
Abstract
Abstract
Background:
Calcific myonecrosis is a rare late complication of trauma, affecting almost exclusively the lower limb. Its radiologic appearance is characteristic. Superimposed infection usually is a sequela of biopsy.
Case Report:
We present three patients, one with bilateral involvement, who presented with calcific myonecrosis and spontaneous infection. Three infections were attributable to a single microorganism: Enterobacter cloacae, Staphylococcus hominis, and S. haemolyticus were recovered. Multiple microorganisms were responsible in the other case. Treatment consisted of radical surgical debridement and antibiotics. The incision was closed over a suction drain, where possible, or left open to close by secondary intention.
Conclusions:
Calcific myonecrosis may present as infection without any obvious precipitating factor, and it should be included in the differential diagnosis in cases of soft tissue infection of the leg.
We present three patients, one with bilateral involvement, who presented with de novo superimposed infection not related to any surgical intervention.
Case Reports
Patient 1
A 54-year-old male was admitted to our department with swelling, redness, and warmth of the anterior compartment of his right leg for the last ten days with a soft and fluctuant mass. The patient was afebrile. He had been in a railway accident seven years before, when he had suffered a crush injury of both legs. His medical history was otherwise unremarkable. No neurologic deficit was noticed.
Radiographs showed a large fusiform calcified mass involving the anterior and lateral compartments of both legs (Fig. 1). A computed tomography (CT) scan of the right leg showed that the mass had a cystic lobulated component with peripheral calcification of the musculature and affected the deep posterior compartment as well. A triplex examination of both lower limbs was normal.

Radiographs of right (
Surgical exploration of the right leg revealed paste-like material and granulation tissue. After thorough debridement, the incision was closed over a suction drain. Cultures of the wound were positive for Enterobacter cloacae. The patient was started on intravenous ciprofloxacin for two weeks and then oral ciprofloxacin for another four weeks. The incision site healed uneventfully.
Four years after the first admission, the patient presented with similar symptoms and signs in the left leg. The wound was debrided and closed over a suction drain. Cultures grew Staphylococcus hominis. He was treated with amoxicillin-clavulanic acid, intravenously for ten days and orally for three weeks. The site healed uneventfully, and five years after the last admission, there are no signs of infection in either leg.
Patient 2
A 66-year-old male presented with a one-month history of painful swelling and redness over the anterior compartment of his left leg. A draining sinus had developed distally in the previous ten days (Fig. 2). The patient's temperature was 38°C. He had a history of a road traffic accident with injury to the popliteal artery 52 years before. Three toes had been amputated. He was suffering from coronary disease and had an artificial heart valve. He was receiving anticoagulants. On examination, the leg was atrophic with a stiff ankle, no peripheral pulses, and sensory loss in the area of the peroneal nerve. Radiographs and a CT scan of the leg (Fig. 3) showed extensive calcification of the anterior and lateral compartment with features similar to the previous case.

Clinical appearance of left leg of patient 2 on admission.
