
Abstract
Abstract
Background:
We investigated current clinical practice of antimicrobial prophylaxis (AMP) in surgery.
Methods:
Survey administration of AMP to patients without co-morbidity or allergy undergoing surgery, among surgeons indexed as corresponding authors for articles published in general surgery, orthopedics, gynecology, and cardiac surgery journals.
Results:
A total of 1,068 surgeons answered (response rate 68%). Of these, 26.1% do not begin infusion of the first antimicrobial dose within 1 h of incision, as suggested by guidelines, and 27.2% continue administering AMP for two or more days after surgery, including 7.6% who continue for four to seven days, in contradiction to the guidelines. There were significant differences between Europe and North America in the selection of AMP regimens. Furthermore, 19% of Europeans order infusion of the first antimicrobial dose during the incision compared with 3.9% of North Americans; 74.2% of Europeans discontinue AMP within 24 h after surgery compared with 86% of North Americans. Finally, 31% of general surgeons in North America administer supplementary oral prophylaxis for colectomy compared with only 5% of European surgeons.
Conclusions:
The AMP strategies in day-to-day self-reported practice differ significantly. Uniform, evidence-based practice is warranted, especially in this era of increasing antimicrobial resistance.
Despite the academic consensus regarding the proper application of AMP, studies around the world have shown that surgeons are reluctant to implement suggestions for short AMP regimens with properly selected antimicrobial agents in their everyday clinical practice [2,9]. We investigated current practice of AMP in surgery by performing an international survey.
Patients and Methods
Study subjects
We searched the PUBMED database and identified all articles published in journals of general surgery (American Journal of Surgery, Journal of Surgical Oncology, Archives of Surgery, British Journal of Surgery, Diseases of the Colon and Rectum, Journal of the American College of Surgeons, and Surgery), orthopedics (Clinical Orthopaedics and Related Research, Journal of Bone and Joint Surgery [American and British], Osteoarthritis Cartilage, and Spine), gynecology (Fertility and Sterility, Human Reproduction, Obstetric and Gynecogical Survey, and Obstetrics and Gynecology) and cardiac surgery (European Journal of Cardiothoracic Surgery, Journal of Cardiac Surgery, Journal of Heart and Lung Transplantation, Journal of Thoracic and Cardiovascular Surgery, and Thoracic and Cardiovascular Surgery) published from March 15 to April 15, 2008. We established communication with the corresponding authors who had an e-mail address available at the indexed affiliation and surveyed them. Respondents were informed of the aims of the study and asked to participate if they routinely performed colectomies, total hip replacements, hysterectomies, or cardiac artery bypass grafting. No follow-up notices were sent. The survey and study protocol were approved by the Ethics Committee of the Alfa Institute of Biomedical Sciences (AIBS), Athens, Greece.
Questionnaire
Participants completed a semi-structured Web-based questionnaire on the use of AMP in surgery. Specifically, after choosing their area of expertise, respondents answered a relevant set of questions regarding the administration of AMP to patients without co-morbidity or allergy who were undergoing colectomy, total hip replacement, hysterectomy, or coronary artery bypass graft surgery, as appropriate (see Appendix). We recorded the time required for the completion of the questionnaire as well as the continent of origin of the participants. No follow-up notices were sent.
It was emphasized to all respondents that we sought to record their everyday clinical practice, not to test their knowledge of relevant recommendations and guidelines. Answers were submitted electronically to ensure the anonymity of the participants.
Data analysis
To better serve the purposes of the analysis, answers regarding the antimicrobial agents were grouped into categories. The collected data were tabulated and analyzed with nonparametric tests, specifically, the chi-square criterion of homogeneity.
Results
The online questionnaire was accessed by 1,578 surgeons of whom 1,067 responded (response rate 68% among those who opened the Web page). Specifically, we received answers from 372 general surgeons, 393 orthopedic surgeons, 101 gynecologists, and 201 cardiac surgeons. Most of the participants originated from Europe or North America (531/1067 [49.8%] and 361/1067 [33.9%], respectively), whereas participants from Asia, South America, Australia, and Africa were considerably fewer (131/1067 [12.3%], 24/1067 [2.3%], 10/1067 [0.9%], and 9/1067 [0.8%], respectively). The median time required to complete the questionnaire was 67 seconds (interquartile range 45–111 seconds).
