
Abstract
Abstract
Background:
An increasing number of publications related to the concept of recurrent ventilator-associated pneumonia (VAP) has emerged in recent years. The clinical relevance of this publication trend could suggest failure to prevent VAP.
Methods:
Review of articles addressing recurrent VAP, which were scrutinized for their definitions and methodology, seeking to determine the actual meaning of “recurrence.”
Results:
A preponderance of the early papers on recurrent VAP used definitions that create the possibility and even, in some cases, the likelihood that what was being addressed actually was persistent VAP. These studies, mostly from the same investigator group, considered “recurrent” VAP to appear as early as three days after the initial diagnosis while patients were still receiving antibiotics to treat that initial episode. The blurring of the concepts of “recurrence” and “persistence” is apparent in the methodology and the results.
Conclusions:
Existing evidence-based guidelines regarding the prevention and treatment of VAP should be applied to reduce the incidence of (i.e., prevent) and treat VAP effectively. A distinction should be made between “recurrence” and “persistence” in order to determine whether clinical inadequacies exist in preventive or therapeutic practices, respectively. An objective process for defining the resolution of VAP should be developed to enable this distinction to be made.
In recent years, there have been several publications discussing recurrent VAP [7–14]. Recurrent VAP increases the total number of antibiotic treatment days, which should not come as a surprise. It is not clear whether recurrent VAP increases morbidity and mortality rates, although it would be reasonable to assume some association. Patients who are subject to recurrent VAP would be likely to be ventilator dependent for a longer period than patients who do not develop recurrent VAP, as they would have to remain on mechanical ventilation to develop a ventilator-associated pneumonia. By the same token, it has been claimed that recurrent VAP decreases the number of ventilator-free days [9]. However, to a large degree, this may be more a condition for than a result of VAP as, again, one must be on a ventilator to have pneumonia be considered VAP.
Literature Analysis
One of the first studies mentioning recurrent VAP was by Combes et al. [7]. Those authors performed a 16-month prospective observational cohort study of 124 patients with an initial episode or VAP. Patients who had clinical or radiologic evidence of VAP underwent confirmatory fiberoptic bronchoscopy. The bronchoscopic criteria confirming VAP were identified as bacteria in 2% or more of cells in the bronchoalveolar lavage (BAL) fluid and at least one bacterial species cultured at a concentration of ≥103 colony-forming units (CFU)/mL from a protected-specimen brush sample or ≥104 CFU/mL from BAL fluid. The authors reported finding monomicrobial pneumonia in 52% of the cases, the rest being polymicrobial. Among the polymicrobial VAPs, two bacterial strains were encountered in 34%, three strains in 8%, and four strains in 6% of the entire group of 124 patients.
Importantly, the authors noted that initial presumptive antibiotic therapy was appropriate in 92% of the patients with monomicrobial VAP, whereas only 75% of patients with polymicrobial VAP received appropriate antimicrobial therapy initially (p = 0.01). The primary finding of the investigation was that the epidemiology and outcome of monomicrobial and polymicrobial VAP did not differ significantly. However, this result suggests a potential Type II error, likely attributable to a small study population, in view of the accumulating literature indicating that inadequate initial presumptive antibiotic therapy is associated with poorer outcomes [15–21].
The article also mentioned the concept of a “relapse” of VAP [7]. The investigators noted that 18% of monomicrobial infections relapsed, which was not statistically different from the 27% of polymicrobial cases that relapsed. The failure of this difference to achieve statistical significance was, again, likely attributable to the relatively small number of study patients. Overall, the authors noted that 23% of the patients with VAP experienced a relapse. Unfortunately, the authors provided no definition of relapse as applied in their study.
One year later, the same group reported another study performed on the same 124 patients [8]. However, in this analysis, the researchers intensified their investigation into VAP recurrence. Ventilator-associated pneumonia, whether recurrent or initial, was defined by the same clinical, radiologic, and bronchoscopic criteria the group had used to define the initial episode of VAP in the previous report on polymicrobial VAP. Risk factors for recurrent VAP were evaluated in patients who were alive eight days after the onset of the initial VAP. Whenever a patient became febrile, had purulent tracheal secretions, deteriorated clinically, developed a new pulmonary infiltrate, or had progression of an existing infiltrate, fiberoptic bronchoscopy was performed, and the results were analyzed for confirmation of recurrent VAP.
