
Abstract
Abstract
Background:
Prosthetic joint infections caused by Listeria monocytogenes are uncommon. Such infections usually occur in patients with malignant disease, diabetes mellitus, chronic kidney disease, or liver disease or in elderly or immunocompromised patients.
Case Report:
We describe a non-immunocompromised 78-year-old male with hip infection caused by L. monocytogenes 11 years after arthroplasty. Eight years postoperatively, revision of the acetabular prosthesis was performed. Two months after that operation, the patient presented with fever, severe left hip pain, inability to bear weight, and painful restriction of left hip motion; the incision site was tender and erythematous. Joint fluid aspirate yielded L. monocytogenes and Staphylococcus epidermidis. Staged revision of the arthroplasty was performed. A gentamicin-loaded polymethylmethacrylate spacer was implanted, and the patient received ampicillin. At the second-stage operation, the cement spacer was removed, and a cement-less total hip arthroplasty was implanted. Postoperative recovery was uneventful, and two years later, the patient has had no joint problems.
Conclusions:
Predisposing conditions and co-morbidities usually are required for L. monocytogenes infection. Listeria is fastidious and is not a recognized laboratory isolate or hospital contaminant; routine cultures therefore may be negative. In approximately one-half of the reported cases, the prosthetic joint infections were treated successfully by two-stage revision surgery plus long-term antibiotic therapy. In most cases, ampicillin and gentamicin are the first choice. Cephalosporins are rarely effective.
In this paper, we describe a non-immunocompromised patient with a late hip arthroplasty infection caused by L. monocytogenes, and discuss the current concepts of diagnosis and treatment.
Case Report
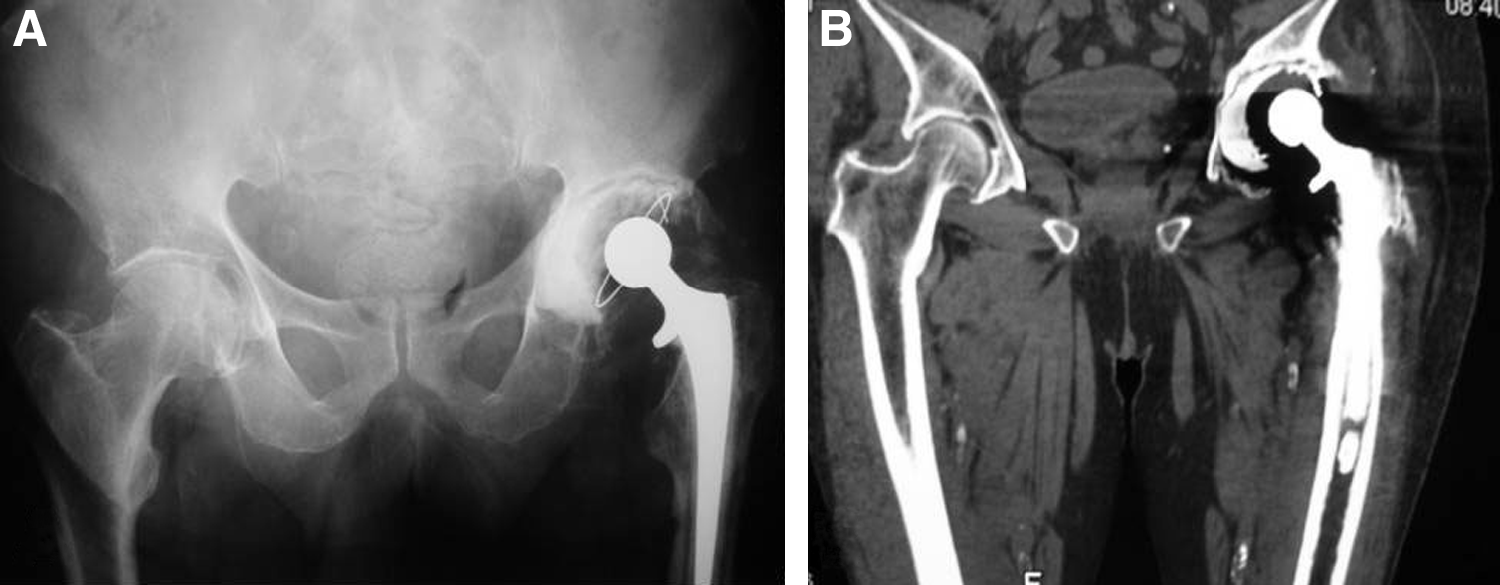
A 78-year old male had a cemented total hip arthroplasty of his left hip for degenerative arthritis 11 years earlier. Postoperative recovery was uneventful. Eight years later, because of left hip pain and radiographic acetabular prosthesis loosening (Fig. 1), revision of the acetabular prosthesis was performed. Preoperative imaging and intraoperative findings suggested a stable femoral prosthesis, so it was not replaced.

