
Abstract
Abstract
Objective:
This report presents a case of femoral osteomyelitis secondary to urinary tract infection in a female neonate with bilateral urinary duplication and right ectopic ureterocele.
Methods:
A female neonate with a history of late perinatal sepsis presented to the emergency department and was found to have left distal femoral osteomyelitis. A complex urological malformation was diagnosed (bilateral renal duplication with right ectopic ureterocele associated with nonfunctional superior pole of the ipsilateral kidney). The baby was submitted to prolonged antibiotic therapy and upper pole nephrectomy of the right kidney.
Results:
The pathology report confirmed chronic pyelonephritis and dysplasia in the resected specimen. After 1.5 years the patient is asymptomatic and developing normally, with no apparent deformity, but manifests asymptomatic vesicoureteral reflux.
Conclusions:
Urinary tract infections must always be excluded as the primary infection focus in neonates with sepsis. Perinatal osteomyelitis is almost always a complication of neonatal sepsis and is associated with orthopedic sequelae. This is the first report in literature of a case of osteomyelitis complicating complex urinary duplication and urinary tract infection.
Introduction
For the first time in the literature, to the best of our knowledge, we report a case of a female neonate admitted to be treated for femoral osteomyelitis secondary to an episode of urinary sepsis associated with a complex urinary tract malformation.
Case Report
A one-month-old baby girl was admitted to the Antônio Pedro University Hospital to be treated for left distal femoral osteomyelitis (Fig. 1). The baby had a clinical history of transvaginal term delivery without complications and normal prenatal exams. The baby had been admitted previously to another emergency ward at 17 days to treat a “late perinatal septic episode” with a 10-day intravenous course of gentamicin and ampicillin. Urine evaluations or cultures were not requested at the time.
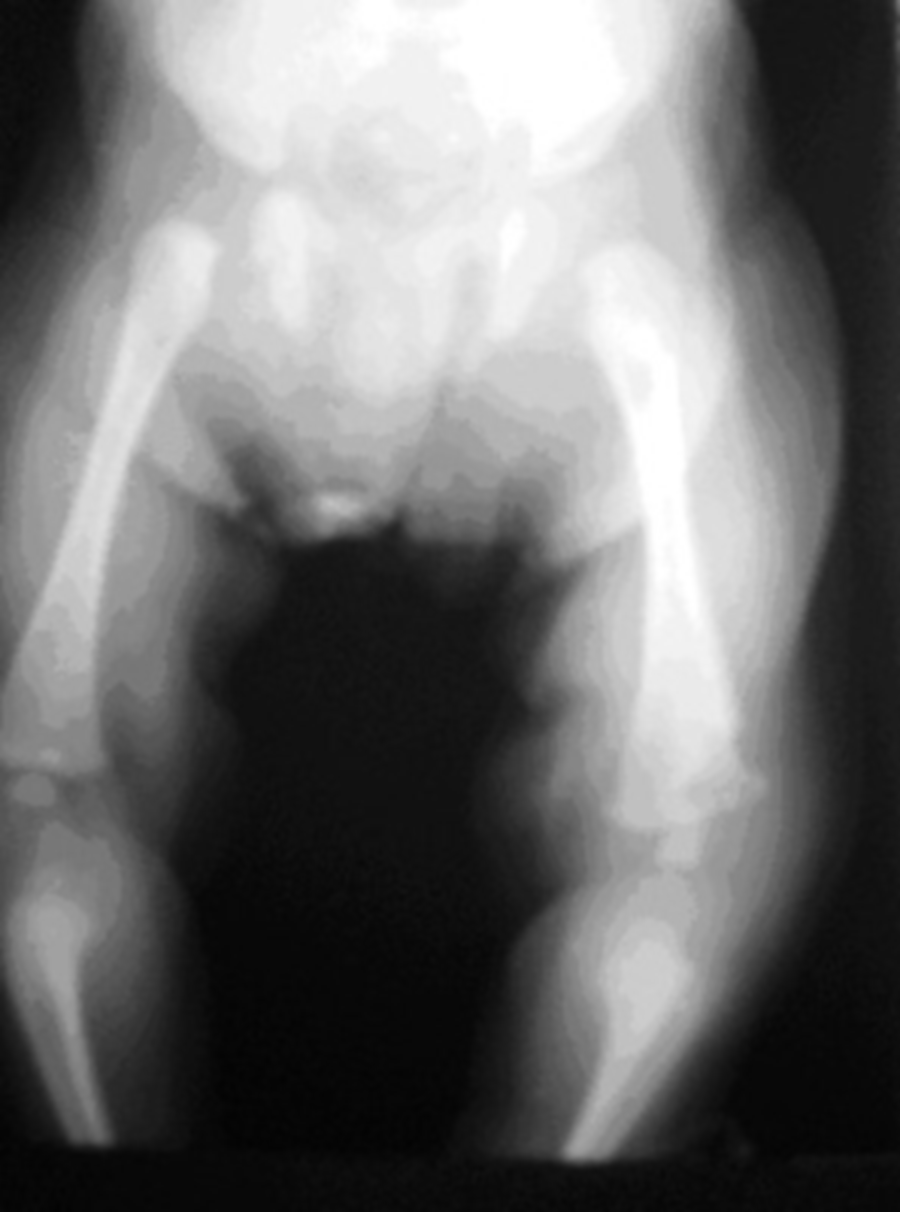
Osteomyelitis: Osteolytic lesion in the inferior femoral extremity.
