
Abstract
Abstract
Background:
In the mid-20th century, it was recognized that patients with major burn injury required a dedicated, multidisciplinary team approach to receive optimal care. In the subsequent years, regionalized systems of care were developed to provide this level of care to the entire populations. There have been no reports on how an individual regional system evolved and the impact it had on the delivery of care for burn-injured patients.
Methods:
The number, distribution of patients, and mortality rates of patients who sustained burn injury from the years 1985–2006 were assessed using administrative hospital data obtained from the New York State Department of Health. Data were also obtained from the archives and registry of the first dedicated burn care facility in the region, the Shires Burn Service, from 1976 through 2008. The incidence of fires occurring by year during this period was assessed from data obtained from the Fire Department of New York City.
Results:
During the period from 1985 through 2006, there were 26,606,463 discharges from hospitals in New York City. Of these, 57,547 patients had a primary diagnosis of burn injury and 33,058 were cared for in designated burn care facilities. Since the inception of regionalized care there appears to be a 43% decrease in hospital admissions for burn injury. In the last year of study, 77.3% of the burn-injured patients were cared for in burn centers. The mortality rate has decreased from 3.8% in 1985 to 2% in 2006. In 1975 there were 137,237 fires in the region, which decreased to 44,054 in 2008.
Conclusions:
Although there has been a significant decrease in the number of patients requiring hospitalization for burn injuries, there are still a large number of patients who suffer these injuries. Regionalization of burn care has been associated with care for patients in designated facilities in over 75% of the cases and a reduction in mortality by almost 50%.
As recently as 1975 it was reported that there was a lack of resources in New York City to care for burn-injured patients. In a New York Times report, it was noted that patients were often flown to San Antonio or Boston for care [3]. In that report the largest burn treatment program in New York City was described as caring for 15 patients, who were scattered in various wards throughout the hospital. Two other hospitals were noted to have even smaller programs. The need for specialized burn care was highlighted in a report by New York City Fire Commissioner in the same year that “about 10,000 people suffered severe burns here each year” [4]. To address this need, the first center dedicated to care for the burn-injured patients was opened in this region in 1976. The goal of this program was not only to provide clinical care but also to serve as a foundation for regionalized care, education, and research related to injured patients. This report documents the evolution of a regionalized system of care for burn-injured patients in a large metropolitan region over a 30-year period.
Methods
Data sources
Administrative hospital discharge data of the Statewide Planning and Research Cooperative System (SPARCS) were obtained from the New York State Department of Health for the years 1985–2006 inclusive. As described previously [5], selected variables were extracted from each text file with the use of SAS 9.0 (SAS Institute, Cary, NC). The dataset contained 59,920,257 discharges statewide and 26,606,463 discharges from New York City. All records in which at least one of the diagnosis codes indicated a cutaneous burn or inhalation injury were extracted into a separate SAS dataset for further analysis. A table of codes to define the population has been published [5]. Data on patients admitted to the Shires Burn Service of the William Randolph Hearst Burn Center at the NewYork-Presbyterian Hospital Weill Cornell Medical Center were collected on a prospective basis. For the years 1976 to 1995 the information was found in center archives and from 1995 through 2008 in the local registry developed for the National Trauma Registry of the American College of Surgeons (NTRACS).
Results
The data available through SPARCS show that the number of burn-injured patients discharged from hospitals in the New York City peaked in the late 1980s and gradually decreased to 2,200 in 2006. Over that same period, regional burn care evolved to reach a point that more patients were discharged from burn center hospitals than noncenter institutions (Fig. 1). In 1985, one-third of the burn-injured patients were cared for in burn centers, whereas in 2006 this rate had more than doubled to 77.3%. The mortality rate for admitted burn-injured patients progressively decreased over time with rates of 3.8% and 4.15% in 1985 and 1995, respectively, to 2% in 2006 (Fig. 2).