It is at this point in the methodology of the study that the terminology becomes problematic. The authors considered recurrence to be a relapse if a confirmatory culture of the same initial infecting organism was obtained after the end of the patient's 14-day antibiotic course. Presumably, this practice assumed that the infection had been cleared, the symptoms had resolved, and the radiographic images had returned to normal. Unfortunately, the manuscript provides no indication that such signs of resolution were sought or recorded. Rather, the single criterion of having completed an arbitrary 14-day course of antibiotics was considered sufficient to maintain that any subsequent culture of the same organism represented a recurrent or relapsed infection.
Even more troubling was the statement that “recurrence was considered a persistent infection” if at least one of the initial causative bacteria was cultured at a significant concentration and the patient was still receiving his or her arbitrary 14-day course of antibiotics. Of course, this situation would occur because patients were analyzed eight days after the onset of the initial VAP (i.e., while still receiving their 14-day course for the initial VAP).
Equating the term “persistence” with the term “recurrence” seems oxymoronic. Inherent in the concept of recurrence is the sense that something that once was present left and then came back, whereas persistence suggests it never went away. In our analysis of the effectiveness of measures to prevent and treat VAP, it is important to be precise in our terminology. Infections that persist most likely are attributable to inadequate antibiotic therapy (i.e., poor selection, resistant strains, dosing inadequate to achieve effective tissue concentrations), inadequate source control (i.e., insufficient drainage, lack of debridement of necrotic tissue, failure to remove foreign bodies), or poor host response (i.e., immunosuppression, poor nutritional status, or inherent immune deficiency). However, infections that are recurrent indicate a failure to prevent infection, which is discussed later.
Finally, the authors considered a superinfection to exist when a species different from the initial infecting strain was cultured either during or after the 14-day antibiotic course. However, this concept is also troubling, as such an organism could merely represent part of a polymicrobial infection that was not detected initially.
The authors identified six operating characteristics of survivors on the eighth day of treatment (while still receiving antibiotics for the original VAP) that predicted VAP recurrence. These were: (1) Acute respiratory failure as the initial reason for mechanical ventilation; (2) a radiologic score of >7 on the first day of treatment for the original VAP; (3) a temperature of >38°C on the eighth day of treatment (i.e., while still receiving antibiotics for the original VAP); (4) a radiologic score of >8 on the eighth day of treatment (again, during the original antibiotic regimen); (5) persistence of mechanical ventilation on day 8; and (6) the presence of acute respiratory distress syndrome (ARDS) on day 8.
No bacterial species from the first VAP episode was predictive of recurrent VAP. The investigators also found that there was no recurrent VAP after successful liberation from the ventilator.
If one understands that the authors never described or defined whether effective treatment of VAP had occurred in these patients before a reinvestigation was declared a recurrence, the data seem predictable. The fact that the persistence of mechanical ventilation on day eight was associated with “recurrent” VAP is obvious: if patients had been extubated and developed pneumonia while no longer being ventilated, the “recurrence” would not be identified as VAP. In fact, those patients who were weaned and extubated did not develop recurrent VAP, which, of course, they could not as they were not being ventilated. The persistence of fever and pulmonary infiltrates on the eighth day of continuous antibiotic therapy for the initial VAP strongly suggests an infection that has not been eradicated completely. The presence of ARDS on day eight also suggests a more severe disease process, which likely necessitates more aggressive therapy for eradication of the pneumonia. In other words, most of the predictive phenomena identified could suggest a persistent infection rather than a recurrent one.