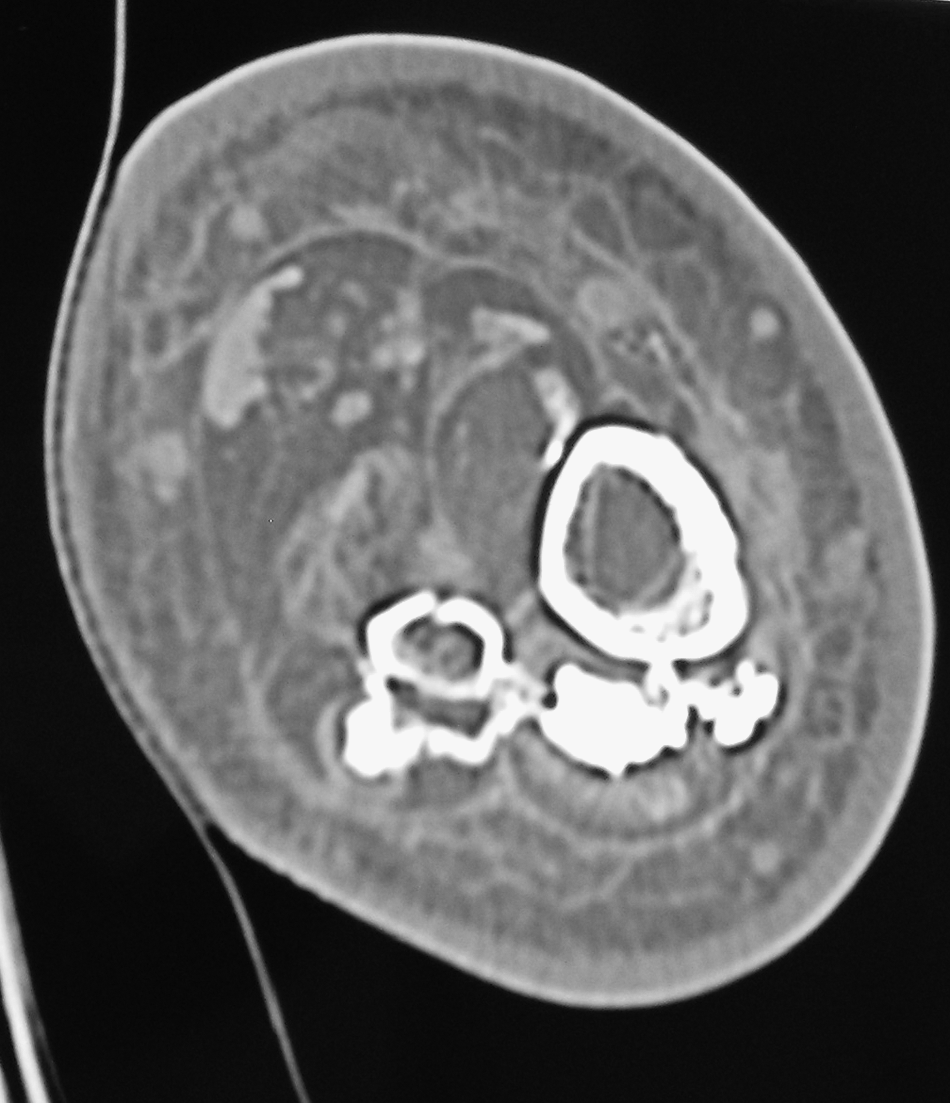
Computed tomography scan of left leg of patient 2. Calcifications of anterior and lateral compartments can be seen.
Cultures from the sinus grew Enterobacter cloacae, Klebsiella pneumoniae, and Enterococcus faecalis. The patient was admitted for intravenous antibiotics (piperacillin-tazobactam for six weeks and gentamicin for ten days) and extensive surgical debridement of the anterior and lateral compartments of the leg. After three operations, in which calcifications and inflamed fibrous tissue were excised, the entire anterior compartment was removed. The incision was left open to heal by secondary intention. A vacuum device was used to accelerate healing. While the site was open, cultures grew multi-resistant Klebsiella spp., Acinetobacter baumannii, and penicillin-resistant Staphylococcus aureus, which were treated with colimycin and linezolid for three and four weeks, respectively. The wound healed over a period of six months. Two years after healing, no recurrence had been reported.
Patient 3
An 84-year-old female presented with soft tissue infection of her right leg and a temperature of 38.3°C. The patient had sustained an injury 53 years before her admission: A tree branch caused “excessive bleeding” from her right leg. She also had been treated for infection of her leg 31, 30, and five years before. The patient was suffering also from hypertension, aortic insufficiency, and pulmonary hypertension. Radiographs showed a fusiform calcified mass in the anterior and lateral compartments of the leg. A magnetic resonance imaging (MRI) scan showed that the deep posterior compartment was involved (Fig. 4).
