
Abstract
Abstract
Background:
Over the past decade, there has been an increase in both community-acquired and health-care-associated Clostridium difficile colitis secondary to broad-spectrum antibiotic exposure. Toxic megacolon is a rare complication of pseudomembranous colitis that often necessitates emergency colectomy.
Methods:
Review of the pertinent English-language literature.
Results:
We present a case of community-acquired C. difficile colitis that made its initial presentation as fulminant toxic megacolon. Six months after a total colectomy, the patient has no complaints.
Conclusion:
Prompt total colectomy may improve survival in patients with toxic megacolon. The incidence of C. difficile-related toxic megacolon and post-operative outcomes of total colectomy should be investigated in a larger observational study.
Toxic megacolon is a rare, serious complication of C. difficile colitis that often necessitates emergency surgical intervention. It is more common in patients with underlying ulcerative colitis (1%–10%) than in patients with pseudomembranous colitis (0.4–5%) [2–4]. Only 64 cases of C. difficile-associated toxic megacolon have been reported in the literature since 1968 [5–8].
There are few reports on the success rates of surgical treatment of toxic megacolon. Post-colectomy mortality rates in these patients range from 38%–80% [3]. No case reports of “community-acquired” CAD progressing to toxic megacolon have been published in the recent literature. Here, we describe a rare case of community-acquired C. difficile colitis presenting as toxic megacolon that was treated successfully with total colectomy.
Case Report
A 54-year old man presented to the emergency department complaining of cramping and 9/10 abdominal pain with watery diarrhea for the past four days. The patient reported having six loose stools in the past 24 h, followed by nausea, vomiting, and increased thirst. Additionally, he had fever and chills, and a gradually enlarging, distended abdomen was noted. The patient denied hematochezia or mucous in his stool. The patient had finished a ten-day course of clindamycin for treatment of an oral abscess two weeks prior to this episode. This visit to the dentist was the patient's only recent encounter with the health care system. He denied any sick contacts or recent travel. Intensifying abdominal pain had prompted his visit to the emergency department.
The patient's medical history was significant for hepatitis C diagnosed 15 years previously, hepatitis B of unknown duration, and migraines. He had undergone splenectomy more than 20 years ago. The social history included a 30 pack-year history of cigarettes and extensive alcohol use (20 years of abstinence). Additionally, the patient admitted to methamphetamine and heroin use.
On physical examination, he was hypothermic with a temperature 96.0° F and tachycardic at 124 beats/min. His blood pressure was 128/93 mm Hg, the ventilatory rate was 18 breaths/min, and arterial oxygen saturation was 97%. The patient was in no acute distress but appeared pale. The abdomen was diffusely tender and distended with decreased bowel sounds, but there was no evidence of abdominal compartment syndrome. His laboratory values on admission were as follows: Sodium 130 mEq/L, potassium 3.4 mEq/L, chloride 97 mEq/L, bicarbonate 18 mEq/L, blood urea nitrogen 69 mg/dL, and creatinine 2.1 mg/dL. His white blood cell count (WBC) measured 28,200/microliter with bands of 62,000/microliter. Computed tomography (CT) showed severe, diffuse chronic colonic wall thickening, suggesting colitis (Fig. 1).
