
Abstract
Abstract
Background:
Advances in technology and in medical knowledge underlie the constant change in paradigms for medical care. Those who understand, anticipate, and plan for these changes will have the greatest impact on future care of patients and education of the next generation of scholars.
Methods:
Review of pertinent literature.
Results:
In hepatobiliary surgery, rapid developments in laparoscopic surgery, image-guided interventions, and minimally invasive ablative therapies have combined to produce much improved care for patients with disease of the liver and biliary tract. Laparoscopic procedures of the gallbladder, bile duct, and liver have altered the morbidity of operations on these organs. Major changes in the treatment of liver abscess, gallstone disease, and liver tumors have resulted from recent changes in technology, highlighting the great opportunities the surgeon anticipating these changes may capitalize on to improve, not only patient care, but the field of surgery.
Conclusions:
Active investigation and developments in education in these areas to improve the training of the next generation of surgeons undoubtedly will improve patient care.
One of my (YF) mentors, Doctor G. Thomas Shires, defined a good academic surgeon as: (1) A good teacher who preaches paradigms of practice based on data; (2) a good researcher who gathers new data to refine practice paradigms; and (3) a good surgeon who learns and uses new knowledge and technology to improve the outcomes of patients. In this article, we summarize the algorithms for treatment of these three diseases and the knowledge gathered over two decades that has driven the evolution to a minimally invasive approach. The most interesting areas of current research are highlighted. The presentation is meant to show the evolution of surgical practice and how surgeons have adopted new technologies to redefine these fields.
Treatment of Liver Abscess
It was only two decades ago that Miedema and Dineen presented their series of surgical treatment of liver abscess at an annual meeting of the American Surgical Association [1]. Until the mid-1980s, surgical exploration with resection or drainage was the standard of care. These procedures carried significant morbidity and high mortality rates, but were the only options that routinely brought about resolution of infections of the liver.
By the beginning of the 1990s, advances in cross-sectional imaging, including computed tomography (CT) and ultrasound scans, combined with the development of pigtail catheters, allowed easy and effective percutaneous drainage of abscesses (Fig. 1) [2–7]. At present, percutaneous drainage has become the standard of care, with surgical intervention relegated to salvage procedures [8].
Abscess in left lobe of liver (
Current practice
Recent data related to percutaneous drainage are summarized in Table 1. Overall, the success rate of drainage, defined as resolution of the abscess, exceeds 60% [2–7]. Many patients (5–20%) need more than one additional drainage procedure. The mortality rate is still high (15–30%)[5,8] because of the cause of such abscesses, including unresolved biliary obstruction, advanced malignant disease, or conditions of immunocompromise [9]. A proportion of patients (20–30%) will require surgical intervention for salvage [5,10]. Predictors of the need for salvage include the size of the abscess, loculations, complex flora, and unrelenting biliary obstruction [5,8]. Some investigators have even advocated primary surgical intervention for large abscesses or those with multiple loculations [11].
Treatment of Cholelithiasis
Treatment of cholelithiasis traditionally has been open cholecystectomy with or without cholangiography or bile duct exploration. In 1986, the first laparoscopic cholecystectomy was reported [12]. Advances in fiberoptic technology and instrumentation allowed for a new approach to removal of the gallbladder and exploration of the common bile duct [13]. In addition, the development of endoscopic retrograde cholangiopancreatography (ERCP) has provided another minimally invasive method for clearing the common bile duct of gallstones. Laparoscopic cholecystectomy has since become the preferred method for treating symptomatic cholelithiasis.
Current practice
Laparoscopic cholecystectomy is the standard of care for treating gallstone disease. Data supporting the evolution to this minimally invasive approach are shown in Table 2. There is no doubt that laparoscopic cholecystectomy is associated with a lower complication rate, a quicker recovery, and a much reduced length of hospital stay [13] compared with traditional open cholecystectomy. However, it also is clear that the incidence of common bile duct injury and stricture is increased greatly [14], the incidence with the laparoscopic approach being on the order of 0.5% [14]. Nevertheless, surgeons and the public have come to accept the tradeoff of this complication as reasonable given the many improvements in outcome.
Calculated using continuity corrections of 1.0.
Statistically significant difference.
