
Abstract
Abstract
Background:
Bacillus species infection of the joints is a very rare occurrence, with sporadic reports in the medical literature.
Case Report:
A 67-year-old woman with osteoarthritis developed infection in the knee joint after arthroscopy. Percutaneous needle aspiration of articular fluid performed post-operatively showed a positive culture for Bacillus species. The diagnosis of septic arthritis was, however, not confirmed as the results were considered contamination. Failure of treatment with beta-lactam antibiotics on two occasions and successful cure of infective arthritis by long-term administration of a fluoroquinolone confirmed iatrogenic clinical joint infection with Bacillus species.
Conclusion:
Any clinically suspected joint infection must be treated as septic arthritis until proved otherwise.
Introduction
Bacillus cereus is a strain associated with infection in open traumatic fractures and is associated with contamination from terrestrial environments [11]. In patients with chronic reactive arthritis, a wide spectrum of bacterial deoxyribonucleic acid is present in the joints, including B. cereus [12]. Bacillus cereus has also been suspected as a secondary etiologic agent in cases of septic arthritis [13]. Septic arthritis due to B. cereus following routine arthrography has been described [14], as well as Bacillus species-related arthritis following hip prosthesis surgery [15]. We report a case of Bacillus species infection in a patient following knee arthroscopy.
Case Report
A 67-year-old woman was followed up as an orthopedic outpatient for several years because of osteoarthritis of both knees. Otherwise she was in good health. Her medical history was unremarkable and she had undergone regular check-ups, including normal gynecological and internistic examinations. As she had developed increasing pain of the right knee, she underwent arthroscopy of that joint; lateral release, abrasion arthroplasty, synovectomy, and meniscal tear repair were performed on June 1, 2009. Five days after arthroscopy, redness, swelling, and pain of the knee was present and correlated to an elevated serum C-reactive protein (CRP) concentration of 18 mg/dL (normal range, 0–0.5 mg/dL). Infective arthritis was suspected and empiric antibiotic therapy was started intravenously (i.v.) with cefuroxime 1.5 g every 8 h. Diagnostic arthrocentesis was performed after two days; microscopically, few leukocytes and red blood cells were identified and gram stain was negative for bacteria; bacterial culture was also negative for growth. Growth of Bacillus species after overnight enrichment was observed and interpreted as contamination. The patient was discharged from the hospital into outpatient care after 4 days and put on oral cefuroxime 500 mg every 12 h. After two weeks of antibiotic treatment (administered initially i.v. during hospitalization and later orally), CRP was repeated because of a lack of clear clinical improvement of the still painful and swollen right knee; CRP had increased further to 29.7 mg/dL. Therefore, cefuroxime was replaced by moxifloxacin 400 mg once daily and was continued for 12 days, when the CRP concentration nearly normalized to 0.68 mg/dL and the knee showed clinical improvement.
The patient presented to the emergency department just four days later with a two-day history of relapsed severe right knee pain, swelling, and redness; and dizziness, lightheadedness, and diaphoresis as a prodrome of neurocardiogenic syncope without loss of consciousness. On examination, the knee was visibly swollen and hot to touch, with a decreased range of movement. Although her white blood cell (WBC) count was normal, erythrocyte sedimentation rate (ESR) was 107 mm/h and CRP was 18.5 mg/dL. A knee aspiration was performed. The gram stain revealed no crystals, moderate WBCs, and no organisms. The patient was admitted and started on a course of ampicillin/sulbactam 3 g i.v. every 8 h.
The patient underwent arthroscopy, which revealed frank pus and marked red pigmentation. Arthroscopic debridement with joint lavage was performed, followed by continuous articular irrigation for five days until culture negativity of synovial fluid was confirmed. During lavage and treatment with ampicillin/sulbactam, CRP after a transient decrease remained essentially unchanged at 18.5 mg/dL, indicating failure of antibiotic treatment. Cultures subsequently identified Bacillus species on enrichment, which was resistant to ampicillin and cefuroxime; however, it was sensitive to moxifloxacin and levofloxacin.
The patient's antibiotics were changed to levofloxacin 500 mg daily, which was given first i.v. for ten days and then orally for another nine weeks until CRP was below 1.0 mg/dL and ESR was normalized. After a 16-day hospital stay, she was discharged and oral antibiotic therapy was continued for three months. Blood cultures were obtained before initiation of therapy with ampicillin/sulbactam and ten days later before antibiotics were changed to levofloxacin. Both were negative for aerobic and anaerobic growth. There was no further identification of the specific Bacillus isolate. During the whole period, her inflammatory markers were monitored closely (Fig. 1). White blood cell count and other routine laboratory parameters remained normal. Since then the patient has been free of infective arthritis.
