
Abstract
Abstract
Background:
Appendicitis is a common surgical emergency with numerous postoperative infective complications. We report an unusual case of iliac crest osteomyelitis as a late complication following emergency appendectomy for perforated gangrenous appendicitis.
Methods:
Review of the pertinent English language literature.
Results:
To the best of our knowledge, this is the first report in the English literature to describe iliac crest osteomyelitis as an infective complication of perforated gangrenous appendicitis. The diagnosis was made with the aid of magnetic resonance imaging and radioisotope bone scans. The complication was treated successfully with broad-spectrum intravenous antibiotics and physiotherapy.
Conclusion:
Iliac crest osteomyelitis is indeed a rare complication of appendicitis. A heightened awareness and better understanding of this complication would necessitate early diagnosis and treatment.
About one-fifth of the patients with appendicitis have appendiceal perforation at presentation [7–10]. Appendiceal perforation is more common at the extremes of age, when misdiagnosis and delayed intervention are usually frequent [11,12]. Maxwell and Ragland reported that the mortality and morbidity rates are significantly higher in perforated (16%) than in nonperforated (5.6%) appendicitis [13].
Post-appendectomy complications include surgical site infection (varying from <5% in simple appendicitis to 20% in perforated appendicitis), intra-abdominal abscess, and intestinal obstruction due to adhesions [14]. We report a case of iliac crest osteomyelitis as an unusual infective complication following appendicectomy. To the best of our knowledge, this is the first such reported case in the English literature.
Case Report
A 29-year-old previously healthy male presented to the emergency room of Blackpool Victoria Hospital with a two-day history of central abdominal pain that radiated to the right iliac fossa.
Clinical examination of the patient showed that he was febrile. The right iliac fossa demonstrated local peritonitis (local guarding and rebound tenderness). His routine blood test results were within the normal range except the C-reactive protein, which was 96 mg/L (normal value <10 mg/L). A working diagnosis of appendicitis was made, and he was taken to theater on the same day. After a single dose of intravenous cefuroxime 750 mg and metronidazole 500 mg administered preoperatively, a Lanz incision was made, which is a transverse muscle-splitting incision over McBurney's point. A perforated retrocecal gangrenous appendix and copious free pus were found within the abdominal cavity. Pus and intraperitoneal swabs were collected at this point and sent for microbiology analysis. A routine appendectomy was performed and the peritoneal cavity was washed out thoroughly.
The intraperitoneal culture results obtained a few days later were positive for both Pseudomonas aeruginosa and Bacteroides spp., which were sensitive to piperacillin-tazobactam and metronidazole. Postoperative, the patient developed a surgical site infection. The surgical site and blood cultures had also grown both P. aeruginosa and Bacteroides spp. The patient was subsequently treated with a seven-day course of intravenous piperacillin-tazobactam 4.5 g and metronidazole 500 mg both administered three times daily. The surgical site appeared healthy thereafter, and he was discharged on the ninth day after appendectomy.
Six weeks later, the patient was readmitted to the hospital with severe, disabling pain in the right lower quadrant of the abdomen. He was also unable to bear weight on his right side. These symptoms had gradually developed after discharge from the last admission. Physical examination revealed tenderness on the right iliac fossa and relative softness at other parts of the abdomen. Unexpectedly, he had marked tenderness on palpation of the right iliac crest and the anterior superior iliac spine (ASIS). Active movement of the right hip was limited and painful. His blood results showed an elevated C-reactive protein (68 mg/L). Plain pelvic radiography was performed, but no abnormalities were found (Fig. 1).

Plain pelvic radiograph. No pelvic bone abnormalities were found. Both left and right hips appeared normal.
In view of the patient's medical history and clinical examination findings, a computed tomography (CT) scan of the abdomen and pelvis (Fig. 2A, 2B) was requested urgently, and it showed early signs of inflammation of the anterior abdominal wall musculature with possible erosion of the right iliac crest and right ASIS. There were no other positive findings. Magnetic resonance imaging (MRI) and bone scans were then performed to investigate matters further.

Computed tomography (CT) scan of the abdominopelvic cavity. (
The MRI showed increased signal on T2-weighted imaging within the right iliac crest and surrounding soft tissue (Figs. 3 and 4). There was no collection of free fluid in the abdomen and pelvis.