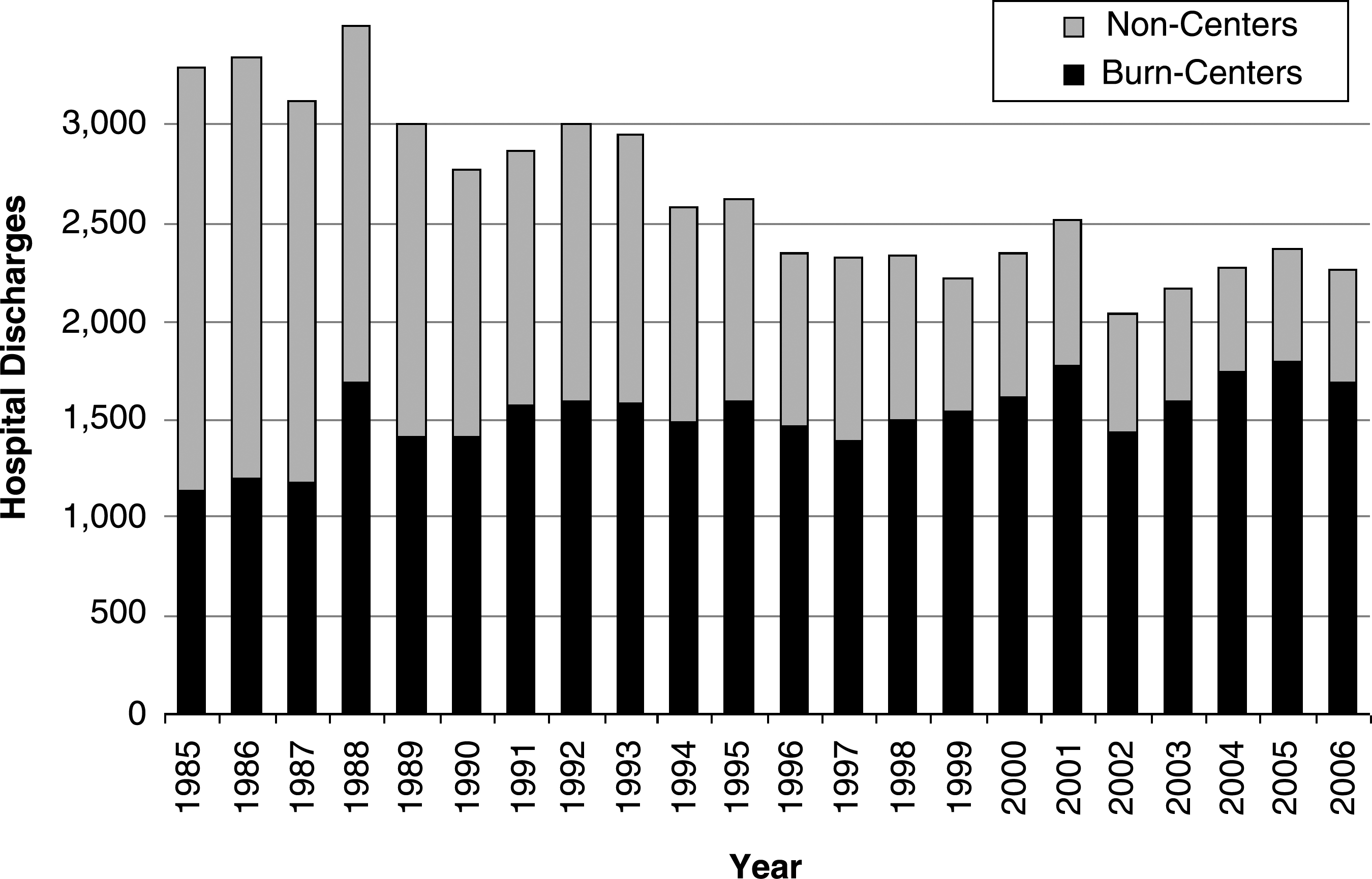
Burn-injured patient discharges from institutions in New York City are shown by year and by the type of center.