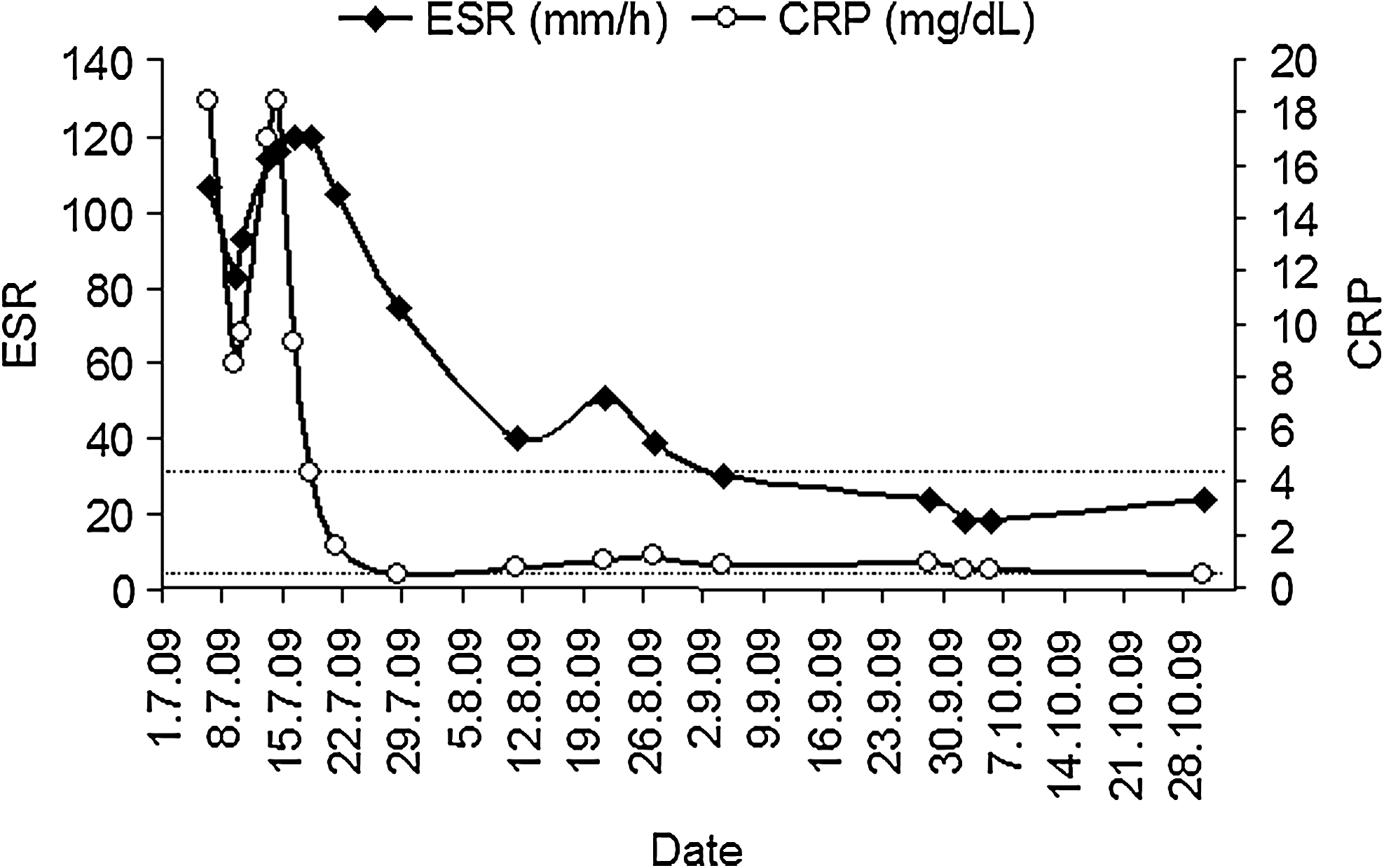
Inflammatory markers at diagnosis and serially during the clinical course of infective arthritis of the knee. Broken lines indicate upper limits of normal range: ESR < 30 mm/h, CRP < 0.5 mg/dL. ESR, erythrocyte sedimentation rate; CRP, C-reactive protein.
Discussion
In recent years, the number of arthroscopies performed has increased greatly as well as the number of joint injections, because of the emergence of intra-articular viscosupplementation therapies. Iatrogenic infection resulting from arthrotomies, arthroscopies, and needle insertions into joints, an increasingly frequent source of septic arthritis, thus, may, also be caused by Bacillus species. In general, the risk of procedure-related septic arthritis has been estimated at 0.5%–2.0% for arthroscopies [16–20] and 0.005%–0.0002% for joint injections [21–23]. According to a recent survey from Iceland, septic arthritis was iatrogenic in 41.8% of adults, and the number of iatrogenic infections increased from 2.8 cases/year between 1990 and 1994 to 9.0 cases/year between 1998 and 2002, with frequencies of post-arthroscopy septic arthritis of 0.14% and postarthrocentesis septic arthritis of 0.037% [24]. Bacillus species were not noted as a causative agent in this study, whereas from among 1,158 cases of microbiologically proven septic arthritis reported from England and Wales over a 4-year period between January 1990 and December 1993, there were three cases with Bacillus species as the causative pathogen (0.026%) [25]. Clinical details of these patients are unknown.
