
Abstract
Abstract
Background:
Superficial surgical site infection (SSI) can be caused by bacterial invasion during surgery. We investigated whether bacteria are found at the wound margin during surgery and whether a wound protector (WP; Alexis® Wound Retractor; Applied Medical, Rancho Santa Margarita, CA) contributes to preventing invasion of the incision margin.
Methods:
We studied 272 patients who underwent gastrointestinal surgery (115 gastric, 157 colorectal, including emergency operations) between October 2005 and July 2007. The WP was used in all operations. After the intra-abdominal procedures were complete, bacterial swabs were taken from the abdominal cavity side of the WP and from the incision margin and used to prepare smears and cultures. After the swabbing, peritoneal lavage was performed using 3,000–5,000 mL of physiologic saline, and, after suture of the fascia, 500–1,000 mL of physiologic saline was used to irrigate the subcutaneous tissue.
Results:
Nine gastric surgery patients and 15 colorectal surgery patients had positive cultures from the abdominal cavity. No patients had positive cultures from the incision margin. Of the 24 patients with positive cultures, three suffered SSIs, all of whom had undergone colorectal surgery. Of the patients who had negative cultures, SSI occurred in only one patient, who had undergone colorectal surgery.
Conclusions:
These results suggest that the WP protects an incision site from bacterial invasion.
Patients and Methods
For 272 patients undergoing gastrointestinal surgery (115 gastric, 157 colorectal, including emergency surgery) between October 2005 and July 2007 at Osaka Minami Medical Center, a WP was used to facilitate exposure of the operative field and to protect the incision site. To perform the laparotomy, the skin incision was made using a scalpel, the subcutaneous tissue was cut using an electrocautery device, and the fascia and peritoneum were cut with scissors.
After the intra-abdominal procedures were complete and before intraperitoneal lavage, swabs were taken from the abdominal cavity side of the WP and from the incision margin (Fig. 1) and used to produce bacterial smears and cultures. After the swabbing was complete, physiologic saline was used to irrigate the intraperitoneal space (3,000 mL for gastric surgery and 5,000 mL for colorectal surgery). After suture of the fascia, the subcutaneous tissue was irrigated with 500–1,000 mL of physiologic saline (the amount of saline was determined by the incision length). The skin was closed by stapling in all cases. For patients undergoing gastric surgery, cefazolin was administered intraoperatively and postoperatively (for one day); and for patients undergoing colorectal surgery, cefmetazole was administered intraoperatively and postoperatively (for three days). The incision was covered with a hydrocolloid dressing for more than 72 h postoperatively. When a bacterial culture was positive, we were contacted by laboratory staff approximately 24 h after the swab was taken. For all patients, but especially when a culture was positive, we maintained close observation of the incision site, performing checks every day. Infections were evaluated according to the criteria of the U.S. Centers for Disease Control and Prevention. Experienced surgeons assessed the incisions postoperatively for SSI.