Adapted from Keus F, Gooszen HG, Van Laarhoven CJ. Systematic review: Open, small-incision or laparoscopic cholecystectomy for symptomatic cholecystolithiasis. Aliment Pharmacol Ther 2009;29:359–378.
In patients with suspected common bile duct stones, the usual approach has been to perform an ERCP with clearance of the common duct prior to laparoscopic cholecystectomy [15], although centers with expertise in intraoperative laparoscopic common duct exploration may choose this approach [16].
Current research and future directions
Application of evolving laparoscopic technology is being investigated for cholecystectomy. Many investigators are studying the merits of using surgical robots to assist in performing such cholecystectomies [17]. In addition, single-port laparoscopy [18] is being developed whereby through a single multi-channel port, instruments (including curved instruments) can be introduced to resect the gallbladder while decreasing further the number of incisions and the morbidity. Determining whether such approaches are reasonable will require not only clinical outcome analysis but also cost-effectiveness analysis [19].
Finally, there are efforts to use the natural orifice approach (natural orifice transluminal endoscopic surgery, NOTES) to resect the gallbladder. Investigators are performing transgastric cholecystectomies [20], and there are reports of use of a transvaginal approach [21]. Although this operation is technically feasible, deciding whether the better cosmetic results justify the higher risk of opening these organs and the reduced visibility and exposure will require rigorous investigation.
Treatment of Liver Tumors
For decades, the treatment of choice for malignant liver tumors was surgical resection. For primary hepatocellular carcinoma (HCC) [22–27] or metastatic colorectal cancer [28–33], surgical resection provided a 40% chance of five-year survival and a 20% chance of cure (Table 3)[34]. The mortality rate was low except in patients with baseline liver dysfunction, such as hepatitis, fibrosis, or cirrhosis [23,24]. In patients with normal liver parenchyma, resections of as much as 75% of the liver were associated with a less than 3% mortality rate [26,27]. In general, surgeons restricted resections in patients with cirrhosis to two or fewer functional segments of liver, and yet the mortality rate was reported to be 5–10% [23]. The morbidity was high for all patients, with 30–50% suffering complications, hospital stays of 7–9 days being routine, and recovery to baseline generally taking on the order of two months. The morbidity and recovery was accepted when resection was the only potentially curative option for these diseases.