In one study of wound complications following total hip arthroplasty, Bacillus species were isolated from 25% of patients [26]. All patients had received preoperative prophylactic benzylpenicillin, flucloxacillin, cloxacillin, or cefuroxime. Although-half the isolates were susceptible to flucloxacillin and related antibiotics in vitro, these agents did not appear to be effective clinically. In our case, beta-lactam antibiotics were tried empirically on two occasions: Initially, when cefuroxime was administered to the patient because the Bacillus species identified was considered to be a contaminant, and later, when ampicillin/sulbactam was given upon hospitalization after a presyncopal episode. On both occasions, beta-lactam antibiotic therapy proved to be ineffective. Bacillus cereus, unlike nearly all B. anthracis isolates, produces beta-lactamases, so it is resistant to p-lactam antimicrobial agents [27], including third-generation cephalosporins. It is usually susceptible to aminoglycosides, clindamycin, vancomycin, chloramphenicol, erythromycin, and ciprofloxacin [1,28]. Moxifloxacin has been investigated for its use in infectious arthritis following arthroscopy [29] and was also effective in our case.
Fluoroquinolones are possibly promising alternative antibiotics for the treatment of septic arthritis [30]. In a recent Italian survey, ciprofloxacin and levofloxacin were the most frequently utilized oral drugs in the outpatient antibiotic management of bone and joint infections [31]. The patient was treated with moxifloxacin for 12 days after the course of cefuroxime, as the Bacillus isolate was reported to be susceptible to moxifloxacin, which is still not approved for use in septic arthritis but is expected to have efficacy comparable to levofloxacin. The patient improved with this antimicrobial therapy, but the duration of therapy of 12 days may be short for successful treatment of septic arthritis, probably because the formal diagnosis of septic arthritis was delayed.
In accordance with the British Society of Rheumatology-approved guidelines on management of the swollen joint [32], there was a high clinical suspicion of septic arthritis, which was immediately treated with i.v. antibiotics even though the initial gram stain was negative. Joint infection can often yield negative cultures; indeed Bacillus species was identified on enrichment only but was then interpreted as contamination instead of as the causative organism. If the Bacillus species had been recognized as a pathogen in the case of our patient with infective arthritis, a fluoroquinolone might have been administered i.v. sooner with greater effectiveness. Not surprisingly, the patient relapsed soon following termination of oral moxifloxacin. Even though inflammatory markers were used to guide the duration of treatment, oral antibiotic therapy given for less than two weeks should be considered too short for infectious arthritis [32].
On presentation of the patient to the emergency department of our hospital with recurrence, the joint was aspirated prior to antibiotics, appropriate cultures were taken, and ESR and CRP were measured at diagnosis and serially; there was no delay in antibiotic treatment; the initial empiric choice of a penicillin was in keeping with the guidelines as the patient presented no obvious risk factors for atypical organisms [32,33]. However occurrence of arthritis after arthroscopy and failure of two previous treatment courses with a cephalosporin and a fluoroquinolone, respectively, raised doubts about the empiric choice. Results of initial bacterial culture and sensitivity testing focusing on Bacillus species as the causative organism for the infective arthritis of the knee resulted in altered treatment. Persistent improvement of inflammatory markers to levofloxacin of sufficient duration was seen only after antibiotic therapy had been changed for treatment of Bacillus species.
The Standards, Guidelines and Audit Working Group of the British Society of Rheumatology concluded that even if there is little high-quality evidence with respect to the choice or duration of antibiotic therapy in the treatment of causes of septic arthritis other than Neisseria gonorrhoeae, antibiotic therapy should be given i.v. for up to two weeks or until signs improve and then orally for around four weeks [32]. Symptoms, signs, and acute-phase responses are all helpful in guiding the decision to stop antibiotics based on current convention. Also, in Italy, guidelines recommend that antibiotic therapy should be given i.v. for up to two weeks or until signs improve and then orally for at least four weeks, not only after symptoms and signs improved, but also after acute-phase responses have normalized [34]. On the basis of this guideline recommendation, duration of antibiotic therapy for the patient was three months in total after arthroscopy.
In conclusion, potential septic arthritis must be treated with a high index of suspicion, with prompt joint aspiration and administration of antibiotics. Rare pathogens require swift identification and appropriate management. In any elective orthopedic procedure, care must be taken to ensure that there are no iatrogenic infections. The clinical course of the current case strongly suggests that Bacillus species may cause infectious arthritis not only after orthopedic implant surgery but also after arthroscopy.
Footnotes
Author Disclosure Statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.