
Abstract
Abstract
Background:
Bilateral iliopsoas abscess is very rare and has never been reported in cases of aortic graft infections. To date, only cases of unilateral abscess have been reported in association with aortic graft infection, and even these are uncommon.
Methods:
Case report and literature review.
Results:
We present the first report of an infected abdominal aortic graft, secondary to an ileal perforation, in a 76-year-old woman presenting with bilateral iliopsoas abscess. The presence of lumbar spondylodiscitis initially led us to suspect this as the primary cause of the abscess. Hence, she was treated initially with drainage of the abscess, percutaneously and surgically. This proved to be unsuccessful. A laparotomy, excision of the aortic graft, and in situ revascularization with a femoral venous conduit was performed subsequently. The bilateral iliopsoas abscess was found to be caused by a perforation of the ileum. Despite the surgery, the patient finally succumbed.
Conclusions:
Bilateral iliopsoas abscess secondary to infected aortic graft is extremely rare and challenging. Drainage of the abscess, percutaneously or surgically, and excision of graft with or without revascularization must be considered carefully based on the individual case.
Background
Case Report
A 76-year-old Caucasian woman presented with a gradual onset of intermittent low back pain and a deep sensation in her anterior thighs aggravated by walking for over six months. This was associated with weight loss and sweats. Ten years earlier, she underwent an elective repair of an inflammatory infrarenal abdominal aortic aneurysm with a straight woven polyester graft. Her other medical history included atypical polymyalgia rheumatica, diverticular disease of the colon, type II diabetes mellitus, psoriasis, and hypothyroidism.
Clinical examination revealed no abdominal or spinal tenderness, but there was a reduction of the range of movement of her lumbar spine. Her blood tests revealed increased inflammatory markers, including an erythrocyte sedimentation rate of 94 mm/h, white blood cell count of 13.9 × 109/L (normal range: 3.5–11 × 109/L), and C-reactive protein of 88 mg/L (<5 mg/L). She was also mildly anemic (normochromic), with hemoglobin of 11.2 g/dL (11.7–15.7 g/dL). Her blood urea nitrogen, electrolytes, and renal and liver function were within the normal range. Plain films of the lumbar spine revealed loss of joint space between L3 and L4, and small erosions of the vertebrae.
She was treated with a course of flucloxacillin for spondylodiscitis, which only partly relieved her symptoms. It was then considered that reactivation of polymyalgia rheumatica might explain the clinical picture. She was commenced on prednisolone 20 mg daily and referred to a rheumatologist. The rheumatologist noted no improvement from prednisolone and thought polymyalgia rheumatica unlikely. Further investigations were arranged.
Magnetic resonance imaging scan of her lumbar spine was performed. This revealed an abnormal signal in the L3 and L4 vertebral bodies (Fig. 1). In addition, there was soft tissue thickening anterolateral to the vertebral bodies. A computed tomography scan of her abdomen and pelvis showed bilateral iliopsoas abscesses infiltrating the tissues around the aortic graft (Fig. 2). To exclude sepsis originating from the intestine, she had a flexible sigmoidoscopy and barium studies (follow through and enema). They revealed only sigmoid diverticulosis, but no fistula or bowel perforation was identified.

Lateral view of the magnetic resonance imaging lumbar spine (T1-weighted) showing abnormal signal in the L3 and L4 vertebral bodies. There was a loss of disc height at this level.

Computed tomography scan revealed bilateral psoas abscesses with pockets of gas near the aortic graft.
An initial diagnosis of bilateral iliopsoas abscess secondary to an infective spondylodiscitis was made. As she was stable clinically and feeling relatively well, a decision to treat her abscess with drainage and systemic antibiotics was taken. Over the subsequent four months, she had multiple radiologically guided percutaneous and surgical drainages of the bilateral iliopsoas abscess while she was hospitalized. She also received various systemic antibiotics through a Hickmann catheter, including ciprofloxacin, flucloxacillin, metronidazole, meropenem, clindamycin, and voriconazole. The antibiotic regimens were based on the sensitivities of positive microbiology cultures of the pus drained (Table 1) and blood. None of the cultures were positive for acid-fast bacilli.
Multiple percutaneous and surgical drainages (six and two, respectively), and intensive systemic antibiotic therapy had not produced sufficient clearance of the abscess. This was despite a repeat magnetic resonance imaging scan of the lumbar spine showing healing spondylodiscitis of L3 and L4. Although the patient was stable clinically, including mobilizing independently and feeding normally throughout this period, she was deteriorating slowly. Due to our increasing concern regarding her infected aortic graft, she underwent an aortic graft excision, surgical washout of the bilateral iliopsoas abscess, and in situ aortic revascularization with a femoral vein graft. At laparotomy a pinhole-size perforation of the terminal ileum was found adherent loosely to the aortic graft. There was dark staining around the part of the graft where the bowel perforation was lying, suggesting that the bowel leak had been there for some time rather than iatrogenic (Fig. 3). An aortoenteric fistula was considered a possibility although the patient did not present with any melena or bleeding per rectum. The bowel was dissected off the aortic graft and repaired. The aorta was then clamped infrarenally and the aortic graft was excised. A left femoral vein conduit was harvested. The vein was then fashioned into a tube graft between the infrarenal aorta and aortic bifurcation. Microbiology tests on the aortic graft were negative. However, the clinical picture was clearly consistent with a case of aortic graft infection.
