
Abstract
Abstract
Background:
Although tube thoracostomy with fibrinolytic agents and video-assisted thoracoscopic (VATS) decortication are relatively equivalent in the treatment of empyema with regard to time to patient defervescence and hospital discharge, the potential for greater benefit with VATS decortication in the setting of advanced empyema has not been explored fully. This paper describes our transition from a policy of drainage and antibiotics to primary operative management with VATS. We wanted to assess the safety and efficacy of primary operative management as a first-line treatment for advanced disease.
Methods:
A retrospective review was conducted of 25 patients treated for stage 3 or 4 empyema. The primary endpoints were morbidity and death. The secondary endpoints were conversion to an open procedure, time to defervescence, and length of hospital stay.
Results:
The morbidity rate was 16% with no deaths. No patient required conversion to open decortication. The mean time to defervescence was 3.2 days, and on average, patients were discharged on postoperative day 9. Patients were discharged home earlier when managed primarily with VATS.
Conclusions:
Video-assisted thoracoscopic decortication is a safe and effective treatment for pediatric stage 3 or 4 empyema.
It is well established that parapneumonic effusions and pleural space infection can be subcategorized for severity on the basis of the chemical, bacteriologic, and physical characteristics of the effusion fluid [1,2]. The American College of Chest Physicians (ACCP) developed a four-part staging system for risk stratification. The system is particularly useful in that parapneumonic effusions are graded largely on radiologic evidence. In this system, stage 1 effusions are small (<1 cm on lateral decubitus radiographs), stage 2 effusions are of moderate size (less than half of the hemithorax), and stage 3 and 4 effusions are large (greater than half of the hemithorax), contain loculations, or are associated with thickened pleura. Stage 4 effusions are differentiated from stage 3 collections by the presence of pus. Whereas stage 1 effusions usually resolve with antimicrobial therapy alone with or without chest tube drainage, higher-stage effusions are more likely to persist and necessitate lytic therapy, surgical decortication, or both for complete resolution. Which treatment is best for initial therapy is still debated. Two recent randomized studies comparing VATS directly with tube drainage and fibrinolytic agents concluded that these treatments are equivalent with regard to time to defervescence and time to discharge [11,25]. However, both studies included patients with all ACCP stages of parapneumonic effusions.
In this study, we assessed the outcomes of our treatment of pediatric stage 3 and 4 empyema after our transition to primary VATS and compared them with our earlier experience treating empyema with tube drainage with or without fibrinolytic agents and delayed operation.
Patients and Methods
A retrospective review was performed of all patients under the age of 18 years who underwent VATS decortication for parapneumonic effusions at Kapi'olani Medical Center for Women and Children between July 1, 2002, and February 28, 2007, who were identified from a prospective database of all patients treated by the hospital's pediatric surgery service. During the last three years, patients were treated primarily with early VATS, and if preoperative drainage was attempted, it was done prior to the surgical consultation. All procedures were performed by one of two pediatric surgeons.
Inpatient medical records were reviewed for age, sex, medical conditions, duration of outpatient symptoms, pre-hospital use of antibiotics, preoperative interventions, preoperative radiologic findings, time to surgery, operative time, intraoperative complications, conversion to open thoracotomy, number of chest tubes placed, duration of chest tube use, microbiologic analysis, time to defervescence, and time to discharge. Outpatient medical records were reviewed for postoperative complications. Patients were classified as having stage 3 or 4 empyema according to the system of Colice et al. [1].
Data are expressed as mean ± standard error of the mean for each group unless otherwise indicated. Differences between children treated with a chest tube prior to surgery and those who received VATS only were determined using a Student t-test. A p value of <0.05 was considered to be significant.
Results
Patient characteristics
A total of 25 patients met the inclusion criteria (Table 1). There were nine boys and 16 girls, with a mean age of 4.6 ± 0.7 years (range seven months–14 years). Eight patients had a chronic medical condition: Seven patients had asthma, and one had congenital hearing loss. Thirteen patients had stage 3 empyema, and 12 had stage 4 empyema. A causative agent was identified by respiratory or pleural fluid cultures in 11 patients: six Streptococcus pneumoniae, four Staphylococcus aureus, and one Escherichia coli. A necrotizing component was present in 12 patients.
