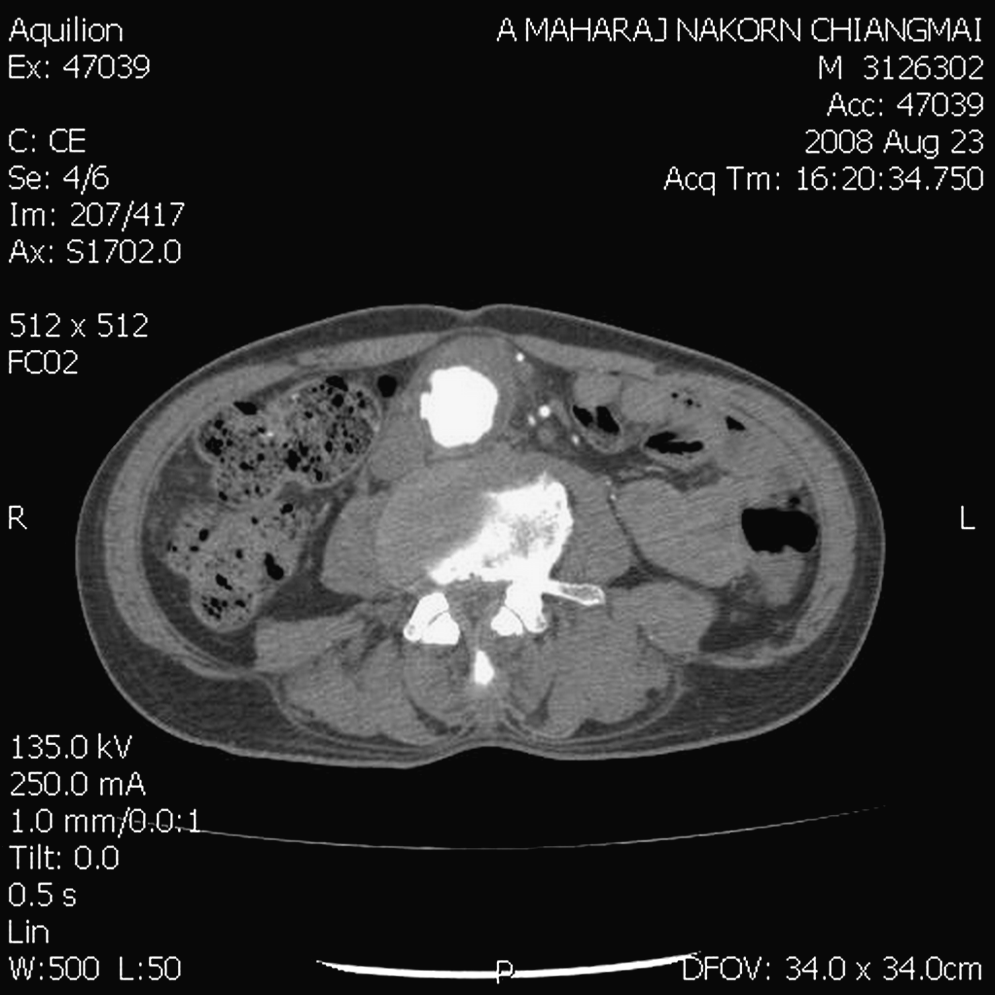
Computed tomography scan of the abdomen revealed a fusiform dilatation of the abdominal aorta just above the aortic bifurcation measuring approximately 6 cm in length and 3.7 cm in transverse diameter, with a crescentic mural thrombus measuring approximately 1 cm in maximal thickness. There is an irregular thickening enhancing the aortic wall in the dilated segment. The inflammation is also seen in the surrounding tissue and lymph nodes.
After he had been given ceftriaxone intravenously (2 g every 12 h) for 14 days, exploration was performed through a midline abdominal incision, and a fusiform aneurysm, 4 cm in diameter located 3 cm above the aortic bifurcation, was exposed and resected. Tissue samples from the involved aortic wall and surrounding lymph nodes were sent for bacteriologic and histologic studies. After thorough debridement of the involved aorta and surrounding inflammatory tissues, an interposition graft repair was performed using a metallic silver-vaporized Dacron graft (Silver graft/B. Braun, Melsungen, Germany) 18 mm in diameter. The graft was covered with an omental patch before peritoneal closure. Pathological examination of the resected aortic tissue demonstrated necrosis with dense foci of acute inflammatory reaction. No bacteria were observed in any of the gram-stained preparations of aortic tissue. Cultures of aneurysmal sac segments were also negative, but additional analysis using a polymerase chain reaction (PCR) technique demonstrated S. suis serotype 2 as the causative organism for this mycotic aortic aneurysm. After two more weeks of parenteral antibiotics, Ciprofloxacin (0.25 g twice a day) was given orally for one month. The patient was discharged from our institution after an uncomplicated recovery. One month after surgery, clinical evaluation, CT scan, and inflammatory markers revealed no evidence of ongoing infection. The patient had a regular follow-up and has been doing well nine months after discharge.