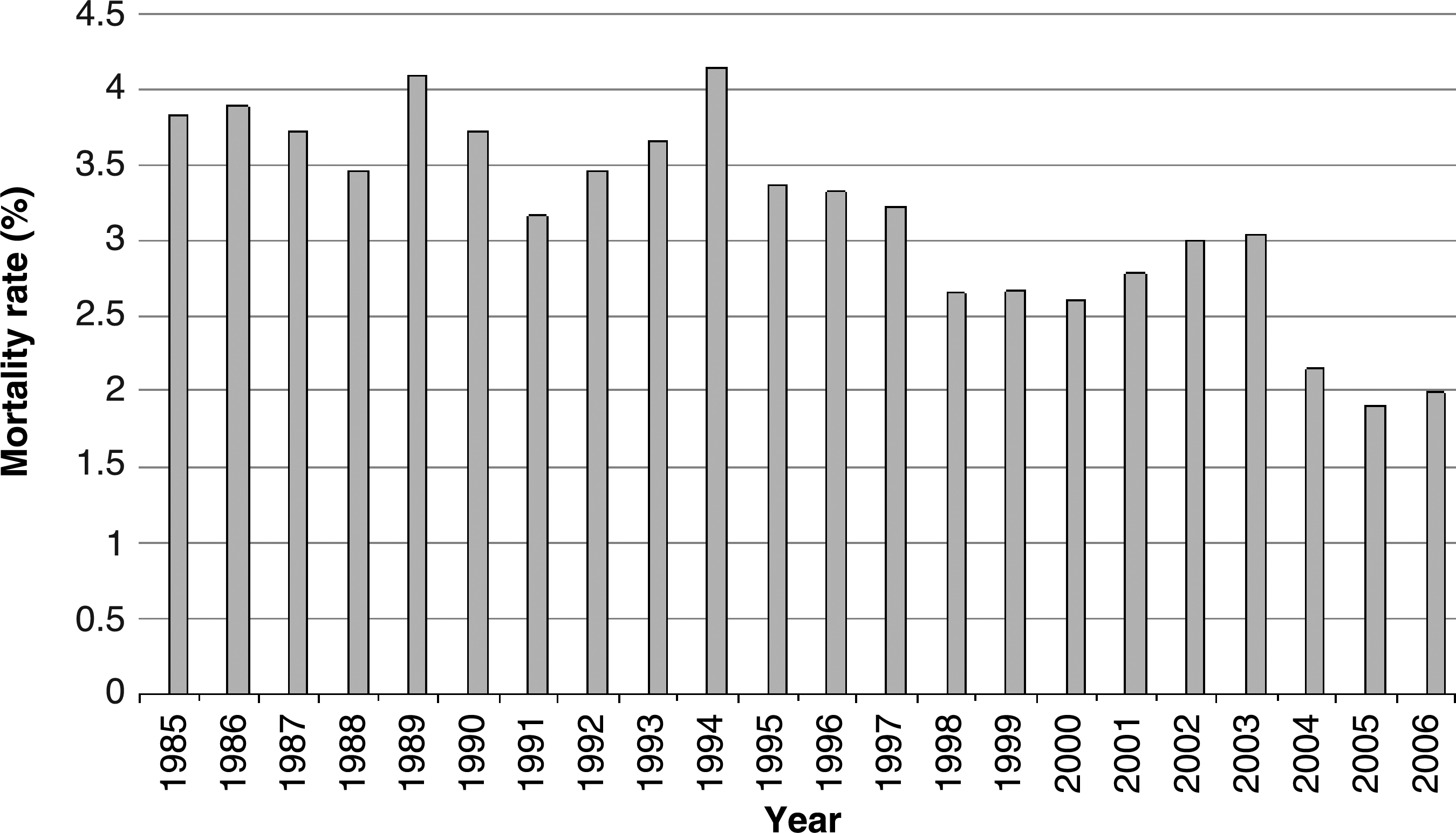
Mortality rate for burn-injured patients discharged from the New York City institutions is shown by year.
