
Abstract
Abstract
Background:
We hypothesized that strict enforcement of ventilator-associated pneumonia (VAP) prevention (VAPP) strategies would decrease the incidence of VAP and improve patient outcomes.
Methods:
This retrospective study examined 696 consecutive ventilated patients in a Level One trauma center. Three study groups were compared: Pre-VAPP, VAPP implementation, and VAPP enforcement. Ventilator days were compared with occurrences of VAP, defined by the U.S. Centers for Disease Control and Prevention National Nosocomial Infection Surveillance criteria. Patients with and without VAP were compared to evaluate the effect of VAP on patient outcome. Fisher exact, Kruskal-Wallis, and chi-square analyses were used, and p < 0.05 was considered significant.
Results:
During the pre-VAPP protocol period, 5.2 cases of VAP occurred per 1,000 days of ventilator support. The number of cases of VAP decreased to 2.4/1,000 days (p = 0.172) and 1.2/1,000 days (p = 0.085) in the implementation and enforcement periods, respectively. However, when including all trauma patients, regardless of head Abbreviated Injury Score (AIS) score, the difference in the rate of VAP was statistically significant in the enforcement period, but not in the implementation period, compared with the pre-VAPP period (p = 0.014 and 0.062, respectively). A significant decrease was seen in the mortality rate (p = 0.024), total hospital days (p = 0.007), intensive care unit days (p = 0.002), ventilator days (p = 0.002), and hospital charges (p = 0.03) in patients without VAP compared with patients having VAP.
Conclusions:
There was a statistically significant decrease in the occurrence of VAP with strict enforcement of a VAPP protocol, regardless of head AIS score. Although the difference in patients with a head AIS score <3 was not statistically significant, it was clinically meaningful, decreasing the already-low rate of VAP by half. Strict enforcement of VAPP protocols may be cost efficient for hospitals and prevent decreased reimbursement under the Medicare pay-for-performance strategies.
Ventilator-associated pneumonia prevention (VAPP) protocols, or ventilator bundles, have been used for many years [1,10,11]. Previous data indicate the incidence of VAP has decreased with the utilization of VAPP strategies. We hypothesized that strict adherence to and enforcement by daily compliance rounds with monitoring of VAPP strategies and documentation would decrease the incidence of VAP and improve patient outcomes.
Patients and Methods
Our retrospective study examined 696 consecutive ventilated trauma patients treated in a busy Level One trauma center from 2003 through June 2008. As part of a quality improvement program, a VAPP strategy was implemented in 2004 (Table 1). This protocol required all ventilated patients to have the head of the bed elevated to 30° or higher except in the event of spinal cord injury, in which case, the bed was to be placed in a 30° reverse Trendelenburg position. A standard protocol of oral cleansing with chlorhexidine was required twice daily using a dose of 10 mL applied by the Suction Swab System (Sage Products, Inc., Cary, IL) to the buccal, pharyngeal, and gingival mucosa. The tongue was scraped and cleansed using the swabs during the oral cleansing.
Respiratory therapy personnel attempted weaning from mechanical ventilation daily. Daily spontaneous breathing trials were performed at pressure support 5 cm H2O and positive end-expiratory pressure (PEEP) 5 cm H2O. One-hour trials were used for patients on mechanical ventilation for less than 72 h with an arterial blood gas (ABG) measurement at 45 min. If a patient was on mechanical ventilation for longer than 72 h, a 2-h spontaneous trial with an ABG assay at 90 min was performed. Spontaneous trials were terminated for objective findings such as respiratory rate >30 breaths/min for longer than 5 min, oxygen saturation <92%, heart rate >140 beats/min, development of dysrhythmia, systolic blood pressure >180 mm Hg or <90 mm Hg, or a tidal volume <5 mL/kg ideal body weight or <250 mL. Subjective signs of weaning intolerance were also documented, such as increased anxiety, diaphoresis, accessory muscle use, and changed mental status. If a weaning trial was stopped, the patient was reassessed for weaning tolerance the next morning. If a weaning trial was successful, a respiratory therapist notified the physician, and extubation was discussed. Physicians made the final decision about extubation of each patient.
