
Abstract
Abstract
Background:
Early, empiric, broad-spectrum antibiotics followed by de-escalation to pathogen-specific therapy is the standard of care for ventilator-associated pneumonia (VAP). In our surgical intensive care unit (SICU), imipenem-cilastatin (I-C) in combination with tobramycin (TOB) or levofloxacin (LEV) has been used until quantitative bronchoalveolar lavage results are finalized, at which time de-escalation occurs to pathogen-specific agents. With this practice, however, alterations in antimicrobial resistance remain a concern. Our hypothesis was that this strict regimen does not alter antimicrobial susceptibility of common gram-negative VAP pathogens in our SICU.
Methods:
After Institutional Review Board approval, a retrospective review of SICU-specific antibiograms was performed for the sensitivities of common gram-negative VAP pathogens. Time periods were defined as early (January–June 2005) and late (July–December 2006). Chart review of empiric and de-escalation antibiotic usage was obtained. Data were collated, and statistical significance was assessed with the chi-square test using the on-line Simple Interactive Statistical Analysis tool.
Results:
Imipenem-cilastatin was used 198 times for empiric VAP coverage (811 patient-days), whereas TOB and LEV were given a total of 149 (564 patient-days) and 61 (320 patient-days) times, respectively. Collectively, the susceptibility of gram-negative organisms to I-C did not change (early 91.4%; late 97%; p = 0.33). Individually, non-significant trends to greater sensitivity to I-C were noted for both Pseudomonas aeruginosa (early 85.7%; late 90.9%; p = 0.73) and Acinetobacter baumannii (early 80%; late 100%; p = 0.13). Further, both TOB (early 77.1%; late 70.0%; p = 0.49) and LEV (early 74.3%; late 70.0%; p = 0.67) were found to maintain their susceptibility profiles. The frequency of resistant gram-positive VAPs was unchanged during the study period. Our de-escalation compliance (by 96 h) was 78% for I-C, 77.2% for TOB, and 59% for LEV. When infections requiring I-C were removed from the analysis, de-escalation compliance was improved to 92%.
Conclusions:
In our SICU, early, empiric broad-spectrum VAP therapy followed by de-escalation to pathogen-specific agents did not alter antimicrobial resistance and is a valid practice. Further, our compliance with de-escalation practices was higher than published rates.
Because of the significance of this problem, the American Thoracic Society (ATS) and the Infectious Diseases Society of America (IDSA) put forth VAP management guidelines [3]. In short, these evidence-based guidelines recommend early, empiric, broad-spectrum antibiotic therapy based on the local VAP bacteriology with de-escalation to pathogen-specific therapy once culture results are final. However, the early, liberal use of broad-spectrum antimicrobials with this treatment approach has led to concerns regarding the induction or worsening of local antimicrobial resistance. Such potential deleterious effects of broad-spectrum antibiotic usage would ultimately have to be weighed against the known benefits of early empiric therapy [6,7].
Although no national VAP empiric antibiotic regimen has been recommended, it has been the practice of our adult SICU since 2004 to use imipenem-cilastatin (I-C) in combination with tobramycin (TOB) or levofloxacin (LEV) until quantitative bronchoalveolar lavage (BAL) results are final. Empiric coverage for resistant gram-positive organisms is added if indicated clinically at the initiation of therapy. Specimens are obtained by bronchoscopy with BAL prior to the commencement of antibiotic therapy. Our empiric regimen was based on the 2004 SICU antibiogram data (Table 1) reflecting the sensitivity profile for the gram-negative VAP pathogens encountered most commonly (Pseudomonas aeruginosa, Acinetobacter baumannii, Klebsiella pneumoniae, and Enterobacter spp.). This management strategy adheres to the ATS/IDSA consensus conference recommendations [3]. We hypothesized that our use of early empiric broad-spectrum antibiotic therapy for VAP with appropriate de-escalation to pathogen-specific agents would not induce gram-negative bacterial resistance in our SICU. Our goals were to ensure that our empiric and de-escalation antibiotic usage was in accordance with the consensus conference guidelines by assessing compliance with subsequent de-escalation practices and to examine what, if any, changes in the sensitivity profiles of commonly encountered gram-negative pathogens occurred during the two-year study.