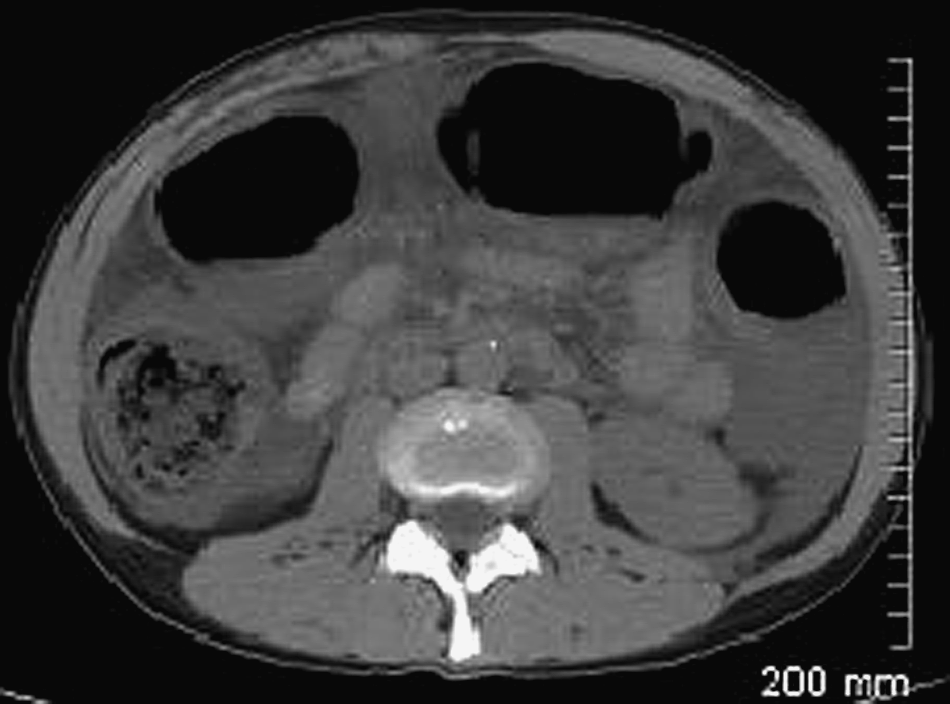
Computed tomography scan showing severe, diffuse chronic colonic wall thickening, suggesting colitis.
On admission, the diagnosis was colitis, but the cause was uncertain. The patient was started on intravenous ciprofloxacin and metronidazole, cholestyramine, pantoprazole, and aggressive fluid resuscitation. When re-evaluated a few hours later, the patient had severe diarrhea, acute kidney injury secondary to volume depletion from diarrhea and sepsis, respiratory failure, and metabolic acidosis; and an emergency surgery consult was arranged. The patient's stool was tested for C. difficile toxins, which were found later.
Within 12 h of admission, the patient was taken to the operating room. He was found to have an acute abdomen with diffuse tenderness with guarding and rebound and thus was scheduled for an emergency exploratory laparotomy.
Approximately 3 L of ascites was found. The colon appeared dilated, measuring 10 cm in diameter, the most-affected segment being the transverse colon. The serosal surface was purple-gray and dusky. There were no signs of perforation. A total abdominal colectomy was performed, and the terminal ileum was used to create an ileostomy. Pathologic microscopic evaluation of the colon confirmed our suspicion of pseudomembranous colitis (Fig. 2).
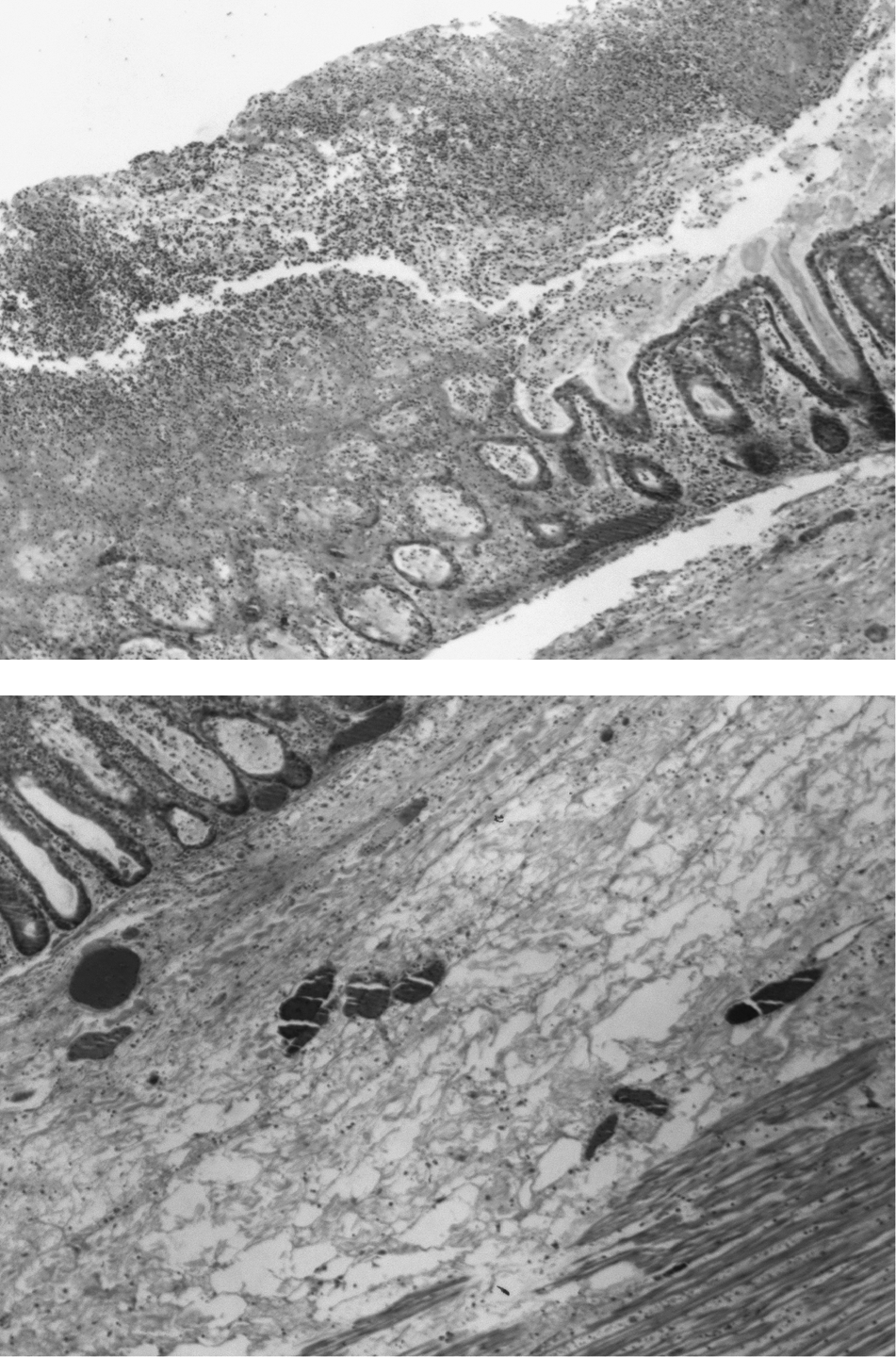
A biopsy of mucosa from transverse colon showing fibrosuppurative pseudomembrane overlying the muscosa and focal areas of necrosis with acute and chronic inflammation. Most of the muscularis propria has degenerated or is completely absent. Hematoxylin & eosin stain; original magnification 20×.
Post-operatively, the patient was admitted to the surgical intensive care unit and placed on vancomycin and metronidazole. Vancomycin was given by rectal enema, 250 mg every 6 h, for 14 days. Oral vancomycin was not given because of the total colectomy. Metronidazole was stopped on post-operative day one. On post-operative day six, the patient's sputum culture grew Chryseobacterium indologenes and Candida albicans, prompting the addition of meropenem for eight days and fluconazole for three days. On post-operative day nine, his status had improved, and he was transferred to the medical/surgical floor. On post-operative day 44, he was discharged from the hospital.
The patient was seen in our outpatient surgery clinic one week later and was free of previous symptoms and recovering well. Subsequently, he had a laparoscopic ileostomy takedown with ileo-rectal anastomosis two months later, which was free of complications. On six-month post-operative visit, the patient continued to report 8 to 10 bowel movements per day, which was reduced with use of loperamide.