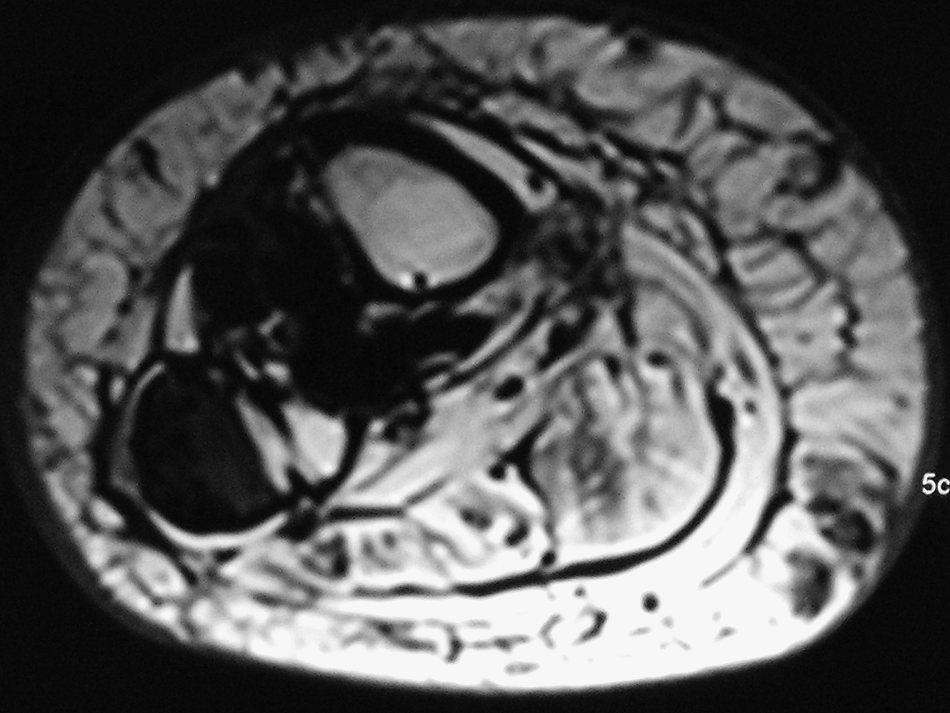
Magnetic resonance imaging scan of right leg of patient 3. Calcifications of anterior, lateral, and deep posterior compartments are visible.
The wound was debrided, and, after removal of calcifications and granulation tissue, it was left open to heal by secondary intention. Cultures from the wound grew S. haemolyticus. The patient was treated with ciprofloxacin and clindamycin, intravenously for four weeks and then orally for another four weeks. The wound healed over a period of two months. One year later, there were no signs of infection.
Discussion
Calcific myonecrosis affects the lower limb typically, although a single case involving the upper extremity has been described [2]. Previous trauma has been reported in all cases, predominantly tibial or femoral fracture, blunt trauma, crush injury, knee ligament injury, and gunshot wound. A nerve injury, particularly of the peroneal nerve, also has been related to calcific myonecrosis. It seems that in most cases, the common denominator is the compartment syndrome, sometimes sub-clinical [3, 4]. The syndrome results in poor circulation, necrosis, and fibrosis with eventual calcification of fibrous tissue that surrounds the liquifaction and hematoma [5]. Over time, repeated intralesional hemorrhage causes the mass to enlarge and calcify [6]. It commonly presents as a slowly enlarging, usually painful, mass several decades (as long as 64 years) after the injury. The anterior compartment of the leg is the most frequently affected site followed by the lateral and the deep posterior compartments [3].
Radiographs reveal a fusiform mass with peripherally oriented plaque- and plate-like calcifications that may present within a whole muscle or compartment [6]. These calcifications are differentiated from those of myositis ossificans by the absence of an intralesional trabecular pattern and marrow signal on MRI [5]. Smooth erosions with minimal periosteal reaction may be seen in the adjacent bones [3]. A CT scan often shows a cystic lobulated component and more evident compartmental involvement [3]. On MRI, the lesions appear heterogeneous on both T1- and T2-weighted images with some areas of hyperintensity on the latter reflecting the cystic change. The outer rim shows low signal intensity resulting from the calcification and fibrosis [7,8]. Sonographic imaging also may be useful [9].