Patients and Methods
The study was approved by the Maricopa Integrated Health System Institutional Review Board. The 13-bed SICU at Maricopa Medical Center, a Level I adult and pediatric trauma center and tertiary-referral teaching hospital, operates under a semi-open model. Rounds are performed daily by both the primary surgical service and a dedicated SICU group. The SICU team consists of a board-certified surgical intensivist, two or three junior residents, a physician assistant, and an ICU clinical pharmacist. Daily critical care decisions and management are conducted by the SICU team, whereas issues pertaining to surgical intervention are dealt with in conjunction with the primary service. Specific care plans pertaining to infection detection and management are made by the SICU team.
Routine monitoring for VAP is performed continuously. When VAP is suspected clinically (three of five possible signs: Fever [>38.4°C], leukocytosis [>10,000 cells/microliter], a new infiltrate on the chest radiograph, greater sputum production, increasing ventilatory requirements), quantitative BAL specimens are obtained by bronchoscopy prior to commencement of antibiotic therapy. Using bronchoscopy with BAL to obtain specimens leads to more appropriate antibiotic use, shorter ICU stays, and lower rates of death [9]. Other specimen collection techniques, such as induced-sputum samples, are not employed routinely by our SICU and are not included in this analysis.
The diagnostic bronchoscopy with BAL is in most cases performed by a surgical resident with attending staff supervision. Specimens are obtained in hemodynamically stable patients after pre-medication and oxygenation in a volume control ventilator mode (using lower volumes with a higher compensatory respiratory rate). The bronchoscope is passed no further than the tertiary bronchi. A flush of 20 mL of physiologic saline is delivered and suctioned to reduce contamination from the upper airway of the area most likely to harbor VAP pathogens. To obtain the specimen, three sequential 20-mL lavage specimens are collected through the bronchoscope into an in-line chamber. Sequential BAL specimens are obtained if clinically indicated (i.e., bilateral pulmonary infiltrates, continuing sepsis). Collections of separate BAL specimens from a single patient were considered individual events. The results of all BALs performed in our SICU during the study period were included in our analysis.
Once the specimens are received by the microbiology laboratory, a gram stain is performed although the findings do not influence our empiric antibiotic selections [10]. The specimen is then streaked with a quantitative loop to isolate colonies and perform the colony count. For specimens initially too thick to streak, a vortex is used. The colony count is performed after an incubation period of 24 h and again at 48 h if negative at the first reading. The count is considered negative and antibiotic therapy discontinued if <104 colony-forming units (CFU)/mL are obtained or if a mixture of organisms is encountered without a dominant growth after 48 h of incubation [11]. If the quantitative analysis is positive, appropriate sensitivity profiles are determined, which takes approximately 18–24 h. Routine sensitivity analysis is not performed for organisms with known usual susceptibilities such as Stenotrophomonas maltophilia. At our institution, cultures should be finalized within 72–96 h of receipt of the specimen by the laboratory. In patients already receiving antibiotic therapy for another indication, we used a diagnostic threshold of 103 CFU/mL.
The empiric VAP antibiotic regimen was chosen on the basis of our late-2004 SICU antibiograms (Table 1). The treatment consisted of I-C with TOB or LEV in patients with renal insufficiency or if there was concern about the development of acute kidney injury. The addition of coverage for methicillin-resistant Staphylococcus aureus (MRSA) was instituted if there had been prior treatment for a gram-negative infection or if resistant health care-associated pathogens were suspected. Examples are patients with a history of MRSA infection; recent hospitalization or dialysis clinic visits, antibiotic therapy, or wound care; or admission from an institutional setting such as a prison, nursing home, or long-term care facility [2,12,13]. De-escalation of antibiotic therapy to a pathogen-specific agent occurred as soon as culture results with susceptibilities were finalized.
There were no changes to infection control or other adjunctive patient care standards during the study period. Intubated patients were kept with the head of the bed elevated 30-45° when no contraindications existed, and stress ulcer prophylaxis consisted of either H2 receptor antagonists or proton pump inhibitors. The nursing staff performed mouth care every two hours with sponge sticks using a 1.5% hydrogen peroxide solution. High-low cuffed endotracheal tubes were used to permit suctioning of proximal aerodigestive tract secretions from above the endotracheal tube cuff. Although we did not have clear data on compliance with these “ventilator bundle” components, such data would be more important in identifying the change in frequency of VAP over time and should have little influence on the antibiotic resistance patterns of bacterial pathogens. Although there has not been a formal policy to limit blood product transfusions, there has been a general trend to restricting transfusion to those patients who are symptomatic or have other clear indications for transfusion.