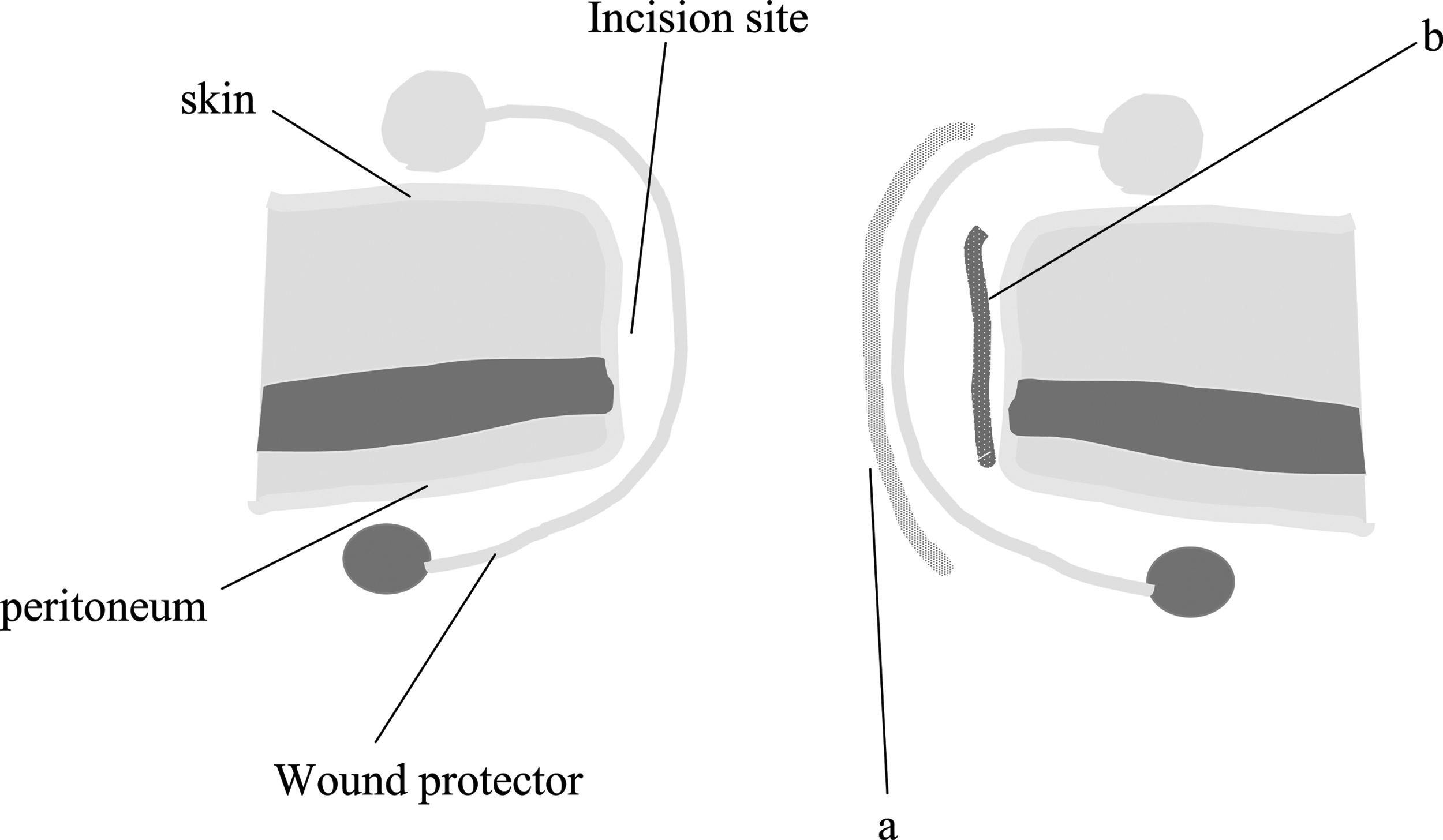
Sites from which bacterial swabs were taken. After the intra-abdominal procedures were complete but before intraperitoneal lavage, swabs were taken from the abdominal cavity side of the wound protector (a) and the incision margin (b) and used for bacterial smears and cultures.
The results were analyzed using Statview 5.0 J (SAS Institute, Cary, NC). The incidence of SSI was analyzed using a chi-square test and the Student t-test, and p < 0.05 was considered to be statistically significant.
Results
Overall evaluation
Twenty-four of the 272 patients had bacteria cultured from the abdominal cavity side of the WP. No bacteria were detected from swabs of the incision margin side. Significantly more positive bacterial cultures were obtained from the abdominal cavity side of the WP than from the incision margin (p < 0.0001).
Of the 24 patients who had positive cultures, superficial SSI occurred in three, all of whom had undergone colorectal surgery. Of the 248 patients who had negative bacterial cultures, superficial SSI occurred in only one patient, who had undergone colorectal surgery. Significantly more patients suffered SSI in the group that had positive bacterial cultures at the abdominal cavity side of the WP than in the group that had negative cultures (p = 0.0033).