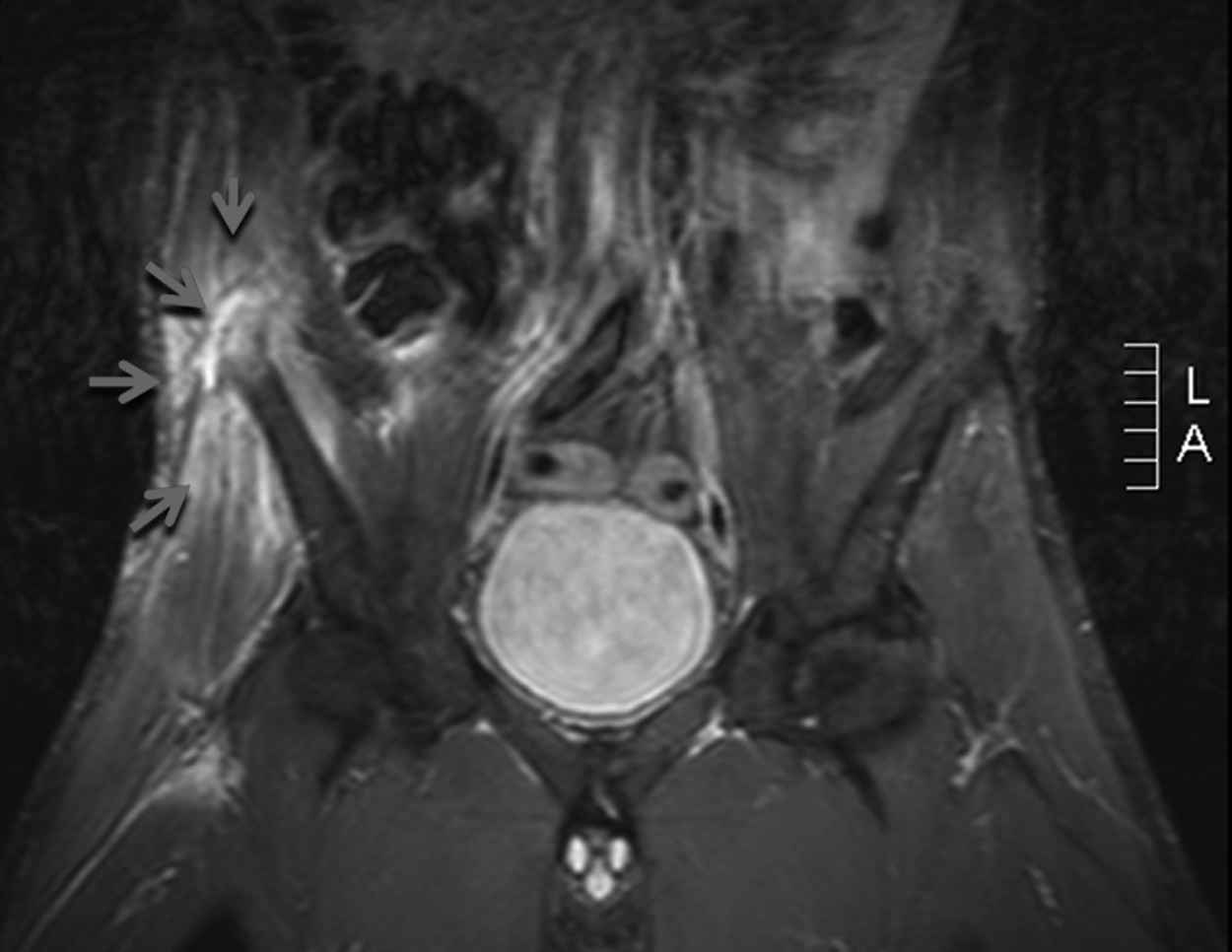
A coronal section of T2-weighted magnetic resonance (MR) scan of the pelvis. There was an area of increased signal of T2-weighted imaging (pointers) on the right iliac crest and anterior superior iliac spine compared with the left pelvis.