On the basis of the SPARCS data, the Shires Burn Service discharged over 16,000 patients from 1985 to 2006 (Fig. 3), which was 28% of all the burn patient discharges and 48.5% of patients discharged from burn centers in the region. In 1988, the Shires Burn Service admitted nearly 100% of all patients who were cared for in burn centers in the region, and this high proportion continued at 84.6% through 1995. Data obtained from the center registry and archives show the distribution of admissions to this center from its opening in 1976 through 2008 (Fig. 4) and confirm the SPARCS data that demonstrated an increase in admissions with a peak in 1995–1996, a gradual decrease after that and a more recent rise. There have been more than 18,000 admissions to this center since 1976.
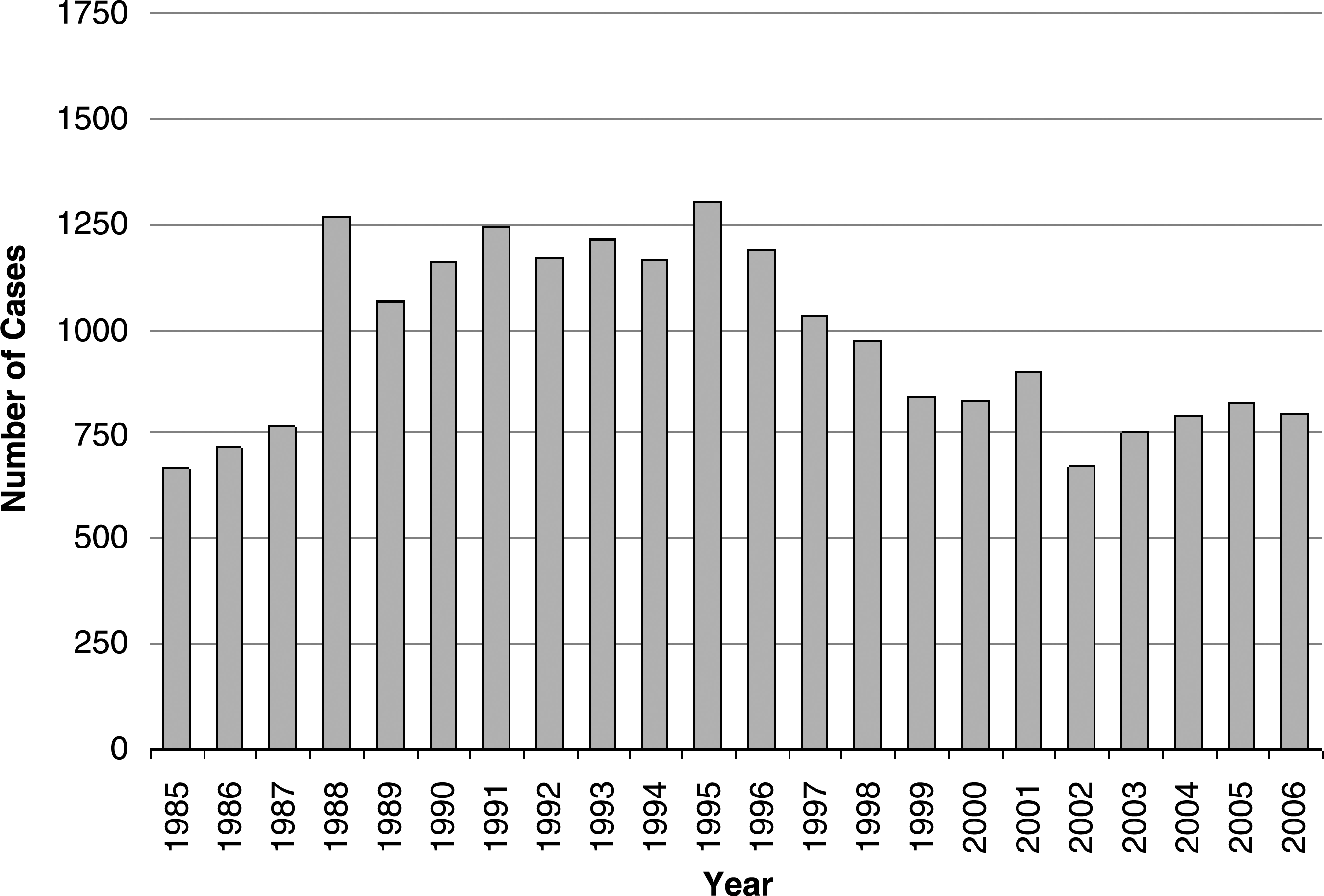
Burn-injured patient discharges from the Shires Burn Service are shown by year. Data are from the Statewide Planning and Research Cooperative System database.
