
Abstract
Abstract
Background:
Mediastinitis due to Acinetobacter baumannii is rare.
Methods:
We report a case of mediastinitis caused by pan-resistant A. baumannii in a patient with multiple comorbidities who underwent cardiopulmonary bypass and we also present a literature review.
Results:
Successful treatment consisted of surgical debridement plus drainage, and tigecycline administration for three weeks.
Conclusion:
Surgical source control along with effective antibiotics is essential in the treatment of mediastinitis. Tigecycline has the potential to be an option for pan-resistant A. baumannii mediastinitis.
Introduction
Tigecycline is a semisynthetic glycylcycline approved by the U.S. Food and Drug Administration in June 2005. Tigecycline represents a modified minocycline active against several gram-negative and gram-positive bacteria, including Acinetobacter. In relation to the usefulness of tigecycline in the treatment of A. baumannii nosocomial infections, the clinical data up to now are scarce [3]. In this report, a case of A. baumannii mediastinitis treated successfully with tigecycline in addition to surgical source control is presented.
Case Report
A 58-year-old obese (body mass index: 38.8), diabetic, hypertensive woman with chronic obstructive pulmonary disease underwent two-vessel coronary artery bypass grafting using the left internal mammary artery and saphenous vein via median sternotomy.
Two weeks after coronary artery bypass grafting, the infectious diseases unit was consulted because of fever and retrosternal pain. Her body temperature was 38.6°C, white blood cell count was 14,800 cells/mm3 (80.9% neutrophils), C-reactive protein concentration was 116 mg/L (normal: <5 mg/L), and erythrocyte sedimentation rate was 92 mm/h.
Computed tomography of the chest revealed air in the soft tissues, fluid and air collections in the anterior mediastinum, blurring in fat tissues, and pericardial effusion (Fig. 1). Imipenem-cilastatin and teicoplanin were started empirically.
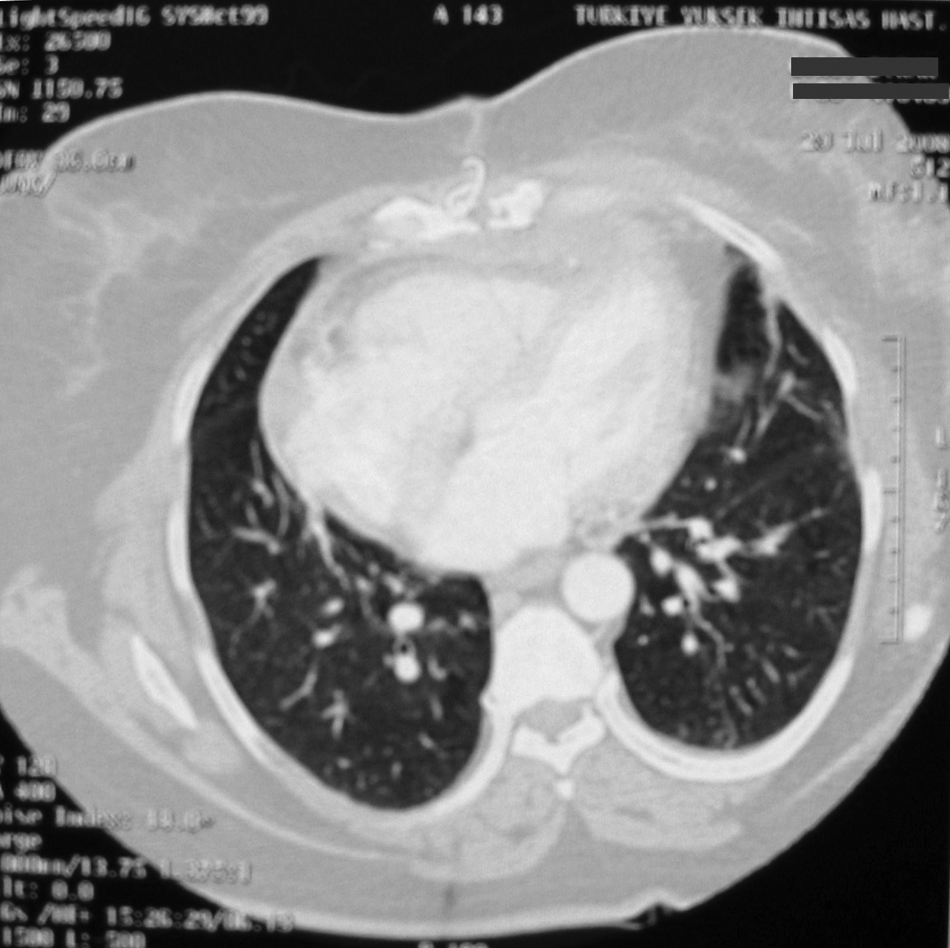
Mediastinal collection with air and fluid, and blurring of fat plane.
The patient was reoperated two days later and surgical debridement, drainage, and sternum fixation were done and drains were left in situ. Wound and pus cultures were taken during the operation.