Discussion
Bacteria commonly involved in infections of an atherosclerotic aorta include Staphylococcus aureus, S. pneumoniae, nonhemolytic streptococci, Salmonella sp., and other gram-negative bacteria, such as Escherichia coli, Campylobacter sp., Pseudomonas sp., and Bacteroides species [1,2]. Streptococcus suis is a common infection in pigs that may present as meningitis, bacteremia, and less commonly endocarditis, arthritis, or bronchopneumonia. The bacterium is carried in the tonsils of young weaned pigs and spread between pigs by nose-to-nose contact or by aerosol over short distances [3]. Occasionally it affects humans, causing meningitis, and it became recognized as an occupational zoonosis in 1968 when first reported in Denmark [4]. Streptococcus suis serotype 2 is responsible for the vast majority of human infections. The exact route of infection for humans has not been well delineated, but S. suis infection occurs mainly in adults and is often related to accidental inoculation through skin injuries. Occupational exposure to pigs and pork, inhalation of aerosols, and ingestion of contaminated pork have also been suggested [3,5]. More than 400 cases of Streptococcus suis infection have been described previously, with a geographic distribution heavily biased toward northern Europe and eastern and southeastern Asia, including China, Hong Kong, Thailand, and Taiwan [6]. Common occupations at risk include pig breeders, abattoir workers, meat processing and transport workers, butchers, and cooks. Patients infected with S. suis are usually previously healthy adults, although patients with asplenia, diabetes mellitus, alcoholism, and malignant diseases are at greater risk of such infection [7,8]. Human infections with S suis are most frequently manifested as purulent meningitis, but reports of septic shock with multiple organ failure, endocarditis, pneumonia, arthritis, and peritonitis have also been published [5].
Diagnosis is usually made upon recovery of bacteria from the cerebrospinal fluid, blood, or joint fluid (the last if septic arthritis occurs). The bacterium can be grown in culture and PCR can be used to detect specific serotypes or strains of S. suis in animal carriers, to identify strains obtained from infected or healthy pigs or in specimens from sick humans for clinical diagnosis or epidemiologic studies. A type 2-specific PCR has been developed and established for the detection of S. suis type 2 in human infection [9]. The isolated strain of S. suis from this patient was sensitive to penicillin and cefotaxime. Intravenous penicillin G is the treatment of choice and should be given as early as possible; the appropriate dose is 18–24 million units per day for 2–6 weeks (mean duration four weeks). Delay in treatment adversely affects survival.
Human infections are not frequent but are serious. Because hospital laboratories are not familiar with S. suis, human disease may be underdiagnosed. Recurrent septic shock due to S. suis serotype 2 after a 15-year interval has been reported; the second and fatal episode being considered a re-infection rather a recurrence, confirming the absence of immunity after previous infection and the importance of persisting with preventive measures [10].
Within streptococci, S. suis is probably the best example of a bacteria that causes a zoonotic infection by direct transmission to human beings. Streptococcus suis vaccines for humans do not exist currently. Suitable preventive measures, such as observation of personal and environmental hygiene and avoidance of contact with pigs that are sick. Education and supervision of people who come in contact with unprocessed pork (e.g., butchers, abattoir workers, and pig farmers) that they should use protective gloves, wash hands after handling pigs or raw pork, cover any wounds, and avoid injury while processing meat is important to decrease the transmission of S. suis to humans.
In our patient, we followed the principles of management of mycotic aneurysms, namely excision of all infected tissue, including all involved vascular tissue, with restoration of distal arterial flow. In situ placement of the Dacron prosthesis in an interposed aortic position rather than an extra-anatomic bypass was performed because of the lack of local purulence and previous culture results governing appropriate antibiotic treatment with penicillin. A silver-coated polyester graft is used to treat infection in abdominal aortic grafts and aneurysms caused by organisms with low virulence to further reduce the risk of graft infection or when autogenous deep vein reconstruction is not possible [11], but long-term follow-up will be necessary to exclude graft infection.
In conclusion, although other human infections with this organism have been reported, this is the first report of a mycotic aneurysm caused by S. suis. This report, taken together with reports of other human infections with this organism, suggest that it should be suspected as an etiological agent in any mycotic aneurysm occurring in adults with a recent history of contact with pigs or unprocessed pork, especially after an infection associated with an episode of bacteremia.
Footnotes
Acknowledgments
The authors acknowledge the assistance of Dr. Tidarat Jiraongcharoenlap in providing the laboratory data used in this report.
This study projected was supported by the research fund of the Department of Surgery, Chiang Mai University, Thailand.
Author Disclosure Statement
There are no conflicts of interest to disclose.