To create the antibiogram, our hospital uses the laboratory information system (Cerner Classic, Cerner Corp.) to interface with the organism identification and antimicrobial susceptibility testing system (Vitek Legacy, bioMerieux, Inc). This arrangement provides a list of the most commonly encountered organisms with their susceptibilities for a set time span. This process is performed and evaluated annually. Urine and blood specimens were excluded from our analysis, leaving only the pulmonary isolates. The library information system treats duplicate cultures from a single patient source as a single occurrence unless 30 days have lapsed between cultures. Prospective antibiograms from the SICU for the study period January 2005–December 2006 were reviewed. Specific organism encounters were tracked, and the sensitivities of individual organisms for the early and late time periods were assessed. Our time periods were defined as early (January–June 2005) and late (July–December 2006). A retrospective chart review was then conducted to assess our use of empiric and de-escalation therapy and compliance with de-escalation by 96 h. Data were collated and statistical significance was assessed with the chi-square statistic using the on-line tool Simple Interactive Statistical Analysis (SISA, www.quantitativeskills.com/sisa/distributions/binomial.htm).
Results
The total number of BALs performed during the study period was 224 in 170 patients. This discrepancy is attributable to the fact that some patients had sequential BALs because of perceived treatment failure (i.e., continuing sepsis or pulmonary failure) necessitating assessment for resistant pathogens. The culture results were positive (>104 CFU/mL) in 63% of the specimens. Among the gram-negative pathogens, the four encountered most commonly were A. (n = 28), P. (n = 26), Enterobacter spp. (n = 25), and K. (n = 16) (Fig. 1). Other gram-negative organisms identified were Haemophilus influenzae (n = 10), Serratia marcescens (n = 8), and Proteus mirabilis (n = 5). There were a few encounters with gram-negative organisms such as Moraxella catarrhalis (n = 3) and, rarely, Stenotrophomonas maltophilia (n = 1).