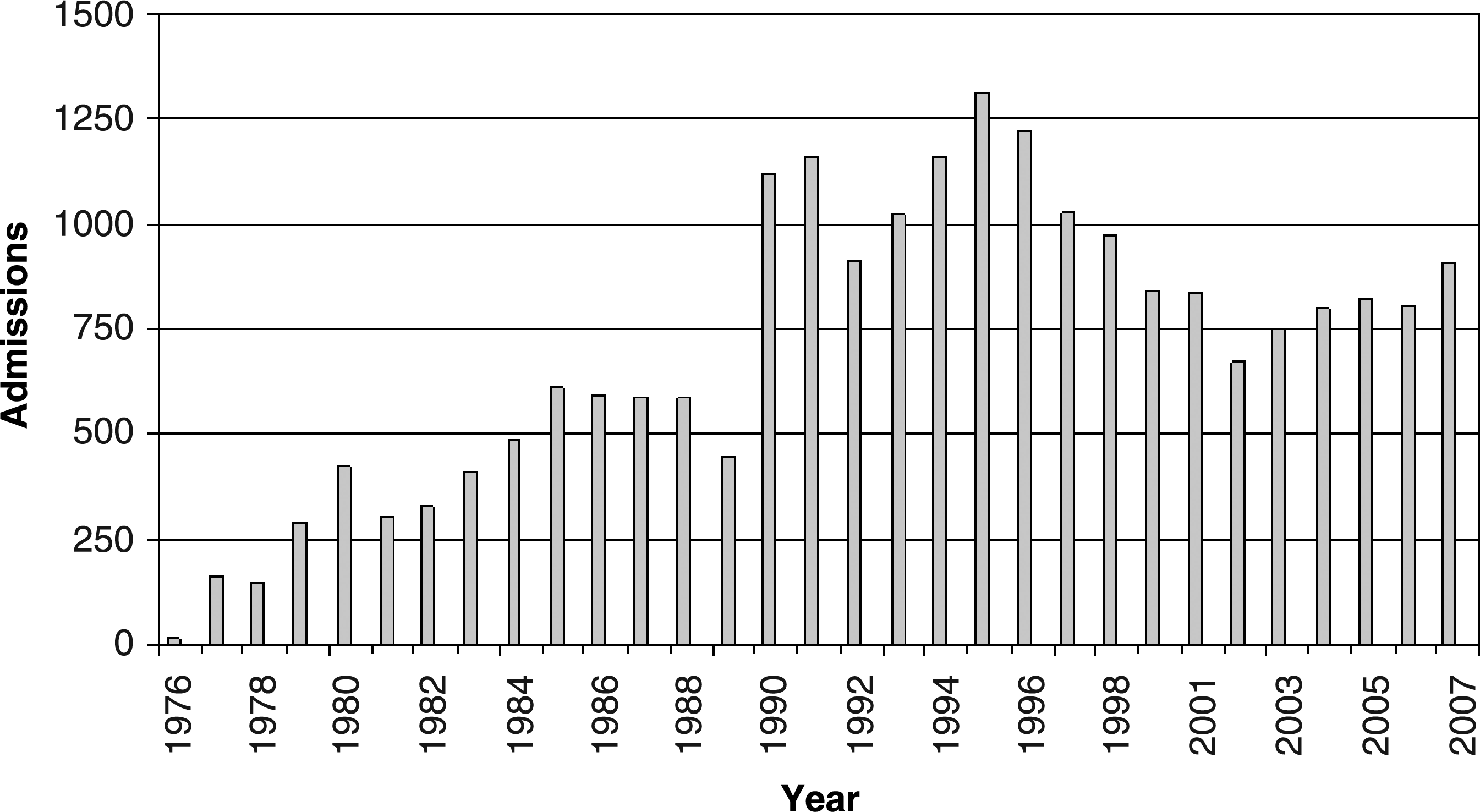
Burn-injured patient admissions to the Shires Burn Service are shown by year. Data are from archives before 1987, from local database 1987–1997 and the National Trauma Registry of the American College of Surgeons (NTRACS) 1998–2007.