Anteroposterior radiograph of pelvis and hips of 78-year-old male shows loosening and migration of cemented acetabular prosthesis.
Two months after the revision, the patient presented with fever, severe left hip pain, inability to bear weight, and painful restriction of left hip motion; the hip incision site was tender and erythematous (Fig. 2). Laboratory examination showed an elevated erythrocyte sedimentation rate (ESR; 100 mm/first hour) and C-reactive protein (CRP; 41.4 mg/L); the white blood cell count was 7,000 cells/mm3. Blood and sputum cultures were negative. Standard radiography and computed tomography of the pelvis and left hip showed a 2-mm circumferential lucent acetabular line without femoral loosening (Fig. 3). Ultrasonography-guided aspiration of the left hip joint yielded 20 mL of fluid; cultures showed L. monocytogenes and Staphylococcus epidermidis.

Two months after the revision operation, patient presented with fever, severe left hip pain, inability to bear weight, and painful restriction of left hip motion; the incision site was tender and reddish.
Radiographic images of infected site. (
With the diagnosis of infection-related loosening, staged revision of the arthroplasty was performed. At surgery, the left hip joint was filled with dark fluid under pressure. The cemented femoral component was seated firmly and was removed with difficulty; the acetabular prosthesis and cement were loose and were extracted easily, revealing a layer of fibrous tissue. A gentamicin-loaded polymethylmethacrylate spacer was implanted, and the incision was closed in layers with deep suction drains (Fig. 4). Cultures obtained from the debrided periprosthetic tissue and fluid yielded L. monocytogenes. On the basis of the antibiogram, the patient was given intravenous ampicillin with clinical improvement within the first four days postoperatively, followed by ampicillin orally for three months.

Revision of total hip arthroplasty and application of gentamicin-loaded polymethylmethacrylate spacer.
At four months, the patient was afebrile; the ESR was 40 mm/first hour, and the CRP concentration was normal. Aspiration of the left hip joint was not performed at this stage. At the second stage of the revision operation, the cement spacer was removed, and a cement-less total hip prosthesis was implanted. Multiple cultures obtained at surgery were sterile. Perioperatively, standard antibiotic prophylaxis for hip arthroplasty, including a second-generation cephalosporin in addition to an aminoglycoside, was administered for three days.
Postoperative recovery of the patient was uneventful. Two years after the revision arthroplasty, the patient was completely symptom-free; the ESR was 40 mm/first hour, CRP was normal, and the white blood cell count was 7,200 cells/mm3. Standard radiographs showed no evidence of implant loosening.
Discussion
Several species of the Listeria genus are distributed widely in nature [9]. The most common is L. monocytogenes, a gram-positive bacillus isolated commonly from soil, water, vegetation, sewage, fresh and frozen poultry, and trout, and is part of the normal fecal flora of many mammals. In the majority of cases, infections with L. monocytogenes occur by food-borne inoculation. When the organism is ingested, it replicates in the small bowel before invading the mesenteric lymph nodes by a mechanism different from that used by other enteric pathogens, and bacteremia follows frequently. Asymptomatic human and animal carriers do exist. However, for infection to develop, predisposing conditions and co-morbidities usually are required, such as impaired cell-mediated immunity secondary to transplantation, lymphoma, or acquired immunodeficiency syndrome [1,5,7,8,10]. In the present case, a healthy, immunocompetent man developed a late L. monocytogenes infection after hip arthroplasty.
Since 1929, when Neufeldt first reported on human infection by L. monocytogenes, the spectrum of the clinical disease attributable to this microorganism has widened considerably. Nieman et al., were the first to report in 1980, on L. monogytogenes arthritis [11]. Meningitis and sepsis in neonatal infants, bacteremia, endocarditis, prosthetic valve endocarditis, and endophthalmitis are the infections reported most frequently; osteomyelitis, septic arthritis, and prosthetic joint infections are rare [1–5,7,12–21].
