
Abstract

To the Editor:
Intracranial suppurative complications from chronic otitis media are becoming fewer; however, they still represent a challenge for early recognition, adequate treatment, and satisfactory results. Staphylococcus xylosus is a commensal bacterium generally found inhabiting the skin and the mucous membranes of mammals [1]. This species is recognized as a nonpathogenic Staphylococcus spp. and has rarely been reported associated with infection in humans [2,3]. We report here a case of otogenic brain abscess caused by S. xylosus in an adolescent. To our knowledge, this is the first case of S. xylosus central nervous system (CNS) infection to be reported in the literature.
A 17-year-old girl was admitted to our department with complaints of headache and vomiting for 2 days. She was known to have left chronic otitis media since childhood without history of any congenital or acquired immune deficiency. Two weeks before presentation, an otolaryngologist diagnosed a left acute otitis media. Amoxicillin-clavulanic acid was prescribed.
At admission, the patient was alert and oriented. Vital signs were normal and the patient was afebrile. She had meningismus with no other accompanying abnormal neurological findings. Otoscopic examination of ears revealed the exudation of fresh pus from the left ear. Bacterial meningitis was then suspected.
The leucocyte count was 17.8 × 109/L with 78% neutrophils and 19% lymphocytes. Erythrocyte sedimentation rate was 36 mm and the C-reactive protein concentration was 12 mg/L. A contrast-enhanced computed tomography scan showed a hypodense area with ring enhancement in the left temporal lobe and ventricular mass effect (Fig. 1). There were also signs of otitis media and mastoiditis on the left side (Fig. 2). Left temporal emergency burr hole operation was performed, and 36 mL of thick green pus was aspirated and sent for bacterial culture. Thereafter, the cavity was irrigated, wound drainage was performed, and parenteral antibiotics (cefotaxime, gentamicin, and metronidazole) were administered. Culture of the pus aspirate from left ear and brain abscess revealed pure growth of S. xylosus by API 20 staph (BioMérieux, Marcy, l'Étoile, France). In a standard antimicrobial disk-diffusion test, both isolates were susceptible to oxacillin, erythromycin, gentamicin, ciprofloxacin, kanamycin, fosfomycin, trimethoprim-sulfamethoxazole, tetracycline, and vancomycin, and resistant to lincomycin, fusidic acid, ampicillin, and penicillin G. In addition, both isolates exhibit low-level resistance to nalidixic acid with a positive CAMP test (a test to identify Group B β-streptococci). Genotypic methods were not used.

Preoperative computed tomography scan after contrast injection showing a large rim-enhancing temporal abscess (star) with an important mass effect.
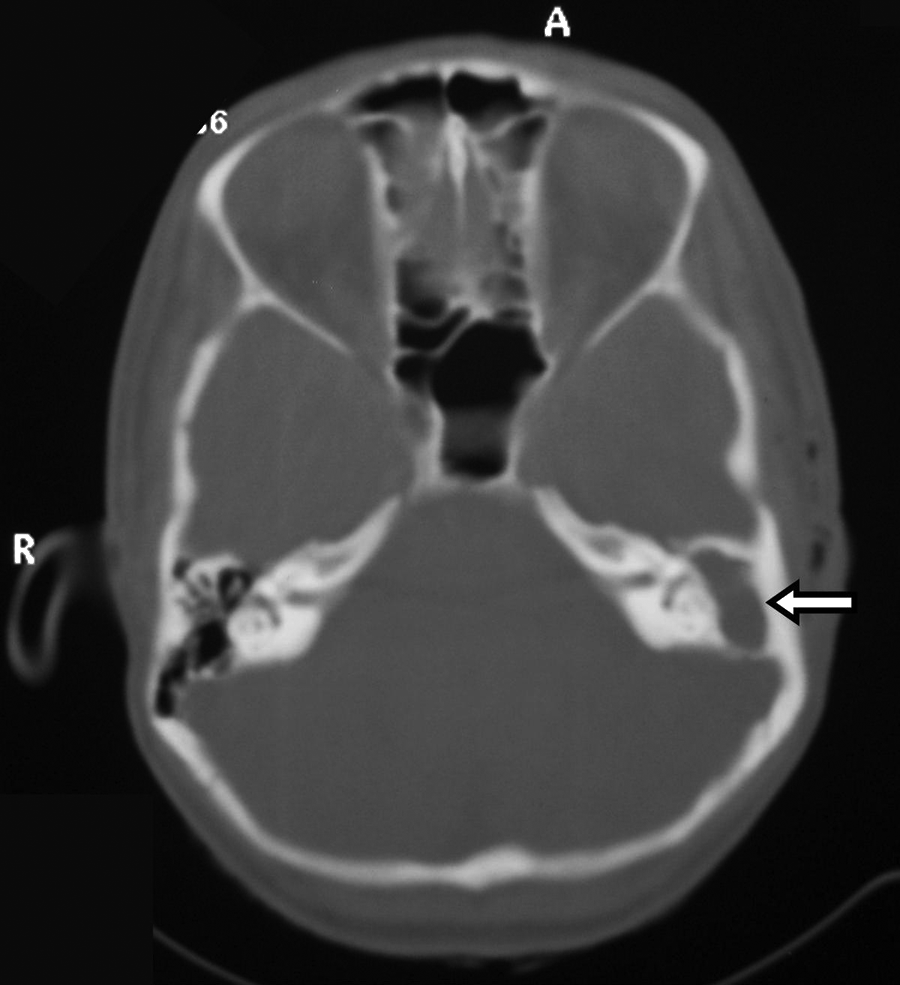
Computed tomography scan, bone window, demonstrating signs of otitis media and mastoiditis on the left side (arrow).
