
Abstract
Abstract
Background:
Stapled hemorrhoidectomy (SH) is a modern approach for the management of hemorrhoids that can provoke life-threatening complications such as fulminant sepsis.
Methods:
Case report and review of the pertinent English-language literature.
Results:
A 23-year old man being treated with SH for third-degree hemorrhoids developed fulminant intra-abdominal sepsis as the result of a rectal injury during the operation. An exploratory laparotomy was performed. The rectal injury was sutured, and a temporary sigmoid loop colostomy was constructed.
Conclusions:
Anorectal injury during SH can provoke serious sepsis, which the surgeon must confront promptly and aggressively.
Case Report
A 23-year old patient was referred to our department with third-degree internal hemorrhoids (prolapsing, requiring manual reduction) and underwent elective SH. General anesthesia was administered, and standard perioperative care was provided. A 33-mm Proximate HCS Hemorrhoidal Circular Stapler (Ethicon, Inc., Somerville, NJ) was used. During the end steps of the operation, after removal of the stapler, there was bleeding at the staple line (right laterally). The site was oversewn with three additional 3-0 polyglycolic acid (PGA) sutures. As in all similar procedures, we performed a histologic examination of the “doughnut” (Fig. 1).
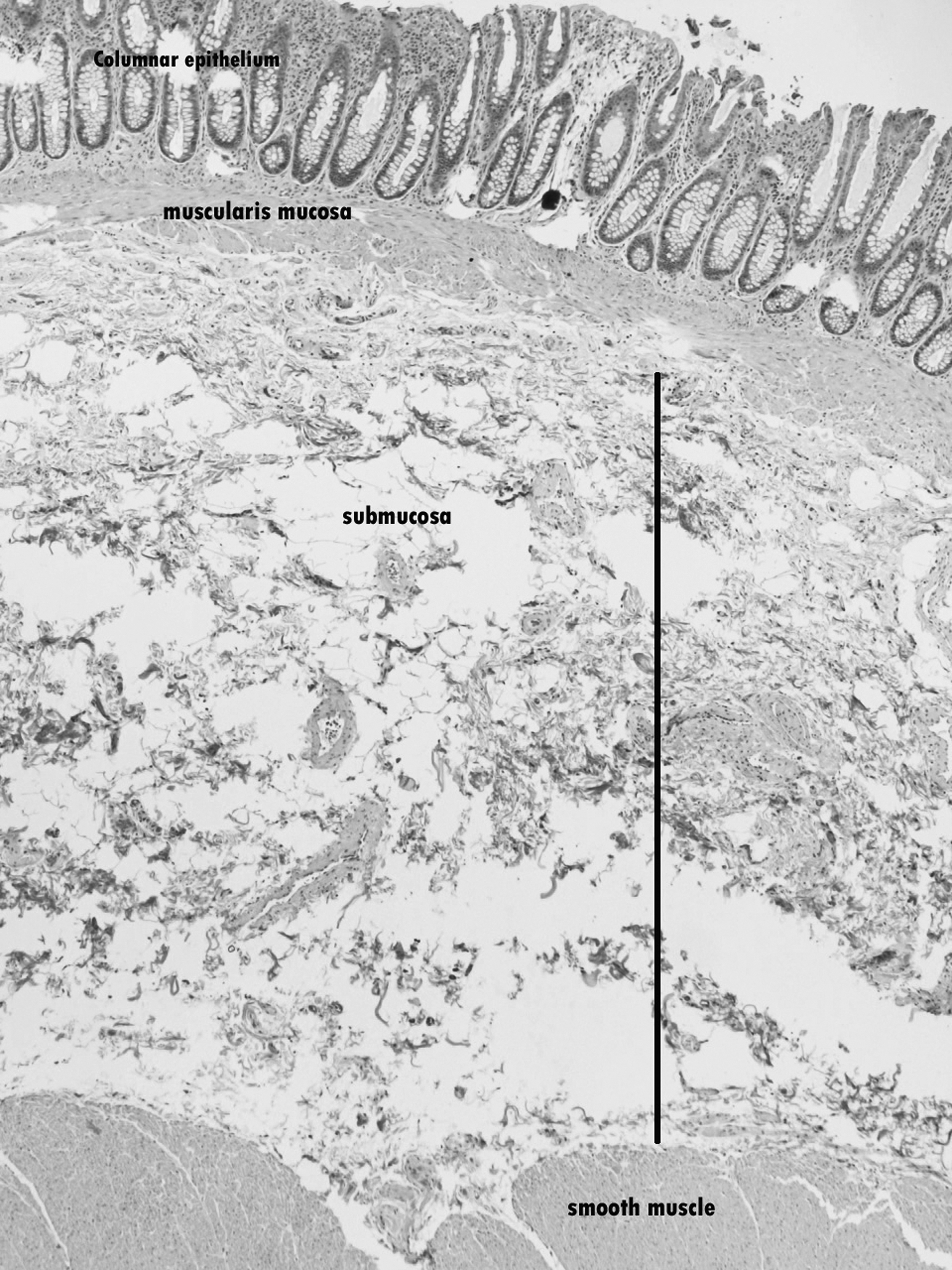
Histologic view of “doughnut.”