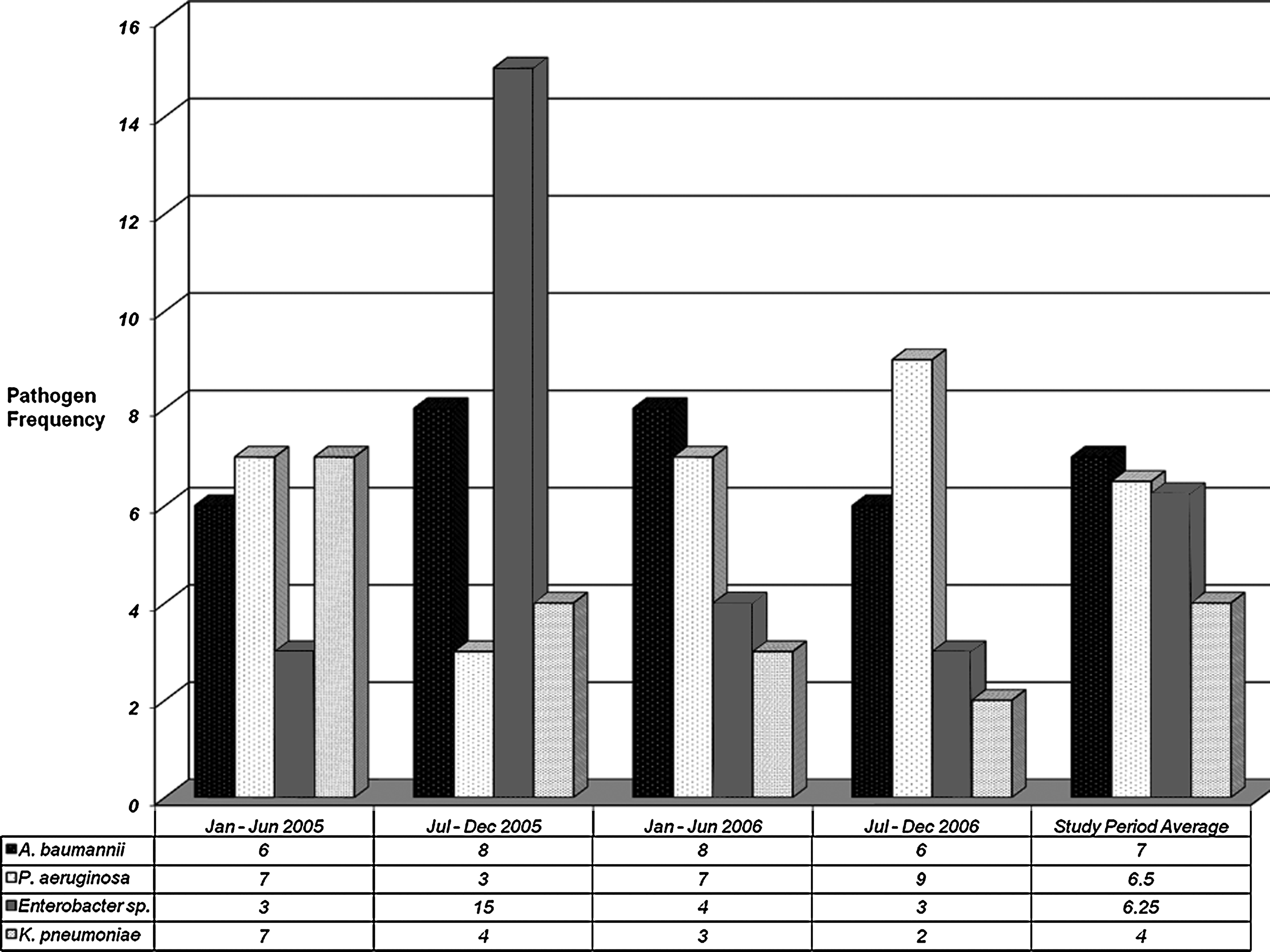
Gram-negative ventilator-associated pneumonia pathogen frequency over the study period.
Gram-positive organisms were encountered in approximately 34% of the positive BAL specimens. The most common was MRSA (n = 19). The frequency of MRSA pneumonia was highest (n = 9) in the first period (Jan–Jun 2005), with one, four, and five cases the following three periods, respectively. The next most common gram-positive pathogens were Streptococcus pneumoniae (n = 16) and methicillin-sensitive S. aureus (MSSA) (n = 7). Their frequency remained largely unchanged throughout the study period (S. pneumoniae: Five, one, five, and five cases per study period, respectively; MSSA: Two, three, zero, and two cases, respectively).
The number of occasions on which empiric antibiotic therapy was initiated for suspected VAP with each antibiotic was I-C: 198; TOB: 149; and LEV: 61. This discrepancy from the number of BAL specimens (n = 224) is secondary to the fact that a sequential BAL specimen may have been obtained because of concern about inadequate antimicrobial therapy while the patient was already being treated with empiric I-C. The total length of antibiotic exposure during the study period was I-C: 811 days; TOB: 564 days; and LEV: 320 days. Our compliance with de-escalation of empiric therapy by 96 h was I-C: 78.0% (range 1–20 days); TOB: 77.2% (range 1–15 days); and LEV: 59.0% (range 1–15 days) (Fig. 2). When we accounted for the cases in which I-C was the only acceptable therapeutic agent because of inherent antimicrobial resistance, de-escalation compliance for I-C was improved to 92%.