Discussion
Toxic megacolon is an unusual, potentially fatal, complication of inflammatory bowel disease, ulcerative colitis, and C. difficile-related disease [3]. Development of CAD is associated with exposure to the bacteria, antibiotic use within the past 6 to 8 weeks, and ineffective host immune response to bacterial toxins [9,10]. Risk factors include age >65 years, immunosuppression, malnutrition, and a long hospital stay [10]. Toxic megacolon associated with CAD has been described as a result of health-care-associated C. difficile colitis. We describe a unique case of community-acquired CAD presenting with toxic megacolon.
Over the past decade, there has been a rise in both community-acquired and health-care-associated C. difficile colitis [11]. Community-acquired CAD occurs by definition within 72 h of admission in patients with no hospitalization within the previous month. The only interaction the above patient had with the health care system was a visit to the dentist two weeks earlier for treatment of a dental abscess. He denied any hospitalizations or visits to hospitals or nursing homes within the last month. The increasing number of community-acquired CAD cases is of interest because patients are at risk for pseudomembranous colitis and subsequent toxic megacolon [12].
Pseudomembranous colitis results from overwhelming C. difficile production of enterotoxin A and B. As enzymes, these toxins glycosylate receptors on enterocytes, leading to loss of cytoskeletal integrity that results in inflammation and fluid release. When the colon wall becomes dilated and friable in toxic megacolon, it is prone to perforation [3,9]. The radiographic definition of toxic megacolon is a transverse colon measuring more than 5.5 cm on a supine abdominal film. However, toxic megacolon is a clinical diagnosis. It often is accompanied by signs of systemic toxicity: temperature >100.4°F, tachycardia >120 beats/min, and leukocytosis [3,7,13]. It can be triggered by an inflammatory reaction, such as immune-mediated ulcerative colitis, or an exogenous toxin, as with C. difficile infection.
Although toxin testing is important clinically, it is hampered by its lack of sensitivity; and a negative toxin assay does not rule out C. difficile as the cause of the clinical picture. Enzyme immunoassay testing for C. difficile toxin A and B is rapid but is less sensitive than the cell cytotoxin assay, and it thus is a suboptimal alternative for diagnosis. Polymerase chain reaction testing is rapid, sensitive, and specific and may be the ideal assay. In addition to presenting signs and symptoms, a pre-operative abdominal CT scan helps confirm toxic megacolon because C. difficile-infected colon often appears thickened, dilated, nodular, edematous, and surrounded by ascites [7,14].
This case demonstrates the importance of increased suspicion for C. difficile-related toxic megacolon in patients presenting to the emergency department with abdominal pain and persistent diarrhea. A clinical picture of fever, profuse watery diarrhea, distended abdomen with diffuse tenderness, and bandemia should alert physicians to an impending surgical emergency. Appropriate fluid resuscitation, antibiotic treatment, and electrolyte restoration should be initiated. A surgical evaluation should be considered early in the workup of such a patient.
In general, management strategies in C. difficile infection should emphasize prevention, with proper isolation of infected patients and hand hygiene for healthcare workers. For infected patients, empiric treatment should be started as soon as possible. Those with a negative toxin assay should be evaluated individually [17]. For mild or moderate infection, those patients with leukocytosis <15,000/microliter and a creatinine concentration <1.5 mg/dL, metronidazole 500 mg orally q 8 h for 10–14 days is recommended. In those patients with severe C. difficile infection, leukocytosis >15,000/microliter and a rising serum creatinine concentration >1.5 mg/dL, vancomycin is recommended at a dose of 125 mg orally q 6 h for 10–14 days. In complicated cases, as in the patient above, with signs of hypotension or shock, ileus, or megacolon, vancomycin 500 mg orally q 6 h in addition to intravenous metronidazole at a dose of 500 mg q 8 h is recommended. If complicated ileus is present, rectal instillation of vancomycin should be considered as a retention enema of 500 mg in 100 mL of normal saline q 6 h [9,17]. Vancomycin is the only medication approved by the Food and Drug Administration for C. difficile infection. However, its use has been discouraged as a first-line medication in order to decrease the selective pressure for emergence of vancomycin-resistant enterococci [17]. If medical treatment fails or toxic megacolon develops, surgical intervention is indicated [9].