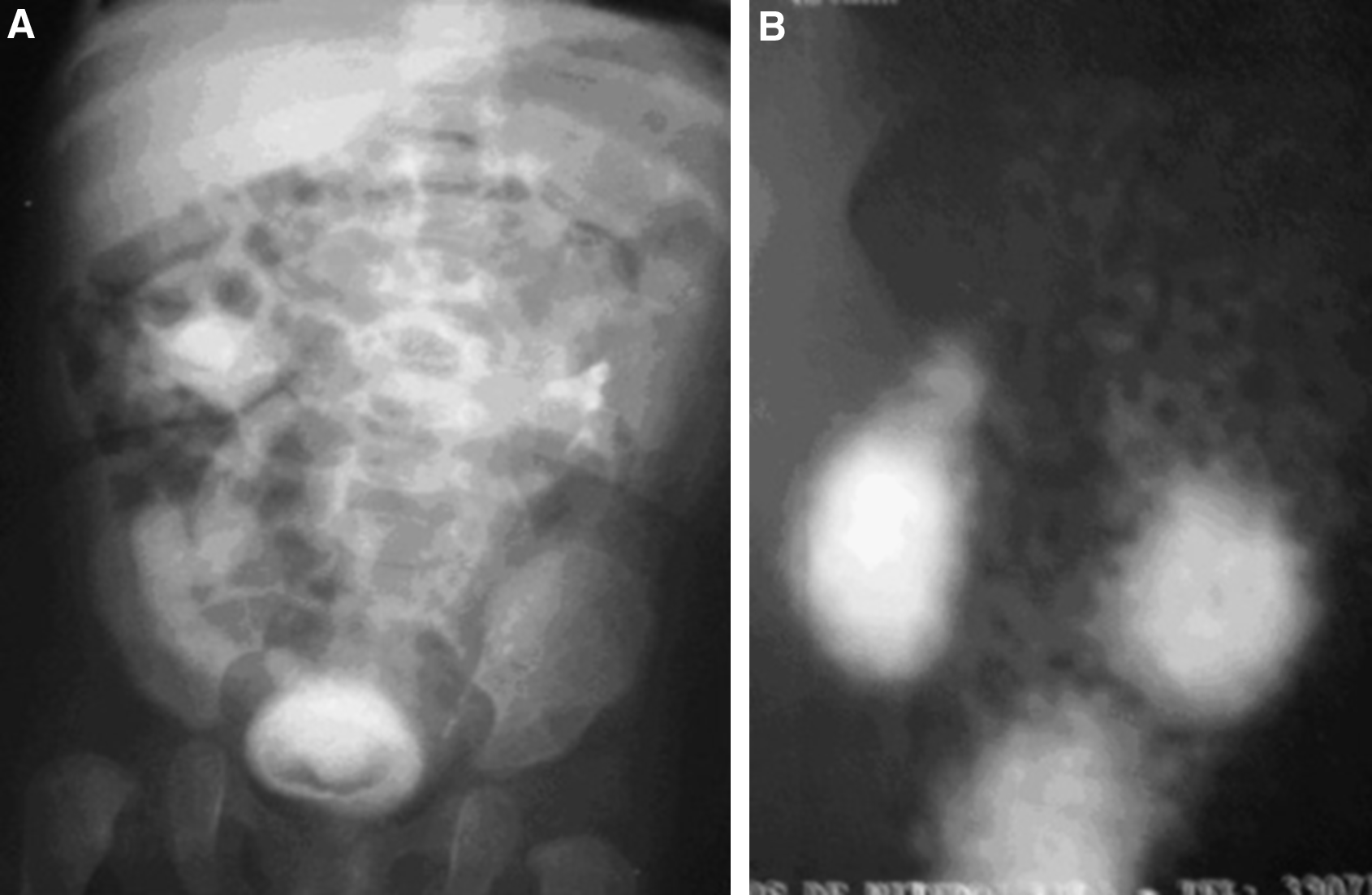
The patient presented with a lytic lesion at the distal femoral metaphysis on the left side, associated with neo-osteogenesis. Osteomyelitis was confirmed and treated with immobilization of the left thigh/leg and parenteral oxacillin + amikacin (21 days), followed by oral cephalexin (21 days). An abdominal ultrasonogram was done to exclude metastatic neuroblastoma, which diagnosed complete bilateral nephroureteral duplication associated with a huge obstructive ectopic ureterocele on the right side. Renal static scintigraphy showed no function of the right upper pole. There was no vesicoureteral reflux, but the right inferior pole was severely hydronephrotic (Fig. 2). Urine cultures and multiple blood cultures were negative, possibly because of the prolonged antibiotic therapy, but the patient manifested pyuria and microscopic hematuria. The patient underwent a right upper pole heminephrectomy at two months of age. The histopathology confirmed chronic pyelonephritis and ureteritis in the specimen, besides hydronephrosis and renal dysplasia with metaplastic cartilage.
(
There were no postoperative problems and the right lower pole hydronephrosis resolved (followup: 1.5 year). The patient now manifests bilateral asymptomatic vesicoureteral reflux to the lower poles. She is being followed up at the orthopedics department, without osseous growth problems presently, and walks normally.
Discussion
Renoureteral duplications occur in ∼10% of the population, but only a small number of them present clinical problems. Associated ureteroceles are proportionally rare, corresponding to a more serious urinary tract malformation. It predominates in girls and the main clinical manifestations are prenatal hydronephrosis and UTI in the first three months of life. The key to postnatal diagnosis is to suspect UTIs complicating urinary tract malformations in “late perinatal sepsis” cases. Symptoms related directly to the urinary tract are rare in young children, but most present high postvoid residual volumes associated with obstructive ectopic ureteroceles and voiding dysfunction [1,2].