Exclusions from weaning from mechanical ventilation were determined by physicians and documented in the chart. Reasons for exclusion were active hemorrhage, open or damage-control abdomens, acute multiple organ dysfunction syndrome, cervical spine fracture with paralysis, increasing or high-dose sedation, and acute high-percentage total body surface burns in the resuscitative phase.
Deep vein thrombosis prophylaxis was implemented according to standard patient criteria. Sequential compression devices or low-molecular-weight heparin were used on the basis of risk stratification. Simple infection control measures by health care professionals, such as hand washing, were also included in the VAPP protocols. This VAPP strategy was driven by nurses, enforced by trauma ICU case managers, and directed by physicians.
The VAPP protocols were implemented in January 2004, and data were gathered prospectively. In January 2006, the VAPP protocols began to be enforced by a trauma ICU case manager and an infection control officer. Enforcement included daily rounds on which compliance with these protocols was documented in patient charts. During the daily infection control rounds, a decision was made regarding VAP status on the basis of National Nosocomial Infection Surveillance System (NNIS) criteria (Table 2).
These data were gathered prospectively and documented in the infection control database. Physicians were not allowed to dispute an infection control decision. However, in the event a diagnosis of VAP was indeterminate, bronchoalveolar lavage (BAL) was performed.
Inclusion criteria for this study included admission to the trauma service with a need for mechanical ventilation for >48 h with no prior diagnosis of community-acquired pneumonia (CAP) between January 2003 and June 2008. Those patients who met the inclusion criteria were divided into three study groups. The first group consisted of patients seen from January 2004 to December 2005 during the VAPP protocol implementation. The second group included patients admitted from January 2006 to June 2008, during strict VAPP protocol enforcement. The control group consisted of patients admitted from January 2003 to December 2003, before VAPP protocol implementation.
Few exclusion criteria existed for this study. Those patients with a head Abbreviated Injury Score (AIS) >3 points were excluded initially. Such patients were later re-evaluated for the status of their outcomes in relation to the status of the VAPP.
The number of ventilator days was compared with the number of VAP occurrences in each study group. The data in each study group were then compared with those of the control group, and the occurrence of VAP was assessed in relation to the data published by the U.S. Centers for Disease Control and Prevention (CDC). Outcome variables included the number of cases of VAP, hospital days, ICU days, and ventilation days in the three study groups. The mortality rate of the three groups was evaluated, in addition to hospital charges and Injury Severity Score (ISS). Data were entered in the Trauma Registry at this institution. Statistical analysis was performed with the Fisher Kruskal-Wallis two-tailed test, Satterthwaite test, and chi-square analysis using commercial software. Statistical significance was defined as p < 0.05.
Results
Among the 696 trauma patients, 15 cases of VAP were documented. In 2003, during the pre-VAPP period, 5.2 cases of VAP occurred per 1,000 days of ventilation in the 215 patients (8 cases in 1,537 days). After the VAP protocol was implemented in 2004, the number of VAP cases decreased to 2.4/1,000 days of ventilation (p = 0.172). During this implementation phase, 240 patients consumed 1,678 days of mechanical ventilation with four cases of VAP. After the VAPP protocol was strictly enforced and documented by infection control and ICU managers beginning in January 2006, the incidence of VAP decreased to 1.2 cases/1,000 days of ventilator support (p = 0.085).
After including all trauma patients receiving at least 48 h of mechanical ventilation regardless of head AIS, the total number of cases of VAP increased to 31. In the control period, 6.63 cases of VAP occurred per 1,000 days of ventilator support. After the VAPP protocol was implemented, the number of cases decreased to 3.15/1,000 days with a 27.3% increase in the study population. When comparing the control period with the implementation period, the change was clinically meaningful, but not statistically significant (p = 0.062). However, during the enforcement period, only 2.03 cases of VAP occurred per 1,000 days of ventilator support with a study population increase of 40.5%. The enforcement period showed both a clinical and a statistically significant difference from the control period (p = 0.014). The incidence of VAP decreased with enforcement regardless of increasing ISS or higher head AIS.