The distribution of patients admitted to the burn centers in the region changed over time with a majority of patients admitted to the Shires Burn Service in the early years (Fig. 5). The opening of a burn program in Staten Island in 1997 was associated with an increased number of admissions throughout the region, and the Shires Burn Service saw a decrease in admissions. Figure 6 indicates the current location and the number of Burn center beds in the New York City metropolitan region.

Burn-injured patient discharges from the Shires Burn Service compared with all other New York City Burn Centers are shown by year from 1985 through 2006.
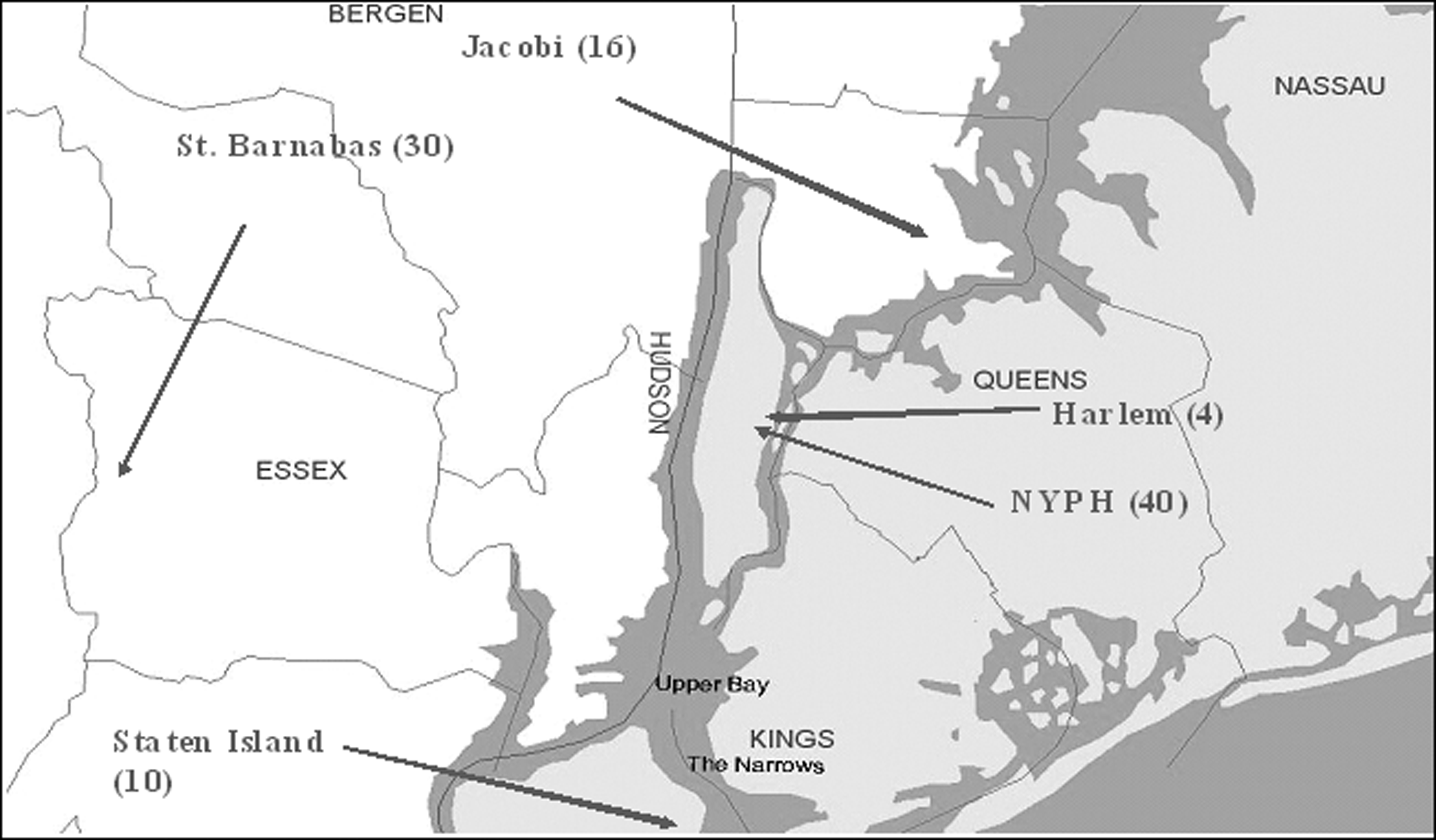
A map of New York City region with the sites of the burn centers indicated, their names, and the current number of beds of the burn-injured patients. NYPH; NewYork-Presbyterian Hospital.