In Figure 1, we present participants' answers regarding the time of administration of AMP. Answers differed significantly among surgeons in different fields (p < 0.001): 80.8% of orthopedic surgeons administer AMP 30 minutes to 1 h prior to surgery compared with 51.5% of gynecologists; 12% of cardiac surgeons administer AMP 2–3 h prior to incision compared with 7.7% and 8.5% of orthopedic and general surgeons, respectively. A considerable proportion of respondents stated that infusion of the first antimicrobial dose is ordered during the incision: 35.6% of gynecologists, 15.8% of general surgeons, 10.5% of cardiac surgeons, and 9.2% of orthopedic surgeons. Finally, according to the answers received, 40.3%, 40.3%, and 15.7% of general surgeons who administer supplementary oral prophylaxis order the first dose 24 h or more, 12 h, and 6 h prior the incision, respectively.
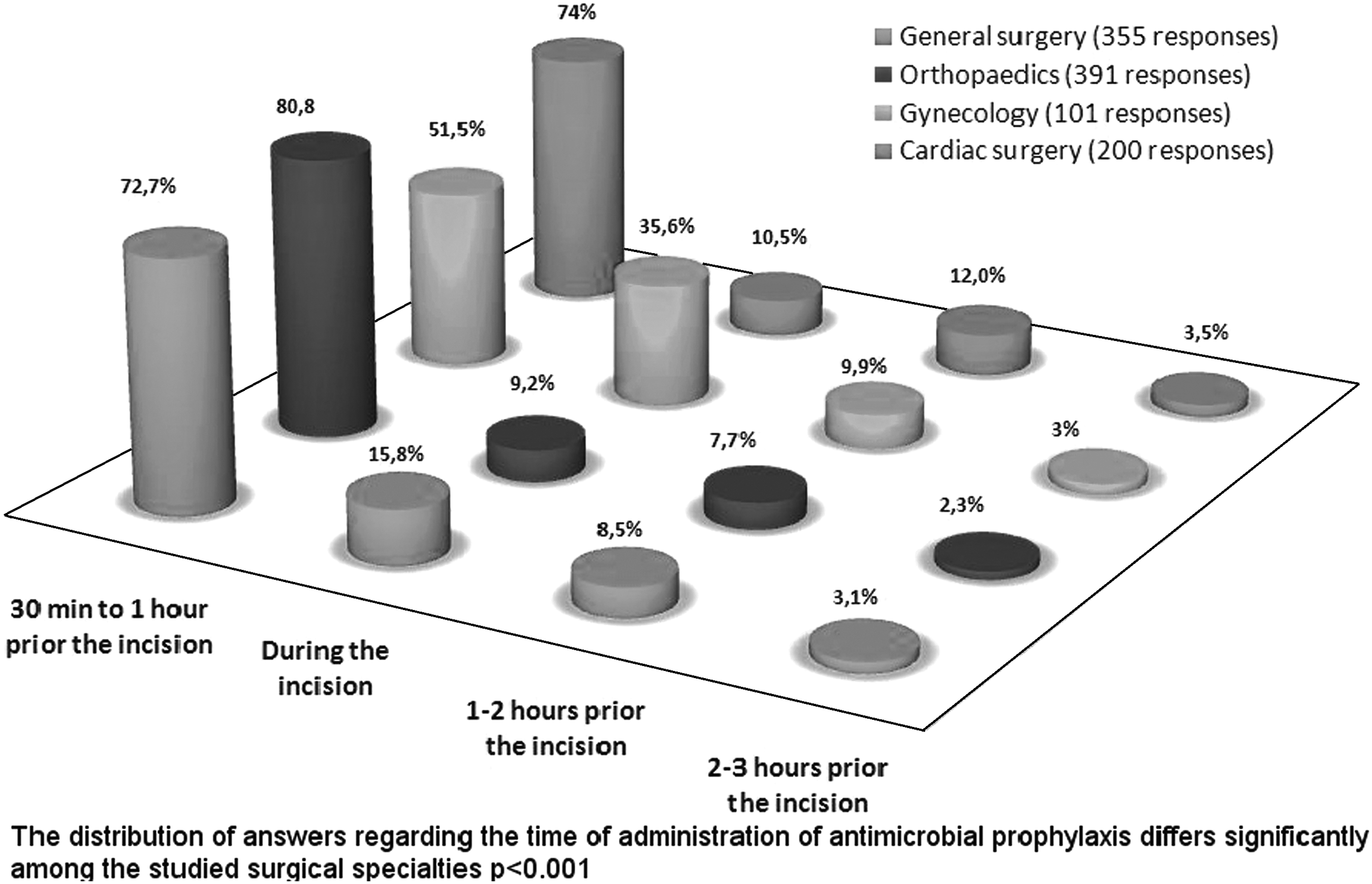
Time of administration of intravenous antibiotic prophylaxis. Distribution of times differs significantly (p < 0.001) among specialties.