A few years later, another publication emerged from the same group again investigating recurrent VAP [9]. This involved a multivariable analysis of predictors of VAP recurrence and death by day 28 after initial VAP onset in 401 patients enrolled in the PNEUMA trial, which was a multi-center, randomized study comparing 8 vs. 15 days of antibiotics for microbiologically proved VAP. In the study protocol, the authors performed fiberoptic bronchoscopy with distal sampling on the basis of fever, purulent tracheal secretions, or a new or progressive infiltrate before any new antibiotics were started. They also performed bronchoscopy for hemodynamic instability, deterioration of arterial blood gases, or any event that necessitated a change in the antibiotic regimen. They found that 27% of patients (110/401) developed “recurrent” VAP within 28 days of the initial VAP onset. Interestingly, in Figure 1 of the published paper, they identify patients with “recurrent” VAP as early as three days after the initiation of treatment for the initial VAP (Fig. 1). In fact, there were 12 “recurrent” VAPs that occurred within one week of the initial VAP, while patients were still receiving antibiotics for the initial VAP in either arm of the study. Of these early “recurrences,” one was a “relapse” (i.e., the investigators were able to re-culture the original VAP isolate), which makes one wonder what happened to the concept of “persistent” infections identified in the previous paper by the same group. Eleven of the “recurrent” VAPs were “superinfections” (i.e., an organism different from the original strain was isolated, of which nine were highly resistant bacteria such as methicillin-resistant Staphylococcus aureus [MRSA] and non-fermenting gram-negative bacilli). Of course, given the early stage of therapy at which these “recurrent” VAPs were being identified, it is likely that the “superinfections” were simply other organisms participating in a persistent polymicrobial infection, and that they either escaped early detection or their concentration in the BAL sample was inadequate to warrant concern. Again, as in the previous studies, there was no evidence of clinical resolution prior to declaring the VAP a “recurrence,” making such a possibility likely.
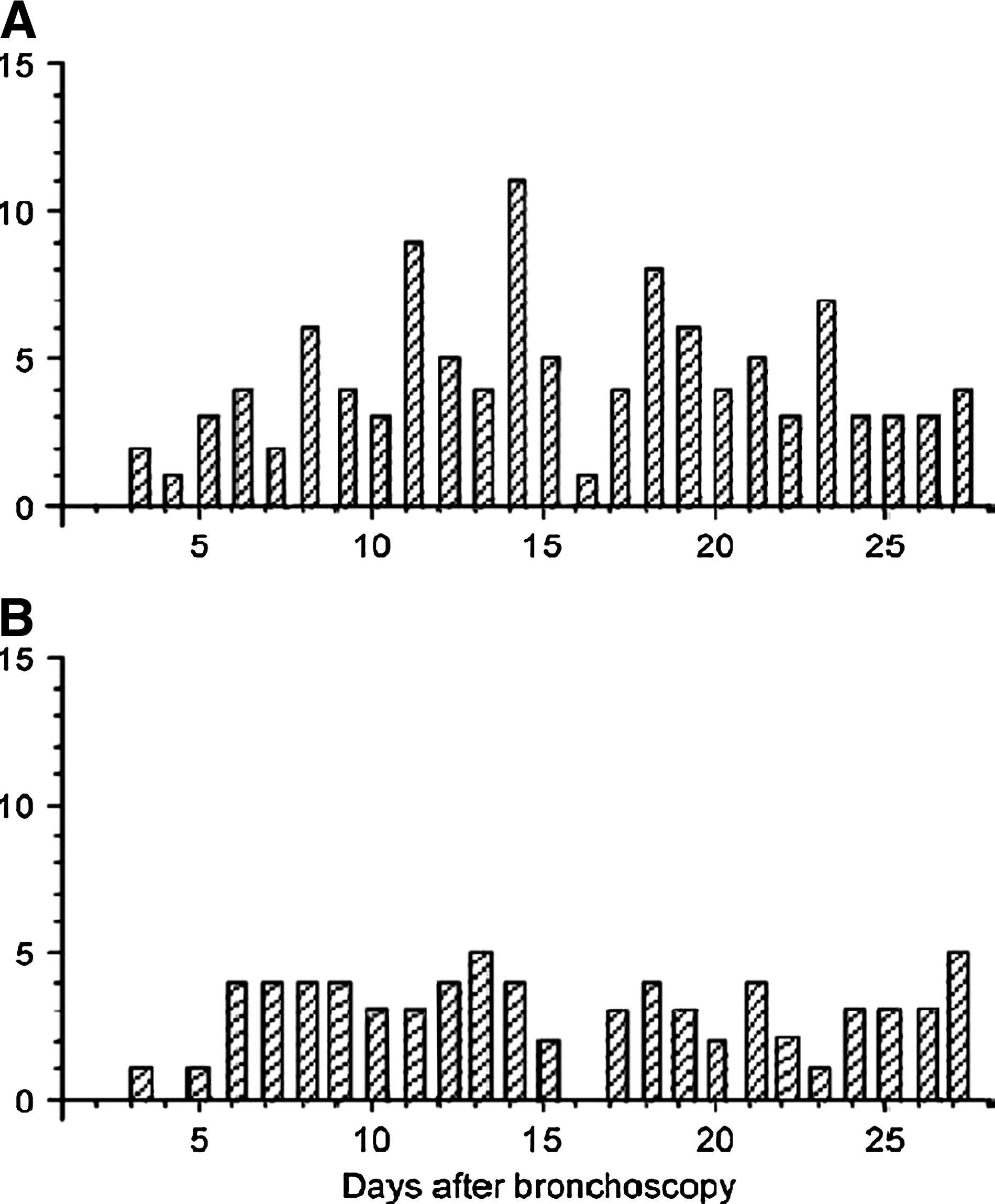
Distribution of the numbers of recurrent infections (
One of the more intriguing papers regarding the issue of recurrent VAP is one that examined procalcitonin kinetics as a prognostic marker [10]. The procalcitonin concentration increases during bacterial infections, but not during viral or non-infectious inflammatory conditions. Elevated procalcitonin concentrations have been associated with a poorer prognosis in sepsis, septic shock, and VAP. Luyt et al. studied 63 patients with microbiologically confirmed VAP who survived longer than three days after the diagnosis. Serum procalcitonin concentrations were measured on days one, three, and seven. The primary outcome measurement was an “unfavorable outcome,” defined as death, extrapulmonary infection necessitating antibiotics, or VAP recurrence. Recurrence in turn was defined as a “new VAP episode, that is, new clinical signs compatible with pneumonia, confirmed by significant (≥104 cfu/mL) growth in quantitative culture of