The total mortality rate among the three study groups was not statistically different (p = 0.24). However, those patients without VAP had a 7.49% mortality rate, whereas those with VAP had a 26.67% mortality rate (p = 0.025).
In addition to decreased mortality rates in patients without VAP, significant decreases were seen in total hospital days (p = 0.007), ICU days (p = 0.002), ventilator days (p = 0.002), and hospital charges (p = 0.03) compared with VAP patients. The ISS was not significantly different in the two groups (p = 0.107). The ISS in our study actually increased with time; the average ISS in the control group was 16.78 with a median score of 14, that in the implementation group increased to a mean of 17.42 and a median of 16, and that in the enforcement period increased further to a mean of 19.46 and a median of 18. As the ISS increased in each study group, the total hospital and ICU length of stay, ventilator days, and charges increased as well. Average hospital length of stay, ICU stay, ventilator days, charges, and ISS scores are compared among the pre-VAPP, implementation, and enforcement groups in Fig. 1.
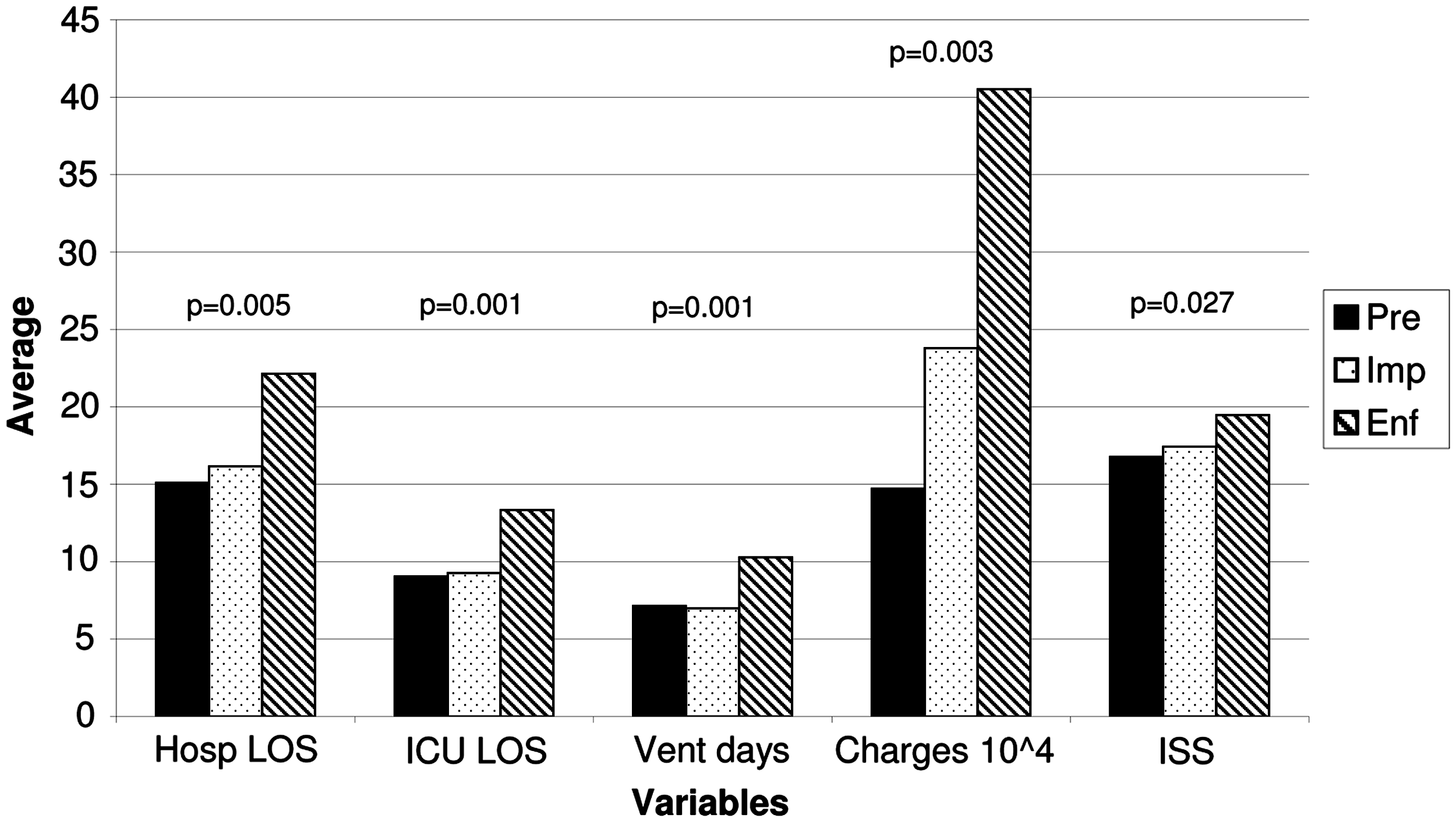
Average values during pre-VAPP, implementation, and enforcement periods. Hosp LOS = hospital length of stay; ICU LOS = intensive care unit length of stay; Vent Days = days on mechanical ventilation; Charges 10^4 = average charges (original values are obtained by multiplying by 104); ISS = Injury Severity Score; VAPP = ventilator-associated pneumonia prevention.
The causative agents of infection in this study were variable. Organisms cultured from BAL fluid included Staphylococcus aureus, Candida albicans, Enterobacter cloacae, Pseudomonas aeruginosa, Acinetobacter baumannii, Escherichia coli, and Klebsiella pneumoniae. Staphylococcus aureus was the pathogen encountered most commonly.
Discussion