Preoperative course
Prior to hospitalization, patients had been symptomatic for a mean of 7.7 ± 1.1 days, and 17 patients had received outpatient antibiotics (Table 2). Once admitted to the hospital, the mean time to the operating room was 3.0 ± 0.6 days, and the mean time from surgical consultation to the operating room was 1.2 ± 0.4 days. This mean time decreased from 1.8 ± 0.8 days for the first 12 children to 0.5 ± 0.2 days for the second 13 children (p = 0.5) (our transition to primary operative management). Prior to operation, seven patients underwent chest tube drainage, and one patient received fibrinolytic therapy. Chest tubes were left in place for a mean of three days prior to declaring treatment failure and proceeding with decortication.
Radiologic studies
All patients underwent radiographic assessment prior to operative intervention. One patient was assessed with radiographs alone. Five patients were evaluated with a combination of radiography and ultrasonography, and eight patients had a combination of radiographs and computed tomography (CT) scanning.
Operative course
The mean operative time was 102 ± 10 min. The operative time decreased as experience increased, from 127 ± 16 min for the first 12 cases to 83 ± 9 min for the second 13. Two to four ports were necessary, with a trend toward more frequent use of only two ports in the more recent cases. Care was taken to break up all loculations and peel off all pleural rinds. No cases were converted to open decortication. The mean estimated blood loss was 43 ± 11 mL (2.3 ± 0.6 mL/kg). In the more recent patients, only one chest tube was placed routinely. If a patient had a preoperative drain or tube, that site was used for the trocar or drain after the VATS. All but two patients were extubated at the conclusion of the case.
Postoperative course
A chest drain remained in place for 2.9 ± 0.2 days after surgery. The time to defervescence was 3.2 ± 0.4 days, where defervescence was defined as 24 h with a temperature <101.1°F. Patients with stage 3 empyema defervesced after 3.6 ± 0.8 days, whereas patients with stage 4 empyema took 3.7 ± 0.8 days (Table 2). The time to discharge after surgery was 7.5 ± 0.8 days (range 2–15 days). Patients with stage 3 or 4 empyema were discharged after a mean stay of 7.5 ± 1.1 days. There were no postoperative bronchopleural fistulas.
There were four postoperative complications (16% of patients). Two patients had either a loculated collection of fluid or air in the chest that necessitated subsequent treatment or drainage. There was no evidence of residual or recurrent empyema, bronchopleural fistula, or pleural space disease in either child. Another child had a port-site infection that was treated with outpatient antibiotics. A fourth patient, found to have empyema necessitans prior to VATS, developed osteomyelitis of the rib away from the port sites. The patient was re-admitted and treated with intravenous antibiotics with complete resolution of the infection.
Effects of preoperative chest tubes
Initial treatment with a chest tube resulted in a significant delay in the time to operative treatment, from 2.7 ± 0.5 days to 7.1 ± 1.3 days (Table 3), and prolonged hospitalization. The operative time was significantly longer and the estimated blood loss was significantly greater if a chest tube was placed prior to VATS: 87 ± 11 vs. 139 ± 10 min and 30.6 ± 10.5 mL (1.8 ± 0.7 mL/kg) vs. 78.3 ± 26.1 mL (4.0 ± 1.3 mL/kg). Postoperatively, chest tubes remained in place longer if one had been placed before surgery (2.6 ± 0.2 vs. 3.6 ± 0.4 days). The time to defervescence was not affected significantly by the preoperative measures (3.3 ± 0.6 days without a chest tube vs. 2.7 ± 0.5 days with a chest tube). The time from surgery to discharge displayed a statistically non-significant trend toward a longer stay with a preoperative chest tube (6.8 ± 0.8 vs. 9.3 ± 1.6 days). The overall hospital stay was a week longer if a chest tube was used preoperatively: 16.5 ± 1.4 vs. 9.1 ± 0.7 days (p < 0.005). There was no difference in complications in the two groups.