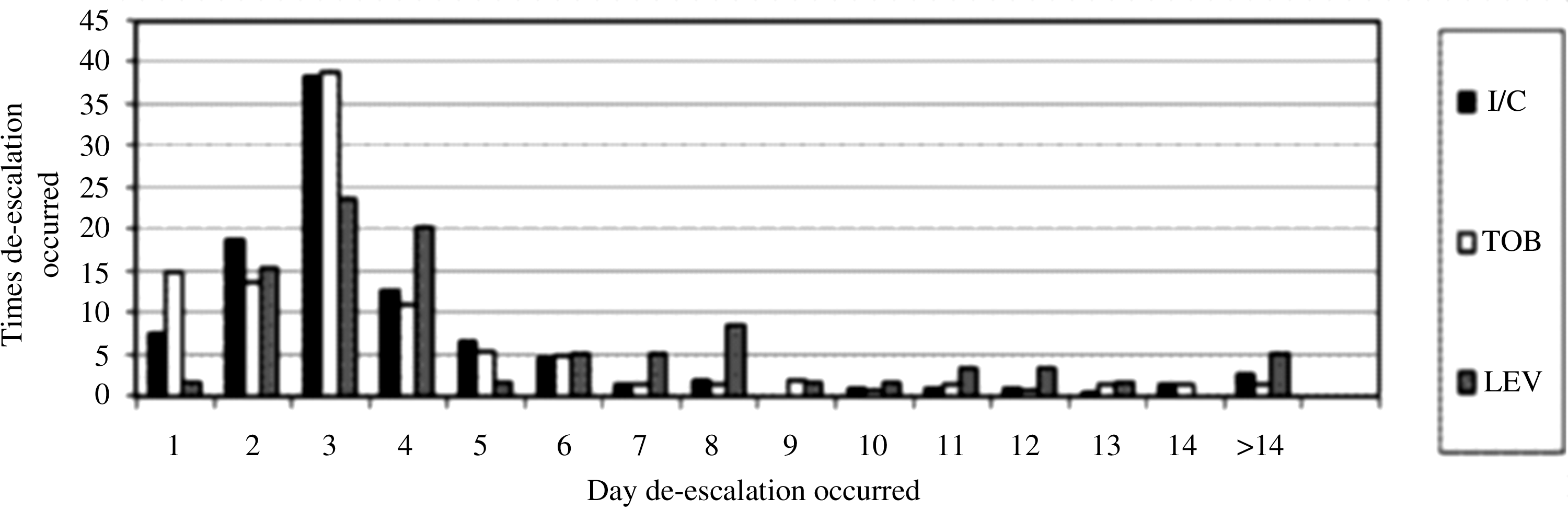
Daily frequency of antibiotic de-escalation to pathogen-specific therapy. I-C = imipenem-cilastatin; TOB = tobramycin; LEV = levofloxacin.
Collectively, the susceptibility of gram-negative organisms to I-C did not change (early 91.4% vs. late 97%; p = 0.33) (Table 2). Individually, non-significant trends in improved sensitivity to I-C were noted for both P. (early 85.7% vs. late 90.9%; p = 0.73) and A. (early 80% vs. late 100%; p = 0.13) (Table 3). Conversely, both TOB (early 77.1% vs. late 70.0%; p = 0.49) and LEV (early 74.3% vs. late 70.0%; p = 0.67) had non-significant reductions in susceptibility during the course of study (Table 2).
Discussion
With emerging and worsening antimicrobial resistance being noted worldwide, effective strategies of antibiotic stewardship must be implemented and championed by physicians and non-physician clinical providers. Obviously, a major concern regarding the use of early empiric, broad-spectrum antibiotics with subsequent de-escalation to pathogen-specific agents is for this approach to alter the sensitivity profiles of commonly encountered bacteria. In actuality, appropriately dosed, early aggressive empiric therapy and timely de-escalation contribute to the preservation of antimicrobial sensitivities [14]. Further, the use of evidence-based clinical guidelines significantly reduces the duration of antibiotic therapy and suggests a trend toward a reduction in ICU stay [15]. Less antibiotic usage and shorter ICU stays may some day yield a slowing or possible reversal of the direction of antimicrobial resistance.
We hypothesized that our use of this treatment philosophy would not induce gram-negative pathogen resistance in our patients with VAP. Indeed, our results did not show any significant induction of antimicrobial resistance, as evidenced by changes in unit-specific antibiogram sensitivity profiles over the two-year study period. It instead displayed non-significant trends toward better sensitivity profiles for our most widely used antibiotic (I-C). Further, non-significant improvement in the sensitivity to I-C for two of the most common VAP pathogens, P. aeruginosa and A. baumannii, was suggested. These findings contradict previously reported trends to increased resistance of this organism in respiratory isolates of ICUs in teaching hospitals, as reported by the National Nosocomial Infections Surveillance System group [16].
A trend to greater sensitivity of P. aeruginosa and A. baumannii to I-C with TOB followed by de-escalation also was noted by Le Floch et al. [17] in a burn ICU. These authors likewise did not find an increase in resistance, most specifically to imipenem-resistant gram-negative strains or MRSA. Furthermore, early empiric I-C and gentamicin for 72 h while awaiting culture results for sepsis followed by de-escalation was described by Namias et al. [18]. Their work likewise did not show a significant difference in the resistance profiles of the bacteria of interest. In subset analysis, those investigators demonstrated a significant increase in the sensitivity of P. aeruginosa to I-C. Our study supports these authors' findings in our predominantly trauma patient population.