Ventilator-associated pneumonia remains a major problem in the mechanically ventilated trauma population. It is the most common nosocomial infection in the ICU setting, causing patient discomfort and increasing morbidity and mortality rates and elevating charges [6,14–16,18]. A single episode of VAP may cost thousands of dollars, eventually consuming millions of health care dollars every year [15]. A trauma patient with VAP increases the average charges by approximately $175,000 compared with a patient without VAP.
Some investigators estimate 10–20% of patients on mechanical ventilation for longer than 24 to 48 h will develop VAP [7,10,17]. The median rate of VAP in the trauma population is 11.4/1,000 days of ventilation, higher than in any other ICU subgroup [16]. Ventilator-associated pneumonia has emerged as an independent risk factor for death, with an average mortality rate of 15–50% and reports of as high as 76% [7,14]. However, it is estimated that 30% of VAP cases are preventable [6].
In order for VAP to develop, pathogens must reach the lower airways by means of inhalation, aspiration, hematogenous seeding, or contiguous spread [10]. A high head AIS score is strongly associated with a greater risk of VAP, regardless of respiratory status [12,13]. Severe brain injury increases the risk of VAP secondary to aspiration of nasal and oral secretions because of blunted glottal reflexes, absence of swallowing, and lack of a cough reflex [21]. A high head AIS score may further promote VAP by the need for the supine position in cases of cervical fracture, longer hospital stays for more severe injuries, and hyperventilation in cases of cerebral edema [12]. In cranial trauma patients, VAP may increase the risk of death and the length of mechanical ventilation, ICU stay, and total hospital stay [22]. The prevalence of VAP in severe brain injury has remained steady over the last 25 years [21]. As a result, patients with head AIS >3 were initially excluded from this study because of the higher risk of VAP regardless of prevention measures. It was believed that the increased acuity and severity of brain injury in these patients would interfere with the variables of this study. All patients, regardless of head AIS, were eventually evaluated in an attempt to confirm the clinical significance of enforcement of a VAPP protocol.