The patient was in good condition during postoperative day one. However, on postoperative day two, he complained of severe periumbilical and lower abdominal pain. Physical examination revealed diffuse abdominal tenderness with rigidity of the abdominal wall, rebound tenderness, and diminished sounds. The patient was febrile (38°C), tachycardic, and tachepneic and appeared ill. His hemoglobin concentration was low, 7.4 g/dL. He was given supportive management with intravenous fluids and packed red blood cells. We started immediate antibiotic therapy with ampicillin-sulbactam, aminoglycoside (amikacin), and metronidazole. The patient underwent a chest radiograph, which showed air under the dome of the right hemidiaphragm, and a CT scan, which showed free pararectal (Fig. 2A) and intraperitoneal (Fig. 2B) air and fluid collections in the presacral area, pouch of Douglas, root of the mesentery, and right paracolic area. The patient underwent an emergency exploratory laparotomy, which revealed a 2-cm linear rupture of the right lateral aspect of the rectum, under the peritoneal reflection, which was opened and devitalized because of severe inflammation. The rupture was closed with 2-0 polyglycolic acid interrupted sutures. The fluid collections (pus) were aspirated, and cultures were taken. The peritoneal cavity was irrigated copiously with normal saline and then drained. Finally, a temporary sigmoid loop colostomy was constructed.

Computed tomography scans.
The patient was in good general condition the first few postoperative days, the only problem being a continuous fever (38.5°C) despite the antibiotic regimen. On postoperative day five, the patient was still febrile, and the antibiotic therapy was changed according to the peritoneal fluid culture results. The cultures yielded Escherichia coli, Proteus mirabilis, and Enterobacter asburiae. The E. coli and Proteus were sensitive to several antibiotics such as penicillin, second- and third-generation cephalosporins, and carbapenems, whereas the Enterobacter asburiae was sensitive only to imipenem-cilastatin meropenem, and colistin. The patient was treated with imipenem-cilastatin monotherapy for 10 days. On postoperative day nine, the patient was still febrile, so we added linezolid for five days, according to a culture result from a surgical site infection obtained on postoperative day five that showed a Staphylococcus haemolyticus infection. The patient was afebrile after postoperative day 13, and he was discharged on postoperative day 15. The continuity of the large intestine was re-established two months later.
Discussion
Hemorrhoids are sacular formations (hemorrhoidal cushions) in the anal canal, consisted of prolapsing mucosa surrounding abnormally dilated veins of the internal hemorrhoidal plexus. A much dilated venous plexus can be compared to a cavernous-like tissue that has enclosed a large mass of venous blood. The resulting expansion of the anorectal mucosa results in the prolapse of hemorrhoidal pathology. In this situation, engorgement of submucosal vessels provokes edema that can fill the subcutaneous area of the perianal margins. The swelling may result in acute external and internal hemorrhoids with associated thrombosis and prolapse.
The main purpose of every surgical treatment of third- or fourth-degree hemorrhoids is to tie up, in a high position, all hemorrhoidal pedicles corresponding to each cushion. The method of Milligan-Morgan excises all protruding mucosa with the hemorrhoidal plexus, taking care to avoid the internal sphincter muscle in the plane of dissection.
In SH, hemorrhoidal tissue is not resected but rather repositioned and suspended in its natural position after circumferential mucosectomy. The most difficult part of the procedure is to define the appropriate distance of the purse-string suture from the anal margin and the depth the suture should pierce into the anal wall (Fig. 3). The correct position of the suture avoids both excess muscle incorporation into the “doughnut” and perforation of the rectum. It also permits efficient stapling of the hemorrhoidal plexus, avoiding the bleeding of a circular stapler suture and giving satisfactory permanent outcomes.