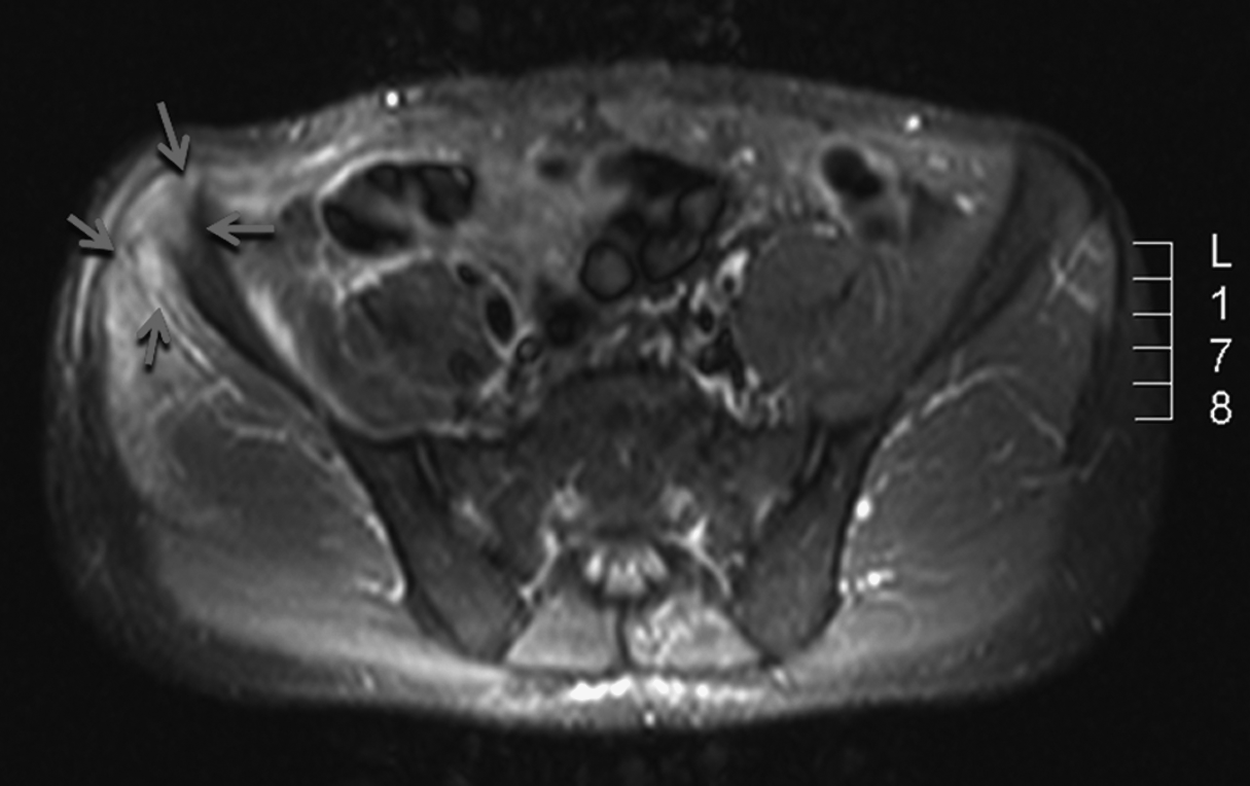
Transverse section of T2-weighted MR scan. There was increased signal on the right anterior superior iliac spine and its surrounding tissues (pointers), which increased the suspicion of an ongoing bone inflammatory process.
The technetium-99m methyl diphosphonate bone scan (Fig. 5), interpreted in conjunction with the MRI, revealed areas of increased uptake of radioisotopes in the right iliac crest and the ASIS. These radiological investigations, combined with the presence of P. aeruginosa and Bacteroides spp. in blood, surgical site, and intraperitoneal cultures during the first admission, confirmed our suspicions of iliac crest osteomyelitis as a postoperative complication of perforated appendicitis.

Anterior (left) and posterior (right) views of the technetium-99m methyl diphosphonate bone scan. The “hot” area (circled) on the right pelvic brim represents increased radioisotope uptake.
After consultation with both the orthopedics and microbiology departments, we treated the patient with a 4-week course of parenteral piperacillin-tazobactam 4.5 g three times daily and vancomycin 1 g twice daily. Following that, he was given a six-week course of enteral ciprofloxacin, doxycycline, and rifampin.
This regimen treated his condition successfully (his inflammatory markers normalized after treatment with antibiotics) and, with time and intensive physiotherapy, his mobility returned gradually to normal.
Discussion
Osteomyelitis is an inflammation of the bone, usually caused by infecting pathogens [15,16,17]. There are two major osteomyelitis classification schemes, one based on the duration of illness (acute versus chronic) and the other based on the mechanism of infection (hematogenous versus exogenous spread) [18,19,20]. The hematogenous type is predominantly seen in children more so than in adults, and it usually affects the highly vascular long bones such as those of the lower limbs in children and vertebrae in adults [21]. Exogenous osteomyelitis usually results from direct trauma, iatrogenic causes such as surgical procedures, and contiguous spread from soft tissue infections surrounding the bone [22].
Epidemiologic studies show a slight male preponderance, with a male-to-female ratio of 1.5:1 to 2:1 [23]. In addition, the annual incidence of osteomyelitis is higher among younger children than among the general adult population [24]. People of African descent who suffer from sickle cell disease are more susceptible to osteomyelitis than the general healthy population [25,26]. The incidence is also relatively high among immunocompromised and diabetic populations [27].