new bronchoalveolar lavage fluid.” However, the authors stated further that the definition of recurrent VAP “included persistent infection (the same pathogen responsible for episode 1), relapse (the same pathogen as episode 1 but after the end of antibiotic therapy), and superinfection (another pathogen, at any time).” Nowhere in the manuscript do they say that the first episode of VAP had resolved before announcing a recurrence. In fact, the equation that “recurrence” = “persistence” apparent in their definition is more understandable when one realizes that four of the authors were among the authors of the two previously cited papers. In this study [10], 38 (60%) of 63 enrolled patients had unfavorable outcomes, which included 21 “recurrences.” The procalcitonin and C-reactive protein concentrations were significantly higher in patients with unfavorable outcomes, although there was no specific association sought with recurrent VAP.
Siempos et al. conducted a meta-analysis of VAP recurrence [14]. Of 94 potentially relevant reports, the authors excluded 87 for various reasons, leaving only seven complete and relevant papers covering 969 patients. For the meta-analysis, recurrence was defined as a new microbiologically-documented VAP episode with at least one bacterial species grown from invasive respiratory specimens taken after the initial isolate of VAP pathogen(s). There were two types of recurrence: (1) Relapse, defined as a second sample containing the same pathogen with the same susceptibilities as the initial pathogen(s), and (2) superinfection, defined as a second sample containing different pathogen(s) from the initial VAP pathogen(s). It is important to note that persistence was not defined. Moreover, there was no requirement for a determination of resolution of the initial VAP episode before a recurrence could be declared. The overall VAP recurrence rate in this meta-analysis was 26.8%, ranging from 14% to 40%. There was no difference in VAP recurrence attributable to differing bacterial pathogens. Only the presence of acute lung injury, ARDS, or shock on the day of the initial VAP diagnosis were significantly associated with VAP recurrence.
Unfortunately, there are problems with this meta-analysis. First, of the 87 excluded papers, the authors claimed that four were excluded because “they were based, totally or mainly, on the same patient population.” However, there were other, non-excluded papers that could be accused of the same problem: (1) The first two papers by Combes et al., described above, involved exactly the same patient population; (2) the procalcitonin paper by Luyt et al. included patients from the PNEUMA trial, as did the third Combes et al. paper described above; and (3) four of the seven papers included were from the same group. A more serious concern, however, is that there does not appear to be any concept that there should be evidence of elimination of the initial VAP episode before considering symptomatology and clinical findings suggestive of VAP to be a recurrence. Although two of the seven papers did use the criterion of completion of the initial antimicrobial therapy course before considering the VAP to be a recurrence, it is not clear that all signs and symptoms of the first pneumonia had been eradicated.