The patient was treated with gentamicin (160 mg/day for 10 days) and cefotaxime (1 × 3 g/day) for four weeks followed by ciprofloxacin orally (1 g/day) for one month. A mastoidectomy was performed one month after her admission. One month later she was discharged in good clinical condition without any neurological deficit. (Supplemental Fig. S1 may be viewed online at www.liebertonline.com/sur)
Staphylococcus xylosus is a gram-positive, catalase-positive, coagulase-negative, facultatively anaerobic, nonmotile, nonspore-forming spherical bacterium, ∼0.5 to 1.0 μm in diameter, that typically forms irregular grape-like clusters similar in appearance to S. aureus. Staphylococcus xylosus is naturally present in raw meat and milk, and is used widely as a starter culture for their fermentation (especially in sausage and cheese production) [2,4,5].
During the past few years, an increasing number of human infections have been associated with this species, including urinary tract, pancreatic, cardiac, ophthalmologic, dental, blood stream, and chest infections [3,5–11]. Although it has not been reported previously in brain abscess, S. xylosus appears to be emerging as a cause of opportunistic infections even in immunocompetent subjects.
On the basis of phenotypic discrimination, S. xylosus may be confused with S. saprophyticus, which is known to be involved in some human infections [12], but it is well known that S. saprophyticus exhibits resistance to fosfomycin, high-level resistance to nalidixic acid, susceptibility to lincomycin, and negative Christie Atkins Munch-Petersen (CAMP) test in contradistinction to S. xylosus [13–16].
On the other hand, the diagnosis of cerebral abscess is often difficult, especially in children and adolescents. The classical intracranial hypertension associated with high fever is usually incomplete and sometimes absent as seen in our patient [17]. Although the abscess itself may be very large (45 mL in our case), the symptoms can be subtle, which can lead to late diagnosis.
In our patient, chronic ear infection was the predisposing factor for occurrence of the intracranial abscess following direct extension from the tegmen tympani, but the reason for the virulence of S. xylosus is still unknown. In our literature review, we could not find any other forms of CNS infections caused by S. xylosus (as meningitis, ventriculitis, epidural, or subdural empyemas).
There are no definitive guidelines for the treatment of S. xylosus infections. The species is characteristically susceptible to aminoglycosides, trimethoprim–sulfamethoxazole, quinolones, and carbapenems, but resistant to beta-lactams and fusidic acid. Susceptibility to macrolide and vancomycin is variable [8–11]. The strain in the present study was also sensitive to the antibiotics with a good clinical outcome. A regimen of 3–6 weeks of parenteral drugs followed by 1–2 months of oral antibiotic therapy is recommended to prevent relapse. Although S. xylosus is a rare cause of infection in human beings, it should be considered as a possible pathogen in CNS.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.