Discussion
We have become more aggressive with early operative management for stage 3 and 4 empyema in children over the last several years. Surgical consultation is being requested earlier by pediatricians and infectious disease specialists, and patients are being managed with primary VATS for advanced empyema. In this study, we sought to review our experience and assess the outcomes of this approach and compare them with our earlier experience treating stage 3 and 4 empyema with tube drainage with or without fibrinolytic agents and delayed operation. We found, as have others, that our patients had a shorter hospitalization and suffered minimal morbidity with primary operative management [26]. All were managed successfully with minimally invasive techniques.
The traditional “non-operative” approach to pediatric parapneumonic effusions includes thoracentesis and antibiotic therapy. Thoracentesis allows visual inspection of the effusion fluid, Gram stain and culture, and chemical analysis for pH, glucose, and lactic dehydrogenase. Chest tubes are placed in patients with large effusions or when evidence of empyema exists. Both of these interventions will require sedation or general anesthesia in most children. In a recent meta-analysis that included 3,418 patients treated non-operatively initially, the failure rate was 23.6%, the length of stay was 20 ± 8.3 days, and chest tubes were left in place an average of 10.6 ± 3.4 days [5]. We found that chest tube placement preoperatively resulted in a delay in surgical intervention and a longer total hospital stay.
The use of fibrinolytic agents has gained support as an alternative to chest tube drainage alone for pediatric empyema. Tokuda et al. reported a meta-analysis of randomized controlled trials in adult patients comparing fibrinolytics with placebo [8]. Among 575 patients treated in five trials, there was a 27.6% statistically non-significant reduction in death or need for surgery utilizing fibrinolytics vs. a 32.8% rate for placebo. These investigators concluded that although fibrinolytic agents may be beneficial for some patients, their use could not be supported for all patients.
There now are several studies in which patients were randomized to primary VATS vs. primary chest tube drainage with fibrinolytic agents and VATS as rescue therapy. Three recent randomized trials in children offer interesting results. Kurt et al. randomized 18 patients to early VATS or conventional chest tube alone [10]. They found a shorter stay (5.8 vs. 13.3 days) and days with a chest tube in place (2.8 vs. 9.6) with VATS. Sonnappa et al. found no significant difference in the length of stay or days with a chest tube in a group of 60 patients randomized to either primary VATS or conventional chest tube with fibrinolytic therapy [11]. However, they reported a failure rate of 17% in each group. Of particular note is that four of the five VATS failures were based on the surgeon's opinion at the initial procedure that the peel was too thick to be removed by that route and necessitated immediate open thoracotomy. The other failure required a second VATS. In comparison, all the failures in the chest tube and fibrinolytics group necessitated surgery. Similar results were reported by St. Peter et al., who randomized 36 patients to either primary VATS or fibrinolysis. They found no difference in the length of stay or time to defervescence. They did find a 17% failure rate with fibrinolysis, all of which patients required rescue VATS [25]. In total, these studies suggest that the two treatment approaches have similar outcomes, although the failure rate is higher with fibrinolytic therapy. However, two studies have concluded that tube drainage with fibrinolytics may ultimately be the preferred therapy based on cost data [25,27], although others have concluded the opposite [28]. Of note, all of the studies demonstrating equivalency or benefit to tube drainage with fibrinolytic agents included patients with any stage of empyema. In contrast, our study was restricted to stage 3 and 4 empyema, where we believe VATS may eventually prove to have greater benefit.
Early reports of small series of patients treated with VATS showed frequent conversion to open thoracotomy or return to the operating theatre for open thoracotomy to remove more of the peel encasing the lung [12–14]. However, this was not confirmed in reports of pediatric patients by others, who reported no cases of failed VATS necessitating open thoracotomy [16–19]. In our series, there were no cases requiring conversion to open thoracotomy. Although our series is small, we believe it shows that open thoracotomy for pediatric empyema should be increasingly rare as minimally invasive surgery experience improves. Many of our patients are now treated with a 3-mm two-port technique.
Complications directly attributable to VATS occur in 7–15% of patients [3,18,22]. The most common is a bronchopleural fistula, which can be seen with necrotizing pneumonia [3]. Our complication rate is similar to that described in other case series. This modest risk of complications and its effects need to be studied further; however, it does not appear to diminish the improvement in care that VATS offers.