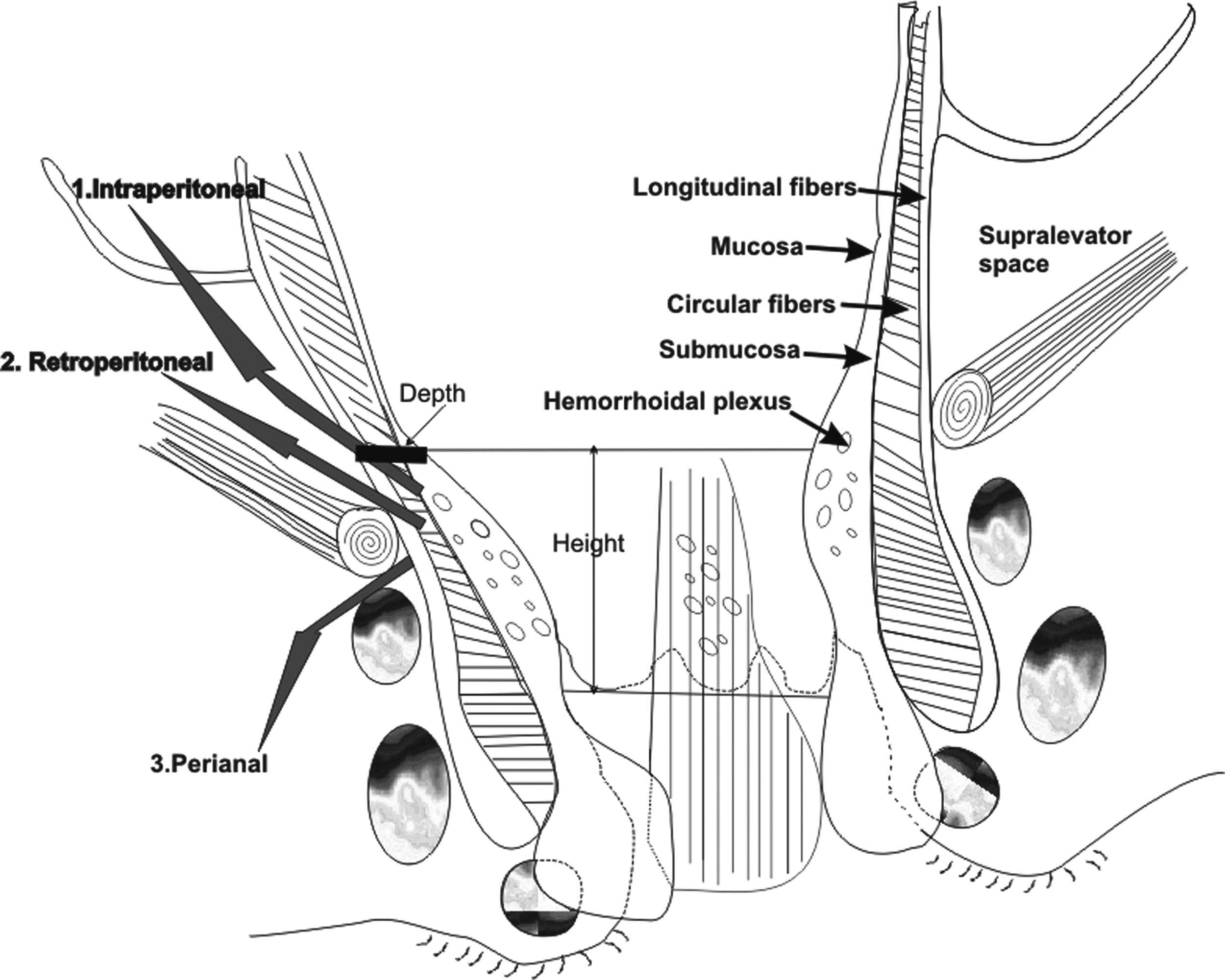
Routes of infectious expansion after injury to rectum from stapled hemorrhoidectomy.
When making the purse-string suture, optimal technique pierces only mucosa and submucosa. This is not always evident. Submucosa, forming a syncytial network of elastic and connective tissue that supports the hemorrhoidal plexus, has not the same mobility in younger as in older patients. Consequently, it is easy to pierce and entrap a part of the underlying muscular layers in young people.
The purse-string suture is placed in a pear- or balloon-like part of the rectum, and it is tied while exerting force on the thread in a plane perpendicular to the plane of its application. Consequently, an irregular portion of the circumferential rectal coat can be incorporated under the head of stapler. Incomplete rings (doughnuts) of excised rectal tissue can signify rectal injury or perforation, which can provoke life-threatening sepsis.
We believe these drawbacks in the application of this method, under certain difficult conditions such as when trying to control severe bleeding, might compromise the integrity of the rectal muscular layers. Any injury to the rectal musculature associated with a hostile microbial colonic environment and microcirculatory instability caused by bleeding could provoke a fulminant local infection. This infection can spread through muscles to three distinct anatomic spaces: (1) Into the peritoneal cavity, causing peritonitis; (2) into the retroperitoneal space [4], causing a difficult-to-drain collection; and (3) into the perianal region, causing an abscess or Fournier gangrene [5] (Fig. 3). The above complications result in potentially serious morbidity, even death, and the surgeon should be aware of all warning signs and symptoms and not hesitate to fashion a temporary colostomy even in a young patient [6,7].
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.