In 1975, there were 137,237 fires in New York City, including 54,957 structural and 82,280 nonstructural [6]. By the year 2008 these numbers had decreased to 44,054, 26,862, and 17,192, respectively (Fig. 7).
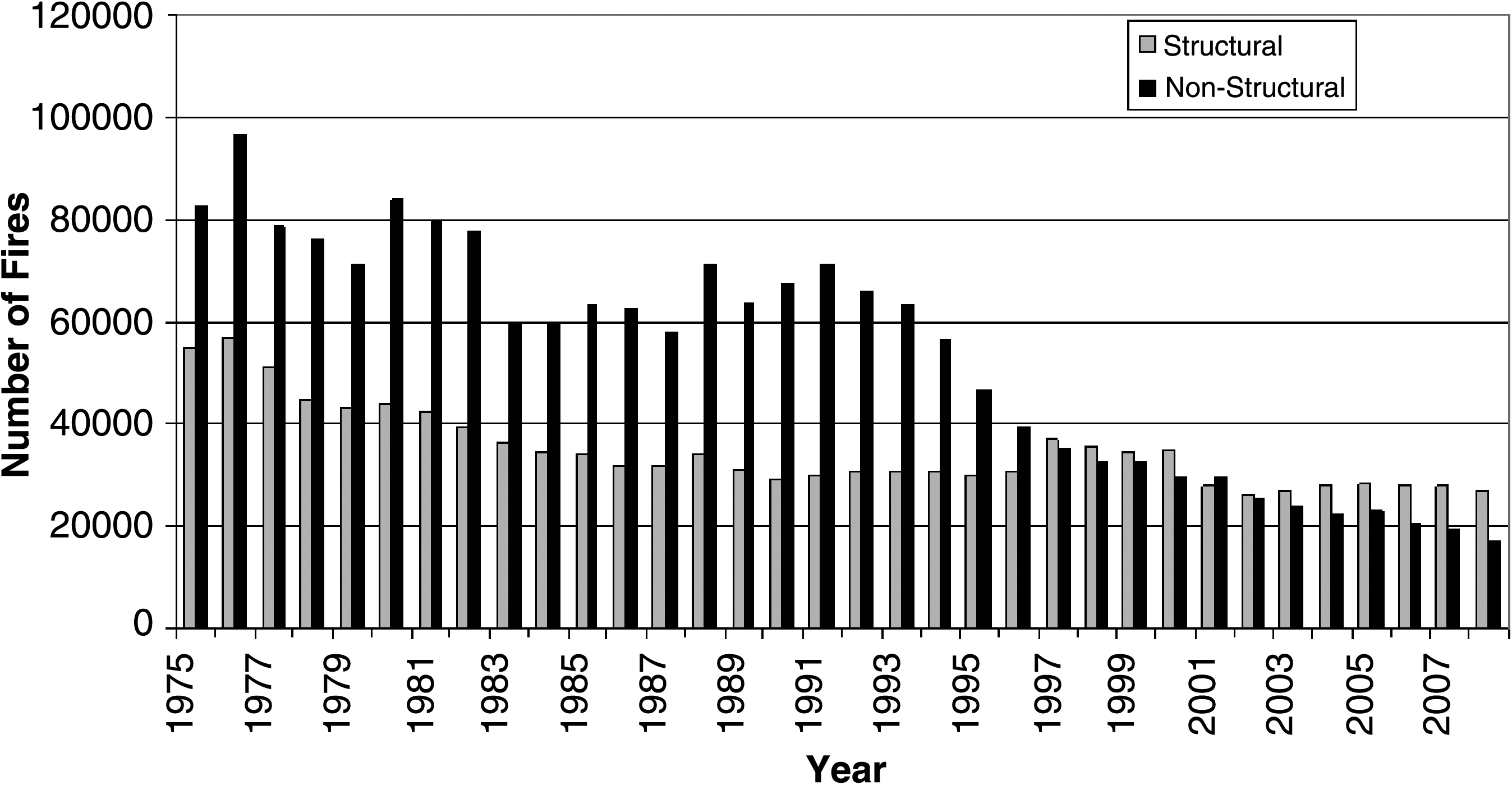
Number of structural and nonstructural fires in New York City by year (data obtained from the Fire Department of New York City [6]).
Discussion
There are no data available that document the number of hospitalized burn-injured patients in New York City at the time when the regionalized system was developed. However, the data provided by Feck and Baptiste [7] indicate that the incidence of admission for burn care in the rest of New York in 1975 was 269 per million population. Analysis of the current SPARCS dataset indicates that the incidence of burn patient admissions for 2003–2004 was 137 and 261 per million population for New York State (not including New York City) and New York City, respectively [5]. Assuming that the relative incidence remained the same over time, these data suggest that the incidence in New York City in 1975 would have been 512 per million population. On the basis of the New York City population at the time of 7,567,000 [5] and the incidence, the number of burn-injured patients in need of hospitalization could be estimated to be 3,874. This number is consistent with the more recent SPARCS data that show a trend of a decrease in admissions at approximately 70 patients per year from 1985 to 1995. Overall, this indicates that there has been a 43% decrease in hospital admissions for burn injury in the 30 years since inception of a regionalized approach to burn care. Although there are surely multiple factors that have contributed to this decline, clearly a major component is prevention. The number of fires in the New York City during this period is more than remarkable for the 137,237 that occurred in 1976 and for the decrease by 2008 of 33%, 49%, and 21% for the total, structural, and nonstructural fires, respectively. These data provide only a partial explanation for the change. Children make up 35% of the admissions at this institution, and a vast majority of those injuries are because of hot liquid exposure.
As the numbers of burn patient admissions decreased overall, the number that are cared for at specialized treatment centers has increased dramatically from very few in 1975 to 77.3% in 2006. That a significant increase has occurred recently is documented by the findings that at the time of the 2001 World Trade Center disaster, only two-thirds of the patients were being triaged to burn centers [8]. Substantial changes have occurred in the city since that time with major adjustments in the emergency medical services [9]. In addition, initiatives in disaster planning have heightened the awareness of and the need for appropriate triaging of patients [10]. Educational programs for prehospital, emergency department, and trauma center staff have been developed and distributed in the region as part of that process. From this center alone outreach programs are now in personal contact with more than 10,000 citizens through more than 125 programs on an annual basis. This does not include media-sponsored reports and public service announcements provided by the center.
Finally, the impact of the development of organized care can be seen in the professional education in the region. The Shires Burn Service has provided an educational program in critical care and burn care throughout the region to over 1,400 surgical residents and has provided fellowship level training for over 50 individuals. Seven surgeons whose primary practice is burn care in this region are the members of the Shires Burn Service or received training on the service.
Footnotes
Disclosure Statement
No conflicting financial interests exist.
Presented at the Memorial Celebration and Festschrift for Doctor G. Tom Shires, New York, New York, October 25, 2008.