
Abstract

To the Editor:
Intranasal ethmoidectomy (INEC) is the common and safe procedure used in the management of sinus disease. Intracranial infections are very rare but remain one of the principal complications of INEC, including meningitis and epidural abscess [1–5]. To our knowledge, intraparenchymal brain abscess following INEC has not been described previously in the English literature.
We present here in a case of frontal brain abscess in a 29-year-old immunocompetent man who underwent INEC for sinonasal polyposis 16 days before his admission to our hospital.
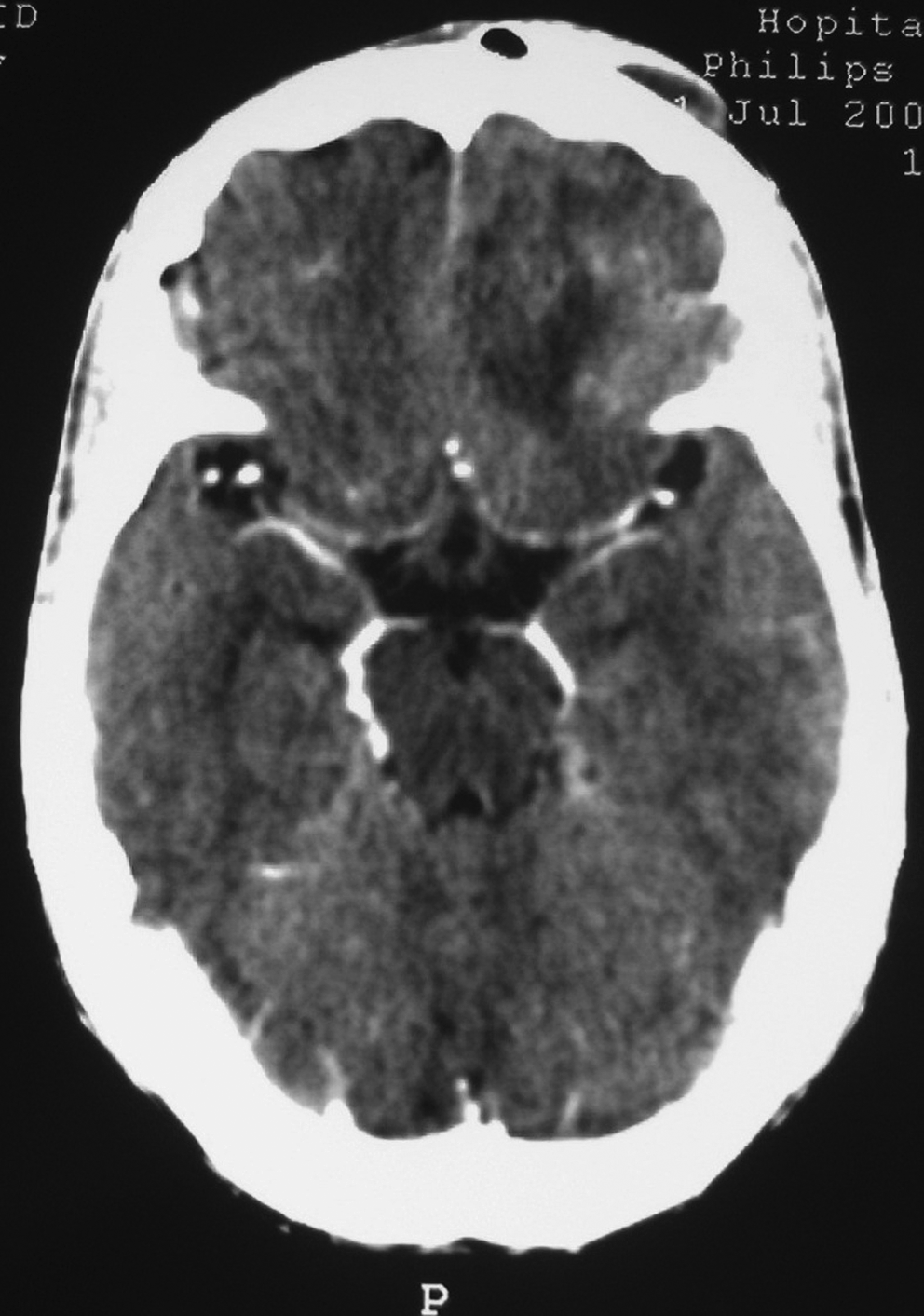
This previously healthy 29-year-old man presented with five days of fever and recent onset of frontal headache and nausea. He was operated on 16 days before this admission, in another institution for sinonasal polyposis (based on the Lund-Mackay staging system on computed tomography [CT] scan [6], the total score was 20 points representing high severity of disease) (Fig. 1). Surgical treatment consisted of an intranasal bilateral polypectomy with ethmoidectomy. This includes ethmoid sinus surgery to the bulla, anterior ethmoid sinus surgery, and posterior ethmoid sinus surgery. The patient was discharged on the fifth postoperative day without complications.