The most important differential diagnosis is between calcific myonecrosis and sarcomas (synovial, epithelioid, parosteal; soft tissue osteosarcoma). Calcific myonecrosis has peripheral calcification and central liquefaction [3,8,10]. In contrast, in soft tissue sarcomas, the mineralization tends to be distributed throughout the tumor. In addition, the majority of synovial sarcomas arise within 5 cm of a joint. Although soft-tissue sarcomas may be largely necrotic, some degree of enhancement usually is evident on gadolinium-enhanced MRI. Contrast enhancement is lacking in calcific myonecrosis [6,7]. However, in rare cases, calcific myonecosis may cause significant bone erosion, making differential diagnosis more difficult [4]. Myositis ossificans can be distinguished from calcific myonecrosis by the relatively short history (weeks or months after injury), the absence of expansion of the lesions, and maturation with bone forming first on the periphery [7]. Dermatomyositis, polymyositis, and diabetic myonecrosis may result in extensive calcification, but the systemic manifestations are evident, and there is no history of trauma. Tumoral calcinosis may be idiopathic in certain parts of the world, but it usually is associated with chronic renal failure and is located periarticularly [3,7]. Chronic expanding hematoma has similarities to calcifying myonecrosis in terms of history and pathology. Dystrophic calcification may occur in this rare condition, although it usually is not so extensive. Some authors consider chronic expanding hematoma and calcific myonecrosis part of a spectrum of the same condition [11].
Calcific myonecrosis is often complicated by infection, usually as a result of a surgical procedure. Ten cases of chronic discharging sinus have been reported after biopsy [3]; one of them ended in above-knee amputation [12]. However, there are only two reports in the literature of de novo infection. Snyder et al. [13] reported an infection attributable to S. epidermidis and S. haemolyticus after minor trauma. Holobinko et al. [5] described two cases: One diabetic patient developed infection caused by Pseudomonas aeruginosa without any injury; the other patient suffered from calcific myonecrosis of the foot and developed infection by S. aureus, which probably entered the calcified area through a broken-down callus. In our cases, as well as in those of Holobinko et al. [5], the infection probably was hematogenous, and in our patients, there was no systemic predisposing factor. Various gram-positive and gram-negative microorganisms may cause the infection. If the incision is left open, there is risk of superimposed infection by nosocomial multiresistant strains. There also is a risk of recurrence of the infection (our patient 3 and case 2 of Holobinko et al.).
With regard to treatment, calcific myonecrosis is a benign entity, and once the diagnosis has been established clinically and radiologically, it should be considered a “don't-touch” lesion [3,5,8,14] because of the high risk of infection. O'Keefe et al. [6] described a case of cardiac arrest at the conclusion of an intralesional excision and related this event to substantial blood loss and exposure of a large area of vascularized cyst wall with possible release of cytokines and necrotic debris into the circulation. If the lesion is symptomatic, complete surgical debridement combined with flap coverage, primary closure over a suction drain, or healing by secondary intention is recommended [5]. If a biopsy is regarded as necessary, it should be performed only if radical debridement is contemplated [3].
In case of infection, which often is combined with poor circulation, early flap coverage may not be feasible, and if the debridement is extensive, healing by secondary intention may be the only solution. However, there is a risk of superimposed infection. Antibiotic treatment should be started immediately after harvest of specimens for culture, and a combination of antibiotics covering gram-positive (including staphylococci) and gram-negative microorganisms should be used until the microbiology results are available. Taking into account the poor circulation of the limb and the necrotic and fibrotic tissue in the lesion, a long period of antibiotic treatment seems necessary. In the literature, six to eight weeks (with a minimum of two weeks of intravenous administration) have been reported [5,10,13].
Calcific myonecrosis is a rare post-traumatic condition that may be missed [5]. It may present as infection without any obvious precipitating factor, and it should be included in differential diagnosis in cases of soft-tissue infection of the leg. In case of confirmed calcific myonecrosis, the patient and the physician should know that if conservative treatment is chosen, spontaneous infection is a possible complication. Radical surgical debridement and proper antibiotic administration are the keystones of treatment.
Footnotes
Author Disclosure Statement
There is no conflict of interest.