The time of discontinuation of prophylactic antimicrobials was significantly different (p < 0.001) among the respondents (Fig. 2). A considerable proportion of the participants administer prophylaxis for two or more days after surgery: 51.3% of cardiac surgeons, 24% of orthopedic surgeons, 20.6% of general surgeons, and 15% of gynecologists. A smaller proportion of respondents continue the regimen for 4–7 days or even longer (Fig. 2). Finally, 88.3%, 5%, and 6.7% of general surgeons who administer supplementary oral prophylaxis discontinue the regimen within 24 h, 2–3 days, and 4–7 days, respectively.

Time of discontinuation of intravenous antibiotic prophylaxis. Distribution of times differs significantly (p < 0.001) among specialties.
In Figure 3, we present the antimicrobial agents used by the respondents grouped into seven categories. According to the answers received, first-generation cephalosporin monotherapy is the most widely used regimen among orthopedic surgeons (52%), cardiac surgeons (42%), and gynecologists (38%). The most popular regimens among the participating general surgeons are the combination of penicillins or cephalosporins with metronidazole (38%) and second-generation cephalosporin monotherapy (29%). The likelihood of use of more advanced agents such as glycopeptides and third-generation cephalosporins ranged widely among surgeons in different fields: From 10% for glycopeptides in cardiac surgery to 2% for third-generation cephalosporins in general surgery (Fig. 3). In total, 9% of the respondents use glycopeptides, third-generation cephalosporins, or both for AMP. Several other agents are used in various combinations by 6% of the respondents: Fluoroquinonolones, tetracyclines, fourth-generation cephalosporins, and clindamycin. The most popular agents for oral prophylaxis in colorectal surgery are neomycin–erythromycin (40.4%) and metronidazole (40.4%).

Distribution of antibiotic choice among specialties.
Several aspects of the clinical practice of administering AMP differed significantly between participants from Europe and North America. In Table 1, we present the most important differences. First, 19% of European surgeons stated that they usually order the infusion of the first antimicrobial dose during the incision (ranging from 11.7% in cardiac surgery to 50% in gynecology) compared with only 3.9% of North American surgeons (ranging from 0.6% in orthopedics to 9.7% in gynecology). Furthermore, 74.2% of participating surgeons from Europe usually discontinue AMP within 24 h after surgery (ranging from 56.7% in cardiac surgery to 82.7% in gynecology) compared with 86% of surgeons from North America (ranging from 63.2% in cardiac surgery to 100% in gynecology). Finally, there were significant differences in the selection of AMP regimens between participating surgeons from Europe and North America; second- and third-generation drugs are used widely only in Europe. First-generation cephalosporins are used by 50.4% of North American participants compared with only 19.4% of Europeans, and glycopeptides are used by 10.6% of North American surgeons compared with 4.3% of Europeans.
Discussion
The results of this survey suggest that in their everyday clinical practice, a considerable proportion of surgeons do not adhere to the basic principles suggested by most of the issued guidelines on AMP. First, more than one-fourth of the respondents (26.1%) do not begin infusion of the first antimicrobial dose within 1 h of the time of incision. Furthermore, 27.2% of the participating surgeons continue administering AMP for two or more days after surgery. A smaller proportion (7.6%) continues for four to seven days, a regimen that is therapeutic rather than prophylactic. It should be emphasized that the questionnaire involved scenarios of patients without co-morbidity or allergy, not unusual cases where an alternative approach to AMP may be necessary. Furthermore, the study was conducted among surgeons who have published, as corresponding authors, at least one paper in international peer-reviewed journals and, probably, have academic experience. A survey among surgeons with lower academic credentials may depict even higher rates of non-adherence to the guidelines.