The causative organisms for osteomyelitis vary according to the patient's age and whether it is hematogenous or exogenous osteomyelitis. Some common microorganisms include Staphylococcus aureus (70–90% of pediatric osteomyelitis [28]), P. aeruginosa, Escherichia coli, and those of the Enterobacter species [29]. Others such as streptococci, anaerobes, fungi, and mycobacteria have also been implicated [19,30–32].
Beaupré and Carroll outlined three syndromes of iliac crest osteomyelitis: Abdominal, gluteal, and lumbar disc syndromes [49], based on the anatomic position and structure of ilium. The relatively thin cortex and the lack of medullary canal predispose to early inflammatory perforation of the cortex. If the perforation occurs in the inner cortex, abscess collects beneath the periosteum producing the abdominal syndrome of deep-seated pain in the right iliac fossa. When the perforation occurs in the outer cortex, a subgluteal abscess forms and produces gluteal syndrome with pain and limitation of hip movement. When abscess from perforation of inner cortex involves the lumbosacral plexus, a lumbar disc syndrome is produced with pain felt in the lumbar region. The presence of one or more of these three syndromes should raise the index of suspicion. Our patient exhibited the abdominal and gluteal syndromes to a certain extent.
Our patient presented with a high clinical suspicion of osteomyelitis. The MRI and bone scans showed evidence of inflammation of the iliac crest and anterior superior iliac spine, consistent with osteomyelitis. Ideally, bone biopsy should have been performed to help identify the actual causative organisms and susceptibility data [33]. However, bone biopsy is useful only if the diagnosis of osteomyelitis is uncertain [34–38]. Where radiological and clinical findings are consistent with osteomyelitis in the setting of positive blood, surgical site, and intraperitoneal swab cultures as in the present case, bone biopsy may not be necessary [39]. In addition, obtaining a bone biopsy may be impractical in some circumstances, such as when the biopsy site may heal poorly because of inadequate vascular supply to certain types of bone and hence aggravate inflammation of the bone [39].
We speculated three ways of development of osteomyelitis in our patient. These were (1) seeding of the pathogens during the operation, when pus may have tracked into the muscle layers to their attachments, that is, the ASIS; (2) direct spread through the iliacus during perforation of the appendix; or (3) blood borne spread through bactercemia (hematogenous spread). Due to the close proximity of appendix to the ipsilateral ASIS, the first two ways are more likely than blood-borne spread.
Osteomyelitis is associated with high mortality and morbidity rates, especially among children, therefore early treatment with antibiotics is of paramount importance. In the pre-antimicrobial era, osteomyelitis was usually associated with a mortality rate as high as 25–40% [16]. With the use of antibiotics, the mortality rate has now been reduced to virtually zero [16]. The choice of antibiotics should be tailored to suit cultures, preferably from bone biopsy and sensitivity findings [36,40]. The existence of Pseudomonas in the blood, surgical site, and intraperitoneal cultures in our patient was important as it is one of the common causative organisms for osteomyelitis [29]. A 4-week course of piperacillin-tazobactam 4.5 g three times daily and vancomycin 1 g twice daily was given as per recommendation by numerous studies, during which routine blood tests were obtained regularly and serum vancomycin concentrations were monitored closely.
Imaging plays an important role in the diagnosis of osteomyelitis. The most sensitive imaging modality is MRI particularly when demonstrating the extent of osteomyelitis [41,42], with 88–100% and 75–100% sensitivity and specificity, respectively [41,42]. However, osteomyelitis frequently requires more than one imaging technique for diagnosis. Nuclear medicine bone scan, despite the risks of radioactive exposure, has high sensitivity and is often used in conjunction with other imaging modalities such as MRI scan [41]. Computed tomography scan seems better at depicting any abnormality, for example, periosteal new bone formation and cortical bone destruction [41,43]. Where accessibility to the above modalities is limited, conventional plain radiography can provide reasonable diagnostic accuracy [41].
Our case report represents a rare complication associated with perforated appendicitis. There are many other rare complications described in the recent literature. These include thigh emphysema [44], retroperitoneal gangrene from a perforated retrocecal appendicitis [45], and scrotal abscess formation [45], to name a few. In the context of iliac crest osteomyelitis as a late infective complication of perforated appendicitis, our case is the first in English literature. We found another similar case reported in the German literature [47]. Within the English literature there are some cases of iliac crest osteomyelitis masquerading as appendicitis but not caused by it [48,49].
We emphasize that although iliac crest osteomyelitis is a rare complication of appendicitis, it requires prompt diagnosis and treatment. Despite all the advanced imaging techniques available, diagnosis is still established through meticulous physical examination of the patient and his medical history. To conclude, this case report aims to generate awareness and understanding of this rare complication.
Footnotes
Author Disclosure Statement
No competing financial interests exist.