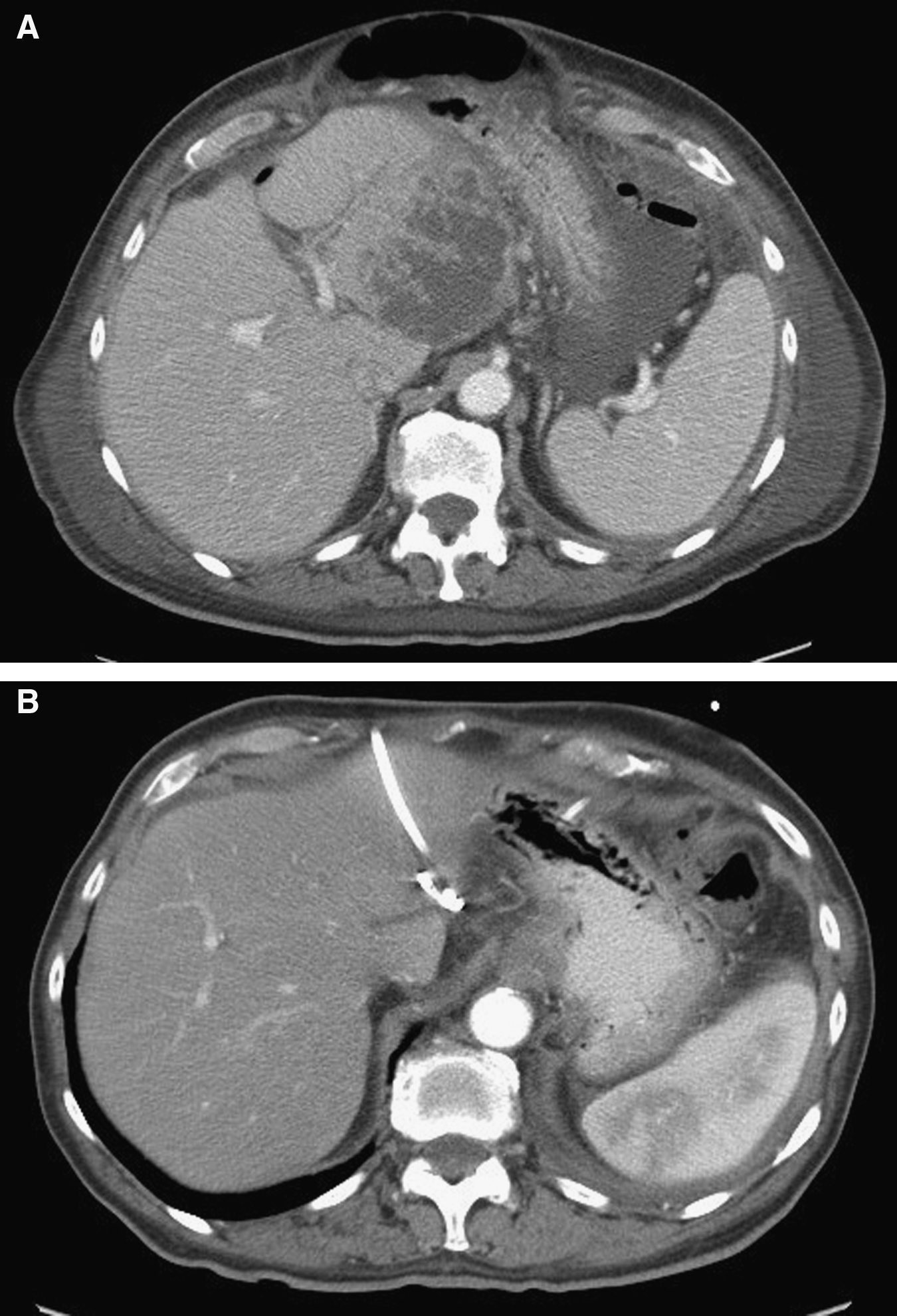
Over the last decade, developments in technology have provided radiofrequency ablation (RFA) units that are affordable, minimally invasive, and effective in killing liver cancers. Conceptually, RFA involves placing a needle electrode into a neoplasm to deliver electrical energy in the range of 300–500 kHz, which results in local ionic agitation and generation of heat. If the local temperature reaches 60°C, there is instantaneous death of tissues, whereas a temperature of 50–60°C will cause tissue death within 5 min [35]. The appearance of one such needle in a tumor as imaged by CT scanning is shown in Figure 2. These needles can be placed under visual, ultrasound, CT, or magnetic resonance imaging (MRI) guidance. The procedure also can be performed during open surgery, particularly in conjunction with resections of tumor, as well as by laparoscopy or percutaneously.

Radiofrequency probe guided by CT scan to target (recurrent metastatic disease in right hepatic lobe).
The results of RFA are accumulating (Tables 4 and 5), and it is clear that these procedures are quite safe. In a collected series of 3,554 percutaneous ablations in 2,320 patients, the mortality rate was reported to be 0.3%, with a major complication rate of 2.2% [36]. The local tumor control rate is highly variable, depending on technique and patient selection (tumor size and location) [37]. It is clear that open surgical ablation has a better success rate [38], but at the cost of higher morbidity. Small tumors far from major vasculature are the best lesions to be treated, the results showing the best durability. In general, a tumor < 3 cm, away from major vasculature, has a 90% likelihood of being ablated completely [37].
NA = not available.
Perc = percutaneous; NR = not reported; Surg = open surgery.
Current practice
Although the field is still in flux, it is clear that use of RFA is on the rise. There are some clinical scenarios in which RFA is becoming the preferred treatment:
In patients with recurrent hepatic tumors after resection, RFA often is the initial local therapy. This choice is understandable because adhesions make the morbidity of repeat resection a concern. Prior resections, particularly major resections, also technically limit the resectional options for recurrences. In particular, for primary HCC, there are data demonstrating the advantage of ablative therapy for small recurrences. In a comparative trial of resection and RFA for small recurrent HCC, the complication rates were 6% (RFA) and 68% (resection), and the five-year survival rate was 40% (RFA) vs. 28% (resection) [39]. In metastatic colorectal cancer, such comparative data are being collected by a number of groups.