Surgical management of C. difficile-related toxic megacolon is controversial, given the limited guidelines available. Early colectomy can be life-saving. Over the last 20 years, there have been conflicting recommendations for total abdominal colectomy (removing all of the colon excluding the rectum), subtotal colectomy (resection of part or all of the colon excluding the sigmoid; although some define it as excluding the rectum), total proctocolectomy (all of the colon including the rectum), or decompressive methods. In a small case series by Koss et al., patients undergoing total abdominal colectomy for fulminant C. difficile colitis had a morality rate of 11.1% compared with patients who underwent left hemicolectomy, who had a 100% mortality rate [14]. Those authors recommended that patients with C. difficile colitis who develop signs of toxicity, peritonitis, or perforation undergo total abdominal colectomy as the operation of choice [14].
In 2005, a retrospective study reported the results of 15 patients who received surgical intervention for toxic megacolon over a ten-year period. Fourteen patients received subtotal colectomy with terminal ileostomy, and one patient received a decompressive cecostomy [13]. Two patients died, a 13% mortality rate. D'Amico et al. concluded that early surgical subtotal colectomy is a valid therapeutic intervention in patients with toxic megacolon. Other approaches have included diverting stoma, decompressive colonoscopy, and segmental resections. However, diverting stoma and segmental colectomies are associated with higher failure rates [2,11,13]. With increasing evidence of lower morbidity and mortality rates, most surgeons currently favor broad resections for urgent cases. The 2010 Society for Healthcare Epidemiology–Infectious Diseases Society of America Guidelines recommend colectomy with preservation of the rectum [17]. In future studies, surgeons should report more specifically how much colon was removed because of the possibility of over-lapping definitions for total and subtotal colectomy.
When a patient presents with signs of sepsis and peritonitis, an emergency surgical consultation is indicated. Patients with a serum lactate concentration >5 mmol/L have a 75% or greater post-operative mortality rate. According to our experience and other reports, early surgical intervention produces the best survival outcomes in these patients. Early clinical suspicion is imperative, because delayed surgical intervention also can increase the risk of perforation, which changes the mortality rate from <5% to 30% [5,7]. The often-quoted dictum to “save the patient, not the colon” was based on a study that reduced the rate of perforation from 32.5% to 11.6% and the mortality rate from 20% to 7% by means of early surgery. The investigators concluded that surgery should be performed shortly after diagnosis [3]. Although reports of successful surgical management of C. difficile-related toxic megacolon are limited, our review of the literature suggests total colectomy as the operation of choice.
In patients undergoing laparotomy for C. difficile-related toxic megacolon, we recommend early total colectomy with ileostomy regardless of whether the colon appears normal externally. Sepsis may persist in patients with residual C. difficile infection in the rectum. For this reason, a course of vancomycin enemas injected into the rectum is recommended. Immune status, age, and pre-operative therapy are factors likely to influence survival. The incidence of community-acquired C. difficile-related toxic megacolon and post-operative outcomes of total colectomy should be investigated in a larger observational study.
Conclusion
This report documents a unique case of community-acquired C. difficile colitis presenting as fulminant toxic megacolon. Toxic megacolon is a rare complication of pseudomembranous colitis that necessitates emergency surgical intervention. There exists a paucity of literature on curative rates of surgical interventions. We were successful with total colectomy and ileostomy.
With the growing incidence of community-acquired CAD, more cases of pseudomembranous colitis and toxic megacolon will present in the future. Although community-acquired cases of toxic megacolon are rare, it is imperative to include the condition as a potential etiology in febrile patients with leukocytosis, diarrhea, and severe colonic distention. A prompt surgical consultation may improve patient survival in these cases.
Author Disclosure Statement
No conflicting financial interests exist.