At the sixth day there was no improvement in the clinical and laboratory condition of the patient. Acinetobacter baumannii was isolated from the culture of pus. It was resistant to all aminoglycosides, fluoroquinolones, β-lactams (including carbapenems), trimethoprim–sulfamethoxazole, and tetracycline, but it was susceptible to colistin and tigecycline. The minimum inhibitory concentration (MIC) of tigecycline was 0.75 mg/L by E-test (AB Biodisk bioMérieux, Marcy l'Etoile, France). Blood cultures were negative.
Imipenem-cilastatin and teicoplanin therapy was switched to tigecycline. A loading dose of 100 mg tigecycline was given intravenously, followed by 50 mg given intravenously two times per day. After 10 days of tigecycline therapy and intensive daily wound care and drainage, the cultures of drainage material became negative. Over the next few days, the wound began to improve, and three weeks after the initiation of tigecycline therapy, both the surgical site infection and the patient's clinical condition had recovered and tigecycline therapy was stopped. No adverse effects were observed during tigecycline therapy except for nausea and vomiting, which occurred during the first two days of therapy and controlled with antiemetics.
The patient was discharged on the forty-sixth postoperative day in excellent physical condition, with a normal hematologic profile and sternal stability.
At follow up four months later, the patient was free of symptoms, C-reactive protein concentration and erythrocyte sedimentation rate were normal, and the surgical site was evaluated with a computed tomography scan, revealing neither air nor fluid collection.
Discussion
Mediastinal surgical site infection has a relatively low incidence in patients undergoing routine cardiopulmonary bypass; it occurs in 1%–3% of patients undergoing median sternotomy. However, the associated mortality rate is as high as 40% [4]. Most mediastinitis cases after cardiac surgery are due to gram-positive cocci such as Staphylococcus aureus and Staphylococcus epidermidis, accounting for 70%–80% of cases. Mixed infections account for ∼40% of cases. Isolated gram-negative and fungal infections are rare [5]. Mediastinitis due to A. baumannii is rare; there are few case reports regarding A. baumannii mediastinitis [6,7].
Nowadays, Acinetobacter has gained great interest owing to the worldwide emergence of multi-drug-resistant (MDR) or even pan-resistant strains that either become endemic or suddenly cause outbreaks of infection [8]. The pooled data suggest that infections by A. baumannii may be associated with considerable attributable mortality [3].
Clinical experience with tigecycline is limited and the U.S. Food and Drug Administration has granted approval only for complicated intraabdominal and complicated skin and skin-structure infections. Tigecycline has shown activity against A. baumannii strains, including imipenem-cilastatin-resistant and MDR strains [8]. Recently, the Tigecycline Evaluation and Surveillance Trial reported in vitro susceptibilities of 63,699 gram-negative isolates, including 9.2% MDR A. baumannii isolates. Although susceptibility breakpoints for tigecycline have not yet been established for A. baumannii, in the Tigecycline Evaluation and Surveillance Trial study tigecycline showed low MIC 90 values against A. baumannii; MIC ranges were found ≤0.008–8 mg/L in MDR A. baumannii [9]. We tested tigecycline susceptibility by the E-test method and found the MIC of tigecycline to be 0.75 mg/L. It has been reported that Acinetobacter isolates with an E-test MIC of 0.5–1 mg/L showed the same MIC by broth microdilution. However, Acinetobacter strains with E-test MICs of 2–4 mg/L were found to be susceptible by microdilution. E-test results showing MICs of ≥2 mg/L should be confirmed with microdilution [10].
Treatment of mediastinitis usually varies from simple, prolonged antibiotic therapy to complete sternectomy combined with plastic surgery. Early recognition and aggressive treatment, including sternal reopening and debridement plus appropriate antibiotic therapy, are crucial for successful treatment of mediastinitis [7]. Source control is one of the most important parts of the treatment of serious infections, drainage eliminates the fluid components of an infection, and debridement discharges the solid components. As a general principle, every established source of infection should be controlled as soon as possible [11]. Our case was treated successfully with surgical debridement and drainage, in addition to three weeks of tigecycline therapy, although the strain exhibited a pan-resistant phenotype. The isolated strain was only susceptible to tigecycline and colistin. We could not use colistin as it is not available commercially in Turkey and tigecycline treatment was the only option for this patient.
In the English literature, we found only one case of A. baumannii mediastinitis treated with tigecycline. In the recently published retrospective study that reports experience with tigecycline for infections caused by MDR A. baumannii and Enterobacteriaceae, 18 patients were included and one patient had primary A. baumannii mediastinitis and secondary bacteremia; that patient was treated with tigecycline and tobramycin in combination. It was reported that the patient died on day eight of therapy because of causes related to this infection [12].
To our knowledge this is the first case of A. baumannii mediastinitis treated with tigecycline successfully. Tigecycline has the potential to be an option for MDR or even pan-resistant pathogens such as A. baumannii. We believe that surgical source control along with effective antibiotics is essential to cure mediastinitis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.