The hip is the prosthetic joint most often infected by L. monocytogenes, followed by the knee [1,3,4,6,7,12,14–16,18,20,21]. A remarkable feature of prosthetic joint infection with L. monocytogenes is the long period between implantation of the prosthetic device and manifestation of the infection. The late occurrence of the infection in prosthetic joints suggests a transient bacteremia and hematogenous route of infection and most likely is not associated with the surgical operation itself [1–4,7,12,14–16,18,20,21]. As in the present patient, the disease expresses as severe joint pain and fever. However, in this case, even if two months before the onset of acute symptoms and diagnosis of the infection, the patient had acetabular prosthesis revision surgery, we believe that the subsequent infection was not secondary to this operation. Even if cultures were negative at this stage, we assume that a low-grade chronic Listeria infection was present that was not diagnosed at the acetabulum revision. Instead, because of the long interval between initial total hip arthroplasty and the occurrence of the infection, hematogenous inoculation of the prosthesis is the most probable pathogenesis.
Isolation of bacteria from multiple samples increases the likelihood of diagnosis [2,12]. Co-infection with S. aureus has been reported [22]. However, Listeria is a fastidious organism, and it could easily be masked on bacteriology plates by the rapidly growing Staphylococcus. Moreover, Listeria is not a recognized laboratory isolate or hospital contaminant; routine cultures for L. monocytogenes may be negative. In this setting, molecular methods of pathogen detection such as broad-range polymerase chain reaction and sequencing are useful when a rare or unexpected micro-organism is present or the sample is collected during antibiotic treatment [2]. This distinction is clinically relevant because standard treatment for S. aureus with a penicillinase-resistant penicillin is inadequate for Listeria [23].
The treatment of L. monocytogenes prosthetic joint infections is in question. In approximately one-half of the cases reported in the literature, such infections were treated successfully by a combination of two-stage revision surgery and antibiotic therapy [5,7,14–16,21,24]. In the remaining cases, treatment by intravenous administration of ampicillin and gentamicin followed by prolonged oral administration of trimethoprim/sulfamethoxazole or ampicillin [15,20] was efficacious. In immunocompromised patients, prolonged antimicrobial treatment certainly is necessary [6,15,20,25]. In all cases, the infection appears to be more insidious and indolent than similar infections with S. aureus, and in view of the frequent recurrence because of the inoculation of the prosthesis and the intracellular growth of the organism, a six-week period of intravenous antibiotic therapy followed by at least three months of oral therapy is indicated [1,3,4,7,12,14–16,18,20,21]; lifelong antibiotic therapy does not seem to be necessary [18].
The best antibiotic for L. monocytogenes prosthetic joint infections is unclear; in most cases, ampicillin and gentamicin are the first choice [1,3–5,12,14–16,18,21,25]. Penicillin (or trimethoprim/sulfamethoxazole in penicillin-allergic patients) also has been used in addition to ampicillin, although both agents are bacteriostatic at the blood concentrations obtained with standard doses [9]. On the other hand, gentamicin is bactericidal at blood concentrations obtained with standard doses [9]. Aminoglycosides have not been used widely as single agents for L. monocytogenes infections; the combination with penicillin or ampicillin acts synergistically against the organism [9,26]. Cephalosporins are rarely effective.
In the present patient, we performed two-stage revision of the hip arthroplasty in addition to giving two weeks of intravenous antibiotic followed by three months of oral ampicillin. At the time of reimplantation, multiple cultures of the tissues were negative. We cannot tell whether shorter courses of treatment, other antimicrobial agents, or one-stage revision and reimplantation of the prosthesis would have been equally effective.
In conclusion, as the scope of patients having arthroplasty expands, the incidence of late prosthetic infections will increase, and the variety of infecting organisms will broaden. The role of prophylactic antibiotics for such infections is unknown. This case report emphasizes the risk of late L. monocytogenes prosthetic joint infection in a non-immunocompromised patient. Early diagnosis of the infected arthroplasty was performed through clinical, laboratory, and radiologic findings. Early treatment with two-stage revision of the prostheses and a 3.5-month course of ampicillin was successful.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.