Preoperative axial (
On admission, he was alert with a low-grade fever (38.5°C) without neurologic or ophthalmologic signs. He had mild neck stiffness without rhinorrhea. Intranasal and ethmoidal examination revealed no purulent material or fistula. No other source of infection was identified. Laboratory tests revealed an erythrocyte sedimentation rate (ESR) of 10 mm/h, and leukocyte count of 10,000/mm3. Routine cerebrospinal fluid (CSF) examination demonstrated white blood cells of 360/mm3 (70% lymphocytes), and protein 80 mg/dL. Subsequent CSF culture was sterile. Intravenous antibiotic (ceftriaxone 4 g/day) was started for presumptive postoperative meningitis. Two days later, the patient remained with sepsis and persistent headache. A non-contrast CT scan examination demonstrated an inhomogeneous hypodense space-occupying lesion in the left frontal lobe without cribriform plate defect. Magnetic resonance imaging was performed for further analysis. On T2-weighted images, areas of low and high signal intensity were identified within the lesion surrounded by a hypointense thin peripheral rim (Fig. 2A). T1-weighted images showed an ill-defined and predominantly hypointense mass in the left frontal lobe, exhibiting an enhancing rim after gadolinium administration (Fig. 2B). A cerebral abscess was suspected. The neurosurgical procedure consisted of a burr hole with aspirated pus growing Staphylococcus aureus. However, no organisms were cultured from blood or swabbed contents of intranasal space. Parenteral antibiotic treatment was changed with a combination of metronidazole (1 g/day), gentamycin (160 mg/day), and ciprofloxacin (600 mg/day).
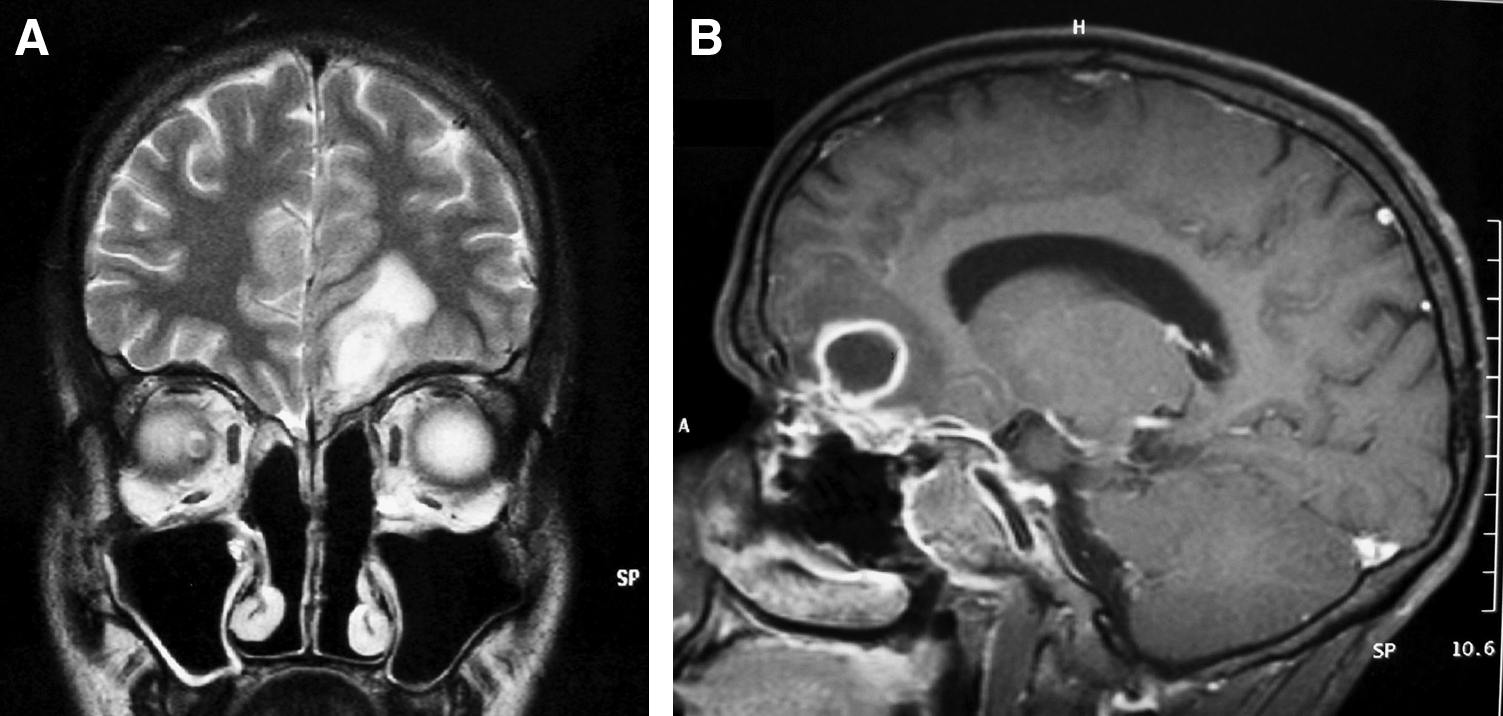
Craniofacial magnetic resonance imaging. (
The patient was discharged after three weeks of antibiotic regimen (except gentamycine for only eight days) with full clinical recovery. The brain abscess had resolved completely on cranial CT scan with and without contrast injection (Fig. 3). His antibiotic regimen was continued orally at home for three more weeks (metronidazole 1.5 g/day and ciprofloxacin 1.5 g/day).
Postoperative cranial CT scan with contrast injection showing complete resolution of the left frontal brain abscess.
Complications of INEC are uncommon and can be classified as minor or major, depending on the case. The incidence of major complications is less than 5% and includes CSF leak, pneumocephalus, internal carotid artery injury, meningitis, bleeding, orbital penetration, and death [1,2,4,5]. Among intracranial infections, suppuration (extradural or subdural empyema and brain abscess) occurs exceptionally. In the English literature, we can find only a few cases of subdural or epidural abscesses following an INEC procedure [3–5,7,8].