Any neonate with sepsis must undergo a urinary culture to investigate the primary focus of infection, as urinary tract malformations are common (∼1% of neonates) and UTIs are a frequent cause of late perinatal sepsis (not done in this case). Late presentations of those patients after multiple episodes care of “unknown cause” of fever are common. Primary practitioners must know that febrile episodes or sepsis in small babies demand exclusion of UTIs and urinary tract malformations [2].
Neonatal osteomyelitis may be a late complication of perinatal sepsis. Subsequent bone growth problems are common because the metaphysis can be affected by the disease [3–6]. The most important differential diagnosis at this age is metastatic neuroblastoma.
In our patient the recognition of a primary urinary infection was fundamental to plan antibiotic therapy, as the bacteria involved in UTI are commonly gram negative, as opposed to staphylococci, which are involved commonly in primary osteomyelitis.
Osteomyelitis and septic arthritis in babies are normally secondary to sepsis, but we could find only one published case of bone and joint infection secondary to UTI in a child, which is a report of right knee septic arthritis secondary to UTI caused by Enterobacter in an 18-day-old baby boy with posterior urethral valves [7]. There is also a paper relating UTI, osteomyelitis, and sickle cell disease in children [8], but in this specific population, osseous infarctions and spontaneous bacteremia are common. In sickle cell patients, approximately three-fourths of the osteomyelitis cases are caused by Salmonella species and not related to urinary tract problems. Bacteremia originating from the urinary tract is commonly caused by Escherichia coli in sickle cell children [9–11]. Tsau et al. reported a case of osteomyelitis in a nephrotic child, but there was no primary UTI [12]. In adults the association of osteomyelitis with UTI is uncommon, but has been reported. The typical patients are elderly people with urinary tract obstructions or immunosuppressed people, and osteomyelitis normally affects the vertebrae [13–21].
Footnotes
Author Disclosure Statement
No competing financial interests exist.