Gastric surgery patients
Nine patients who underwent gastric surgery had positive cultures from the abdominal cavity side of the WP. The microorganisms detected were Streptococcus spp. in seven cases, Staphylococcus in one case, and Klebsiella oxytoca in one case. Superficial SSI was not detected in any case, and no patient had positive cultures from the incision margin. The proportion of patients with negative cultures was significantly higher for the incision margin than for the abdominal cavity side of the WP (p < 0.0001).
Colorectal surgery patients
Fifteen patients who underwent colorectal surgery had positive cultures from the abdominal cavity side of the WP. The microorganisms detected were Escherichia coli in six cases, Enterobacter cloacae in two cases, Enterococcus spp. in two cases, and Streptococcus, Staphylococcus, Klebsiella oxytoca, Lactococcus, and a gram-positive bacillus in one case each.
No patients had positive cultures at the incision margin. The proportion of patients with negative cultures was significantly higher for the incision margin than for the abdominal cavity side of the WP (p < 0.0001). Of the 15 patients who had positive cultures, superficial SSI occurred in three. Of the 142 patients who had negative cultures at both sites, superficial SSI occurred in one. The patients who had positive cultures thus had a significantly higher rate of superficial SSI (p = 0.0023). In one case, the bacteria detected in the infected incision were the same as those found on the abdominal cavity side of the WP, but in the other two cases, they were different.
Discussion
Surgical site infection is one of the most frequent complications of colorectal surgery. Risk factors for superficial SSI include high body mass index, low blood pressure during surgery, and severe bleeding during surgery [5,6]. Given that bacterial contamination is the cause of superficial SSI, all surgical procedures should be conducted with a view to minimizing contamination [7]. Our data show that, even if we take care to avoid bacterial infection in the surgical field, the incision margin still is exposed to intestinal bacteria such as E. coli.
In the present study, among patients undergoing gastric surgery, none had a positive culture from the incision margin, but nine patients had positive cultures from the abdominal cavity side of the WP, which demonstrates that the WP protects the incision margin from bacterial invasion. A similar pattern was noted for patients undergoing colorectal surgery, with no positive cultures from the incision margin, but 15 at the abdominal cavity side of the WP.
The incidence of superficial SSI was zero for patients undergoing gastric surgery and 2% for those undergoing colorectal surgery. Given our findings of negative cultures from the incision margin, we consider that the low incidence of SSI may have resulted from the protective effects of the WP.
Irrigation of the subcutaneous tissue is an extremely important measure in preventing superficial SSI. Cervantes et al. reported that irrigation of appendectomy incision margins with 300 mL of physiologic saline delivered by a syringe significantly decreased the likelihood of SSI [8]. Irrigation is believed to remove foreign materials and bacteria from the incision site and contribute to healing, resulting in a lower risk of superficial SSI. Irrigation with antimicrobial solution also reportedly decreases incision infection rates during appendectomies [9].
In the present study, we investigated whether the presence of bacteria at the incision site is related to postoperative SSI. Our data suggest that there is a link between superficial SSI and a positive culture at the abdominal cavity side of the WP. However, in all but one case, the bacteria detected in the infected wound were different from those in the abdominal cavity side of the WP. This can be explained by the fact that many bacterial species exist in the intestinal juices. If one species of bacteria is detected at a site, it is likely that many species actually are present. Therefore, a positive culture at the incision margin is likely to lead to superficial SSI. The results of the present study suggest that the risk of superficial SSI is higher for patients with positive cultures at the abdominal side of the WP than for those without. Thus, for patients with positive cultures, careful postoperative observation of the incision site is necessary.
Conclusion
The WP we used most likely protected the incision margin from bacterial invasion.
Author Disclosure Statement
No conflicting financial interests exist.