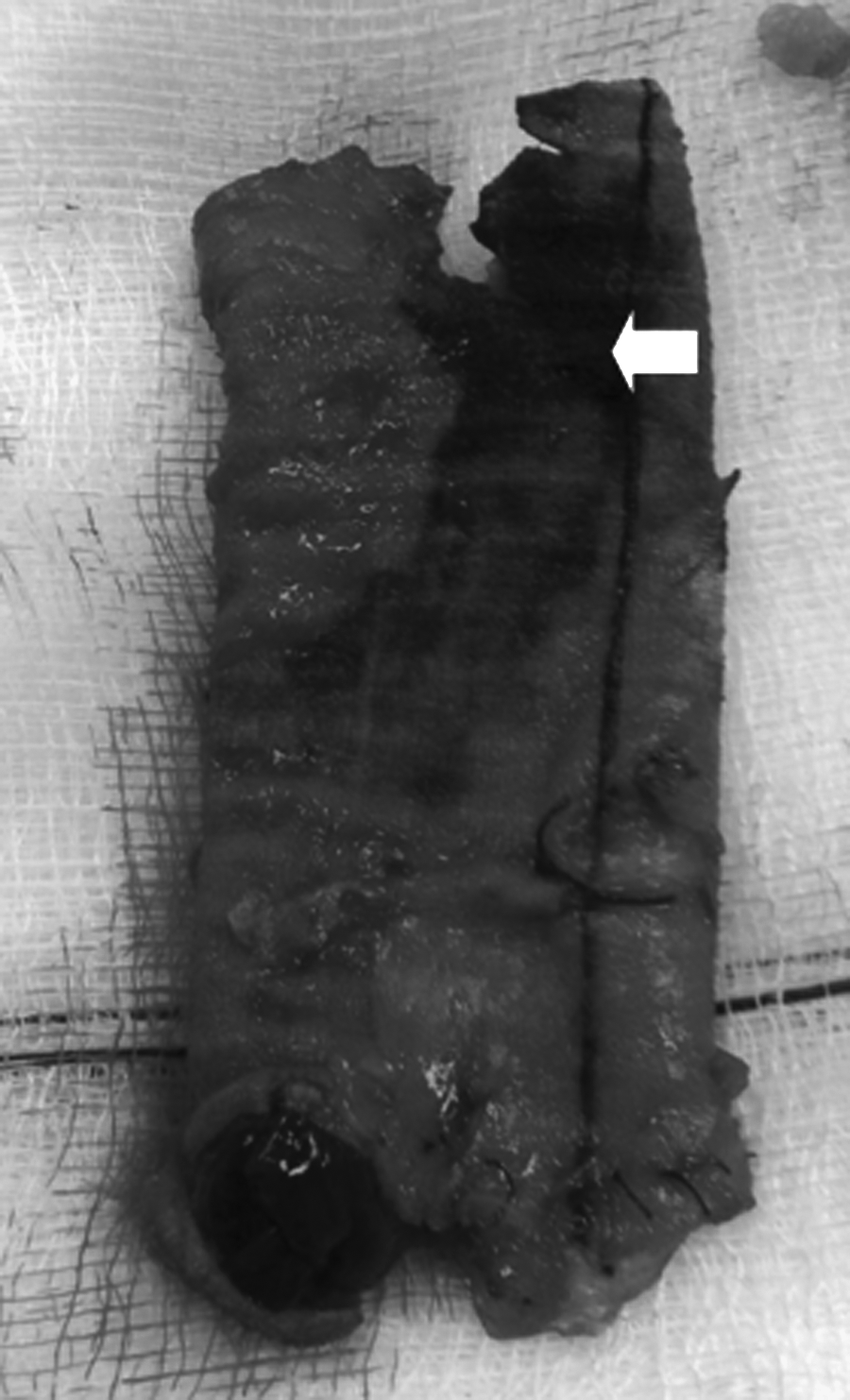
Excised infected aortic graft. The dark staining on the graft indicated by the white arrow was where the bowel perforation was directly lying over.
Her initial postoperative recovery was satisfactory. However, she later developed a false aneurysm at the anastomotic site of the vein graft that was likely to be caused by the continuing infection of the graft site. When she re-presented to our hospital, she deteriorated rapidly with sepsis and multi-organ failure, including kidney, chest, and liver dysfunction. At this point we decided that she would not benefit from further invasive treatment, which decision accepted by the patient and her family, and she died subsequently.