Recently, there has been growing support for primary VATS with the goal of reducing length of stay and the total number of invasive procedures [21,22] The first report advocating VATS as initial therapy for all children with parapneumonic effusions was a small study by Kercher et al., who argued that because general anesthesia is required to place a chest tube in a child, thoracoscopic evaluation with decortication based on findings at the same time makes sense [22]. Additionally, a larger series from Poland advocated VATS as both a diagnostic and a therapeutic tool for all children with parapneumonic effusions [23].
In our experience, primary management with VATS decreased the hospital stay and often provided an important diagnostic tool when the severity of empyema or loculations was in question. Additionally, at our institution, when a chest tube or pigtail catheter is placed, it is placed under anesthesia or sedation; and sometimes, multiple tubes or anesthetics are required for replacement, manipulation of catheters, or secondary catheter placement. These repetitive anesthetics and secondary procedures were generally avoidable once we transitioned to primary operative management.
Ultimately, the main difficulty may be in judging which patients have true loculated stage 3 and 4 parapneumonic effusions or empyema. We believe this difficulty accounts for the success of fibrinolytic agents, which are most successful when treating unloculated stage 1 and 2 effusions. Both ultrasonography and CT scanning can be used in preoperative staging of parapneumonic effusions. Kalfa et al. favored ultrasonography in a series of 50 patients [3]. They argued that this modality is more reliable in evaluating the nature of pleural fluid, although they reported 77% sensitivity compared with operative findings. Additional support for ultrasonography comes from Meier et al., who concluded that the technique offered better views of the fibrin, but they qualify their statement with a note about the need for experienced radiologic personnel [4]. However, the same patient series relied primarily on CT results for staging, as the surgeons found it more helpful for planning an intervention. These modalities are not mutually exclusive, and each gives unique information that may be useful. Ultrasonography more accurately shows loculations and debris within the pleural fluid, which is essential for proper staging and subsequent selection of intervention. However, CT scanning more clearly shows the extent of the effusion and gives detailed information on the state of the underlying lung, information that likewise may alter the planned intervention.
We present an algorithm based on our experience and transition to early VATS for the management of advanced pediatric empyema (Fig. 1). We now favor early VATS (within 24 h of presentation) for all children with stage 3 or 4 empyema. We and many others have documented the success of the VATS technique with acceptably low morbidity. However, we recognize the success of some centers with lytic agents and agree that it is at least an equivalent therapy for low-grade (stage 1 and 2) parapneumonic effusions. Those patients who fail lytic therapy are then rescued with VATS. We also advocate VATS as a diagnostic and definitive therapeutic tool for cases in which there is uncertainty about the stage of empyema.
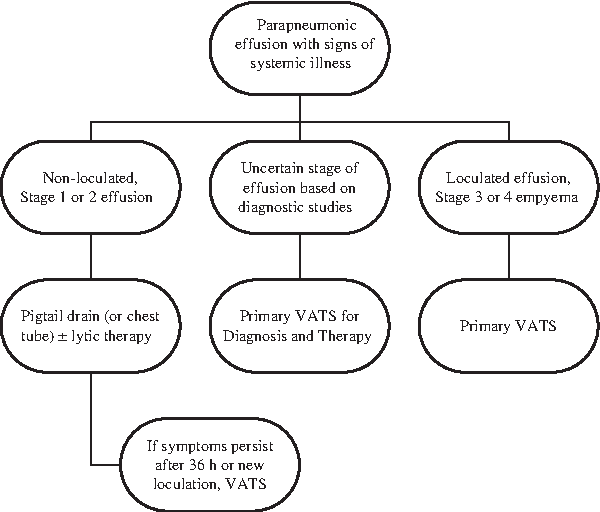
Algorithm for management of advanced pediatric empyema. VATS, video–arrested thoracoscopic surgery.
Conclusion
Our results confirm the high level of success with VATS in children with stage 3 or 4 empyema. No patients required conversion to open surgery, and the overall morbidity rate was low at 15%. We and others have shown a reasonable length of stay with VATS and a minimal number of days of chest tube drainage. We believe that the success of the VATS coupled with the minimum number of invasive procedures required strongly supports VATS as first-line therapy in advanced-stage empyema.
Footnotes
Author Disclosure Statement
No competing financial interests exist.