On the basis of the sensitivity profiles in the antibiograms for our local pathogens, we chose to use I-C as our primary antimicrobial agent. Including a carbepenem in the empiric antibiotic regimen may play a vital role in this strategy. A recent assessment of the impact of early empiric guideline implementation using an I-C-based regimen compared with a widely varied practice (most commonly using cephalosporins and penicillins) for severe hospital-acquired pneumonia in the ICU demonstrated a significant improvement in the adequacy of initial therapy and a reduced 14-day mortality rate without increasing the number of imipenem-resistant organisms [19]. The addition of either an aminoglycoside or a fluoroquinolone as a second agent with a different mechanism broadens the coverage and may provide a synergistic effect. The principle of short antibiotic exposure time in the design of the management guidelines requires de-escalation to pathogen-specific therapy as soon as cultures are final [3]. Meticulous attention to detail with in-depth reviews of pending cultures is paramount in this strategy in order to allow discontinuation or de-escalation of the empiric therapy as soon as possible. Decreasing the number of unnecessary antibiotic exposure days should diminish the risk of resistance induction accordingly. In our study, culture results were positive in 63% of BAL specimens. This allowed immediate discontinuation of any antibiotic therapy for patients (37%) who failed to reach our diagnostic criterion threshold. Thus, unnecessary prolongation of antimicrobial exposure was avoided in 37% of patients we suspected clinically to have VAP and who would have likely received a full course of antibiotic therapy had a negative quantitative analysis not been obtained.
Our compliance rates for de-escalation of empiric therapy by 96 h to I-C, TOB, and LEV were 78.0%, 77.2%, and 59.0%, respectively. This is higher than previously reported [15,20,21]. The de-escalation compliance from I-C to a more appropriate agent was elevated to 92% when the cases in which bacteria required I-C as the subsequent therapeutic agent (secondary to resistant sensitivity profiles) were isolated. De-escalation in patients with VAP has been demonstrated to carry an associated reduction in mortality rate compared with patients requiring escalation of therapy and patients who had no change in the initial antibiotic regimen prescribed [20]. The lower de-escalation rate noted with LEV was likely attributable to the appropriate or sensitivity-specific use of this single agent to complete the course of VAP therapy.
There were some cases in which de-escalation occurred at one or two days. Finalized culture results usually are not available within this time, so the reason for de-escalation at this extremely early time usually was related to final culture results becoming available from a previously obtained BAL specimen. In a few patients, early discontinuation of TOB was secondary to recognition of evolving renal insufficiency or a higher risk of acute kidney injury. In such patients, conversion to LEV was performed as part of a renal-protective strategy.
There are some limitations to this study. First, as a registry-driven project, there may be some bias in patient selection and data collection practices. Second, although major changes in SICU standard of care were not apparent, there may be some effect on the data on changes in clinical practice over time. As stated previously, there was no formal restrictive transfusion policy implemented during the study period, but there probably was a general tendency to limit transfusions to patients who had symptomatic anemia or other firm indications for transfusion. The impact of this effort on ventilator-associated complications has been shown and may be difficult to control fully [22].
Conclusion
The time-honored belief that the use of early broad-spectrum antibiotics ensures emergence of bacterial resistance has been challenged. Although resistant organisms remain a true threat with indiscriminate use, responsible antibiotic stewardship practices may not induce antimicrobial resistance. Our results showed that a standard practice of early empiric, broad-spectrum antibiotic therapy for VAP utilizing I-C plus TOB or LEV followed by de-escalation to a pathogen-specific agent did not increase the resistance of common gram-negative VAP pathogens in our SICU. We also demonstrated that a strong antibiotic stewardship philosophy provides high rates of compliance with the empiric regimen. Our findings provide reason to believe that the concept of early empiric broad-spectrum therapy with appropriate de-escalation is an appropriate strategy in the therapy of VAP without an associated induction of anti-microbial resistance. Further studies are necessary to see if this holds true over time and if a reversal of the resistance trajectory is possible with strong antibiotic stewardship practices.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist. This research was supported by departmental funds.
Presented at the Society of Critical Care Medicine 37th Critical Care Congress, Honolulu, Hawaii, February 2–6, 2008.