Discussion
Iliopsoas abscess was first described by Mynter in 1881 and was referred as psoitis [4]. Primary iliopsoas abscess accounts for 99% of all the cases in developing countries, as compared to 17% and 61% in Europe and North America, respectively [1]. Staphylococcus aureus is the most common pathogen in primary iliopsoas abscess, seen in 88% of cases as a single causative organism [5]. The most common cause of secondary iliopsoas abscess is infection from the gastrointestinal tract, such as inflammatory bowel disease, diverticular disease of the colon, appendicitis, and malignant disease. Of these, Crohn's disease is the most common cause [2,5]. Other causes of secondary iliopsoas abscess include urinary tract infections, septic arthritis, vertebral osteomyelitis, and infected abdominal aortic aneurysms [2]. Cultures from a secondary iliopsoas abscess usually demonstrate mixed organisms, predominantly with Escherichia coli and Bacteroides spp. [5]. Mycobacterium tuberculosis from spinal osteomyelitis (Pott disease) is the most common cause of secondary iliopsoas abscess in the developing world [6].
The management of iliopsoas abscess should involve drainage and the use of appropriate antibiotics [2]. Drainage can be performed percutaneously under radiological guidance, or surgically. Cantasdemir et al. reported that percutaneous drainage of iliopsoas abscess was effective in 21 of 22 cases [7]. Percutaneous drainage has the advantage of being less invasive, with a low mortality and morbidity rate [2]. Surgery is an important treatment option especially when the cause of the iliopsoas abscess has to be dealt with surgically. A combination of both percutaneous drainage and surgery, with the former being the initial treatment, has also been described [8].
The mainstay of treatment of an infected aortic graft is surgery. Surgery for an infected aortic graft generally involves the removal of the graft with or without revascularization. Revascularization can be done with an in situ conduit or an extra-anatomical bypass [9].
Although an earlier surgical exploration was an option in our case, we opted for the less invasive treatment, that is, drainages of abscess instead. In iliopsoas abscess associated with infected aortic grafts, both percutaneous drainage and surgery have been reported to be effective in case reports. Melissano et al. described four cases of aortoiliac infection with unilateral iliopsoas abscess [3]. Two of the iliopsoas abscesses were caused by aortic graft infection secondary to enteric fistulas. Both cases were treated successfully: One with graft removal and axillobifemoral bypass graft, and the other with percutaneous computed tomography-guided drainage.
To our knowledge, our case was the first report of bilateral iliopsoas abscess associated with an infected aortic graft. Our case was also challenging because of the presence of a lumbar spondylodiscitis as a “red herring,” complicating the diagnosis of the disease and management of the patient. Spinal infection, especially from M. tuberculosis, is a well-recognized cause of bilateral iliopsoas abscess [9–11]. Worse still, the endoscopy and barium studies did not reveal bowel perforation, masking the cause of the problem further. During the surgery, we did not excise any intestine because the small perforation was easily repaired with suture. We also did not take any intestinal biopsy as this would cause further trauma and would not change the management at least in the early stage. Therefore, there was no histological diagnosis of the intestinal perforation. There was a possibility that it was caused by her occasional intake of high-dose steroids for her polymyalgia rheumatica. Prolonged antibiotic therapy in our case might have also complicated the case further by altering the types of organisms cultured from the pus and blood sampled from the patient. This was clearly demonstrated by the variations shown by the culture results over time and the negative microbiology tests of the aortic graft. It is also important to stress that extended-spectrum beta-lactamase producing bacteria were not routinely tested for by our hospital microbiology laboratory at that time. However, in hindsight, it was likely that some of the microorganisms cultured were likely to be extended-spectrum beta-lactamase positive, which is at present routinely tested in our hospital microbiology laboratory.
We decided on an in situ aortic revascularization with an autogenous femoral vein conduit. In situ prosthetic graft would have been too high an infective risk, and therefore a large autogenous graft was used, that is, femoral vein. In hindsight, an extra-anatomical bypass such as axillo-biprofunda femoris or bilateral axillo-profunda femoris bypass, especially avoiding the laterally placed puncture sites would have been a good option. Although this option was considered preoperatively, this was then believed to be difficult and carry a high infective risk due to the proximity of the path taken by the graft from the contaminated tracts formed from previous percutaneous and surgical drainages. This was obviously a very difficult decision to be made at that time because the infective risk of both options in this particular case was considered to be comparable. We ultimately opted for the former because at that time, we felt that the use of an in situ autogenous vein graft with a reasonable excision of the infected graft bed would have a lesser infective risk than the latter. Therefore, this case also demonstrated that the decision to perform percutaneous and surgical drainages of abdominal abscesses with the presence of an infected abdominal aortic graft must not be taken lightly as they might contraindicate future extra-anatomical revascularization.
We conclude that bilateral iliopsoas abscess secondary to infected aortic graft is extremely rare and challenging. Drainage of the abscess, percutaneously or surgically, and excision of graft with or without revascularization must be considered carefully based on the individual case.
Footnotes
Author Disclosure Statement
The authors declare no conflicts of interest.