Despite the implementation of the VAPP protocol in this institution in 2004, the protocol was not enforced routinely. As new nursing staff were hired for the surgical ICU, the status of implementation of the protocol was unknown. In 2006, the protocol was revised to hold nursing and physician staff accountable for its use. Completion of the protocol was documented in the chart every shift and verified by either a nurse manager or an infection control manager. After strict enforcement of this protocol was started, the incidence of VAP decreased. In fact, after the enforcement period was started, this institution had ten months with no cases of VAP in the surgical ICU.
Despite the fact that our results were not statistically significantly different from the pre-VAPP period, they do appear to be clinically meaningful, showing a halving of the already-low incidence of VAP. The rates of VAP in our institution continue to decrease with routine enforcement and widespread awareness of this protocol. These data do not appear to be cyclical, given the constant downward trend. After re-evaluating the data to include patients with any head AIS score, enforcing a VAPP protocol still appeared to have both clinically and statistically significant benefit (p = 0.01). These data support the theory that VAPP protocols may reduce the incidence of VAP, especially when staff are held accountable for protocol observance. Our results are similar to those of a study by Cocanour et al., in which staff were held accountable for completion of a ventilator bundle, resulting in a significant decrease in VAP [1].
The cost of this protocol was minimal. Previously employed staff such as infection control managers, nursing managers, and respiratory therapists enforced it, avoiding additional personnel costs. Chlorhexidene costs approximately $15.00 for a 473-mL bottle in our institution, and the average cost for one day is <$1.00 per patient. This protocol thus does not require high costs or excess personnel, merely utilization of resources readily available in most hospitals.
Over the years, the degree of injury of trauma patients has varied. During our study, ISS increased over time, although not significantly. This increase in ISS may have contributed to the greater number of ventilator days, longer hospital and ICU stays, and higher total charges. After implementation of a VAPP protocol mandating early weaning from a ventilator, many of the trauma patients with lower ISS scores may have been eliminated from the study because they were not on mechanical ventilation for >48 h. Another consideration is that some patients may have been delayed in moving toward step-down wards secondary to high hospital volume and lack of floor beds, potentially increasing the length of ICU and hospital stays and the charges. The increase in hospital charges may have been a result of more days on the ventilator, greater acuity of injury, and longer hospital stays.
According to the NNIS, the median rate of VAP was 11.4/1,000 ventilator days in a trauma ICU [16]. The NNIS criterion has 84% sensitivity and a specificity of 69% when applied to individual patients using BAL results as the criterion standard [14]. The incidence in our institution is well below the national average at 6.63 cases/1,000 days of ventilator support. Although this study failed to show a significant decrease in VAP among trauma patients with head AIS <3, we will continue to collect these data to obtain a sufficient study population.
This study indicates that although implementation of a VAPP protocol is important, strict enforcement of and accountability for this protocol may be the key factor in a successful program. Although our results were not significant in trauma patients with a head AIS <3, we believe the study is a worthwhile pursuit, especially in the era of Medicare's “pay-for-performance” programs. The Deficit Reduction Act of 2005 has created financial incentives for quality improvement programs in hospitals since 2009 [19]. Early calculations estimate 1–2% bonus payments to the top 20% of hospitals, ranging from $914 to $847,227 [19]. However, reductions in pay by as much as 2% may be expected for those hospitals with poor performance and more complications such as VAP [19]. The United States has health care costs 40% higher than the next most expensive nation, yet 44,000 to 98,000 Americans die in hospitals each year as a result of medical errors [20]. Utilization of prophylactic measures, such as a VAPP protocol, may be part of the way to lower health care costs and improve medical care [20]. We conclude that a VAPP protocol may reduce costs and improve patient outcomes, but more studies are needed to determine appropriate changes to the protocol and methods to ensure its observance.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Presented at the Twenty–ninth Annual Meeting of the Surgical Infection Society, Chicago, Illinois, May 6–9, 2009.