Of interest, this survey showed that European and North American surgeons have significantly different approaches to the administration of AMP. It seems that North American surgeons have endorsed the advisory statements of their professional associations for shorter AMP regimens and timely infusion of the first dose of antimicrobial more effectively. Furthermore, European surgeons more often use new, advanced, and expensive wide-spectrum antimicrobial agents than do American surgeons, who generally prefer first-generation cephalosporins. This may be attributed partly to local pharmaceutical marketing policies; for example, some respondents from Europe stated that older agents such as cefazolin are no longer available in the local market. Furthermore, the observed variation may be attributable to the role of governmental regulation and pay for performance, which differs significantly in Europe and North America. No doubt, the use of advanced agents has few advantages and a major disadvantage of emerging antimicrobial resistance [3]. The use of glycopeptides is significantly higher in North America; several participants stated that they choose glycopeptides because of the high prevalence of methicillin-resistant Staphylococcus aureus (MRSA) infections in their institutions. However, there is no evidence that routine use of glycopeptides for AMP in settings with perceived high rates of MRSA infections will result in fewer SSIs than do less advanced agents [5]. Finally, our survey showed that oral prophylaxis in colorectal surgery is used mainly by North American surgeons and confirmed the fact that in North America, there is a trend favoring a combination of oral and intravenous (IV) AMP [10]. In contrast, most surgeons in Europe and Asia use IV antibiotics alone [11,12] and mechanical bowel cleansing [13]. The results of randomized control trials comparing IV AMP with oral and IV AMP in colorectal surgery remain controversial [14–16].
The distribution of North American and European respondents among different specialties was similar for general surgery and gynecology; 35% of Europeans were general surgeons compared with 33.7% of North Americans, whereas 10% of Europeans were gynecologists compared with 9% of North Americans. For the specialties of orthopedic and cardiac surgery, there was a certain degree of imbalance: 32% and 23% of Europeans were orthopedic and cardiac surgeons, respectively, compared with 47% and 11% of North Americans. However, it should be noted that the practice patterns of orthopedic and cardiac surgeons, regarding AMP agent selection (Figure 2) are similar. North American and European guidelines adhere to the same principles regarding the selection of antimicrobial agents, time of administration, and discontinuation of AMP [3–8]. The only major difference is in regard to the use of oral AMP for colon surgery. American guidelines recommend oral AMP consisting of neomycin plus erythromycin or neomycin plus metronidazole initiated 18–24 h before the operation [3]. Combination of oral and IV AMP is common practice in the United States [17]. On the other hand, the most recent European guidelines [18], issued a few months after this survey was completed, did not cover the administration of oral antibiotics for colon preparation, considering that there is relatively little evidence of the effectiveness of orally administered AMP. The above may explain the observed difference regarding the practice patterns of European and North American colon surgeons.
This survey has certain limitations. First, the participants are not representative of the average surgeon. The paucity of participants originating from less developed countries may be attributed to the selection of the survey population from among authors of articles published in English-language journals with high scientific impact. Thus, the results may not apply to all settings. Moreover, there are certain limitations inherent in the methodology of surveys, including self-sel-ection bias and concerns regarding the validity and reliability of responses that are descriptions given by the participants, which may differ from reality [19,20]. It is unclear whether the results of the study would be different if the response rate of the survey had been 100%. Finally, it should be noted that a choice of “ ≤30 min” was not among the possible answers for the question regarding the time of administration of AMP. Surgeons who administer antibiotics in the operating room just prior to incision may prefer this choice to describe their practice.
In conclusion, this survey outlines that AMP strategies in day-to-day self-reported practice differ significantly. Adherence to several aspects of guidelines for AMP in surgery has to be improved, especially in Europe, and antibiotic stewardship programs may help to achieve this goal. A uniform, evidenced-based practice is warranted in the era of increasing antimicrobial resistance.
Footnotes
Author Disclosure Statement
None of the authors has any conflict of interest. No funding was provided for this project.
Appendix. Questionnaire To Record Clinical Practice of Administering Antimicrobial Prophylaxis in Surgery
What is your area of expertise? (This question served to supply the participant with the proper set of questions according to specialty)