The concept that resection can be combined with ablation was first suggested by Rivoire et al., who described a 36% four-year survival rate after combination resection and cryoablation for malignant liver tumors [40]. Rivoire et al. suggested that some patients with disease not completely resectable can be rendered disease-free and potentially become long-term survivors. A subsequent study examined 101 patients subjected to combined resection and RFA, and found 41% three-year and 20% five-year survival rates [33]. These are inferior to the results of resection alone because the patients eligible for such combined therapy were those with disease that was not completely resectable. The results are nevertheless much better than treatment by chemotherapy only (no five-year survivors), and suggest that some patients previously relegated to palliation only do have the potential for cure. Ongoing studies are examining results in patients with completely resectable disease, where combined resection and ablation are being used to try to minimize morbidity and mortality rates.
In primary HCC, dysfunctional parenchyma increases the risk of liver resection manifold. Thus, even for completely resectable disease, investigators have been looking for less-invasive alternatives that may produce durable results. Large single-treatment series demonstrate the usefulness of RFA as a replacement for resection for small HCC. Livraghi et al. reported a series of 374 treatments of HCC by RFA [41]. In patients with solitary tumors, or three tumors each <3 cm, the three- and five-year survival rates were 69% and 43%, respectively. These results rival the outcomes of resection or transplantation. In a recent trial, investigators randomized 180 patients to either resection or ablation. The mortality rate of the therapies was 0 vs. 1.1%, whereas the morbidity was significantly different (4% vs. 55%; p = 0.0001) [42]. The five-year survival rate was no different (68% vs. 64%). Other reports corroborate these results (Table 4) [43–51]. Thus, it appears that for small HCCs, RFA may prove to be equivalent in outcome to resection, at much lower morbidity.
For metastatic colorectal cancer, the data are less clear because no good randomized trial has been performed. In the past, only those patients deemed not to be candidates for resection have been included in trials of RFA (Table 5) [52–64]. Thus, the overall survival rate generally is much lower than that for resection. Nevertheless, it is clear that appropriate use of a minimally invasive approach is indicated, particularly in patients with major co-morbidities that preclude resection.
Current research
Technologic studies of better methods of guidance for placement of probes such as virtual reality, robotics, or biologic scans are likely to improve targeting of lesions. Studies of methods for monitoring the completeness of tumor ablation, such as MR spectroscopy or MR thermography [65], also are likely to improve the effectiveness of these therapies.
Awaited are important studies examining the usefulness of RFA in common clinical scenarios, examining both efficacy and cost-effectiveness endpoints. There also are plans for national studies to examine the value of these low-morbidity local therapies as cytoreductive treatment for predominant liver disease in patients with minimal systemic spread.
Challenge to Surgery and Surgical Training
With the development of various minimally invasive therapies, a number of challenges will be posed to the academic surgical oncologist. First and foremost is how to train individuals to perform these procedures with competence. It is imperative that those pioneering these procedures mentor surgeons new to ablative therapies.
Because these minimally invasive procedures are being performed on less complex cases, it is the more complex cases that will require traditional surgery. The most inflamed gallbladders, the largest tumors lying in proximity to the vena cava, and multi-loculated abscesses adherent to the diaphragm are examples of cases that will make up a larger percentage of the workload of surgeons performing open surgery. If all simple cases are to be managed by minimally invasive alternatives, how do we ensure adequate training for surgeons asked to perform open surgery on the most complex cases? This will be a challenge that will necessitate intensive advanced training as well as surgical simulators to overcome.
We also will need to perform well-designed trials to define the clinical role of these new therapies. The most difficult part will not be deciding on trial design, but rather recruiting patients. We as guardians of the traditional therapies should be open-minded enough regarding new therapies to participate in these trials. Only with dialogue between inventors of new techniques and surgeons performing traditional therapies can adequate trials be performed and the results evaluated with all viewpoints and biases taken into account for the benefit of future patients. Once a new therapy is established, training programs to grow the next generation of practitioners, as well as credentialing criteria, will need to be established.
Conclusion
Minimally invasive surgical approaches are being perfected to treat safely and with low morbidity many of the simpler clinical lesions encountered by surgeons. A role for traditional open surgery always will exist, but will be increasingly demanding from a technical standpoint. As such evolution occurs, those surgical leaders paving the way will need to conduct research to establish new paradigms in treatment, restructure surgical training to encourage dissemination of new techniques, and ensure that surgeons continue to be competent in traditional surgical therapies.
Author Disclosure Statement
No conflicting financial interests exist.