Nevertheless, brain abscess remains a diagnostic challenge. Fever is observed in fewer than 50% of patients. Focal neurologic findings present in only one-third to one-half of cases, especially in the frontal location [9,10]. As seen in our case, laboratory tests are of limited value for the diagnosis. Lumbar puncture provides little diagnostic assistance and is potentially dangerous in a patient with intracranial mass lesions.
There are several mechanisms that may explain why infection may spread to the brain: Direct extension of infection may occur with a dural tear or brain penetration even without rhinorrhea. This condition is observed in cases of fracture, or as a result of operative trauma. The mechanism of spread is through the bony wall of a diseased sinus, through a congenital dehiscence, although intracranial complications may occur as a result of thrombophlebitis involving the meningeal veins, cortical veins, diploic veins, or the intracranial venous sinuses and their communications. Furthermore, infection may reach the meninges and the brain via the pial sheaths of the optic nerve or the olfactory perineural sheaths [9,11].
As reported by Maniglia, postoperative CSF leak may go unrecognized initially until the patient develops one or more episodes of meningitis [1]. Special care must be exercised when dissecting between the nasal septum and middle turbinate because of the danger of injury to the cribriform plate and intracranial invasion. Antibiotics used for prophylaxis should have high penetration of the central nervous system and adequate spectrum to cover both anaerobic and aerobic bacteria [9,10]. Prompt and aggressive medical and neurosurgical intervention is required, aiming to minimize the morbidity and mortality and also to maximize a favorable outcome.
Although INEC is performed commonly with a very low incidence of complications, intracranial suppuration should be considered postoperatively in patients with fever, meningitimus, seizures, and symptoms of raised intracranial pressure even in absence of rhinorrhea or focal neurological deficits. Imaging evaluation using CT scan or magnetic resonance imaging is important to diagnose such rare complications. Effective therapy, ensured by close coordination of care between otorhinolaryngologist, neurosurgeon, and infectious diseases specialists, must be instituted promptly.
Footnotes
Author Disclosure Statement
No competing financial interests exist.