Discussion
There are serious problems with the existing literature on recurrent VAP. Although MRSA and other multidrug-resistant pathogens often are considered responsible for recurrent VAP, they do not demonstrate as such consistently, especially in large series. This phenomenon could be attributable to dilution from cases that are persistent VAP instead of cases that are true recurrent instances of VAP. It is not clear how many of the reported cases were recurrent VAP vs. how many were persistent. For example, when fever and infectious markers (such as procalcitonin) appear as “predictors” of “recurrence,” are we not really observing an ongoing process? In fact, there does not seem to be any concept, much less a consensus, on what constitutes VAP resolution. Many authors have considered the initial VAP to have resolved only when an antibiotic treatment course of arbitrary duration has been completed. Although this appears to be the dominant position in the literature, this weak definition leaves open the possibility that an undertreated initial VAP could be considered a “recurrent” VAP. It would make more sense to define VAP resolution as the absence of the signs and symptoms of VAP; that is, the same criteria that established the diagnosis of VAP initially should no longer be evident. Such an approach would reduce the possibility that under-treated persistent VAP would be identified as “recurrent.”
Surgeons understand the concept of recurrence. For example, we often must deal with recurrent hernias, which we can distinguish clearly from a persistent hernia. Inherent in the definition of recurrence is the concept that at some point, the hernia had been repaired. Imagine the response to an operative report wherein the surgeon states: “At this point, while suturing in the mesh, the patient strained, pushing the viscera through the defect, making this a recurrent herniation.” There certainly would be financial incentives for such an approach, as recurrent hernia repairs are reimbursed at a higher rate than initial repairs of hernias, but such concepts clearly are erroneous, and such billing efforts would be determined, appropriately, to be fraudulent.
It is true that making the diagnosis of VAP can be problematic. There is no method of diagnosis that is 100% accurate, sensitive, and specific. Even pathologic lung biopsy is not perfect, with a measured κ statistic of 0.916 [22]. Thus, whereas diagnostic criteria for VAP are controversial, identifying a case of recurrent VAP is even more problematic. Aside from having imperfect criteria for diagnosing VAP, there appears to be no consistent process for determining resolution of the initial VAP. Consequently, the distinction between persistent and recurrent VAP can be blurred. Because of this, our opportunities to improve the processes of care can be muddled because we are not certain of the nature of the problem. Persistent VAP suggests failure of the therapeutics selected to treat the initial infection, either through inappropriate antibiotic selection, inadequate dosing, or ineffective pulmonary toilet. On the other hand, the presence of a truly recurrent VAP (i.e., one in which the initial VAP resolved) suggests failure of VAP prevention.
There has been a great deal of attention applied over the last several years to trying to prevent VAP. Guidelines have implemented in many healthcare institutions, usually at the urging of third-party payors, often employing the “ventilator bundle” [6]. This bundle consists of four components: (1) Peptic ulcer disease prophylaxis; (2) deep venous thrombosis prophylaxis; (3) elevation of the head of the bed; and (4) a sedation vacation. The initial report of the bundle's use suggested a 44% reduction in the incidence of VAP. However, subsequent experience has not been so positive, which is not surprising in that only two of the items in the bundle (i.e., head-of-bed elevation and the sedation holiday) have the potential to prevent VAP directly. All too often in the medical literature, authors load consensus guidelines with whatever Level 1 evidence they can find, because such high-quality studies are relatively rare. It is likely for that reason that only 50% of the “ventilator bundle” items are targeted directly at prevention of pneumonia. A recent systematic literature review failed to identify consistent evidence of bundle's success [23].
In seeking potentially better ways to prevent VAP, treat VAP, and prevent recurrent VAP, it may be best to seek a more comprehensive approach. The American Thoracic Society and the Infectious Diseases Society of America have produced a comprehensive review and set of guidelines dealing with nosocomial pneumonias, including VAP [1]. The document cites 95 evidence-based points or recommendations, 14 that are Level III, 58 Level II, and 21 Level I in terms of the quality of the supporting evidence. Of the Level I items, 11 address VAP prevention, nine address VAP treatment, one address both, and 2 address neither.
The Level I items focused on VAP prevention are listed in Table 1. However, many of the items are related only indirectly to the issue of contamination of the tracheobronchial tree. In fact, only the first six (highlighted in italics) actually can prevent aspiration of microbes into the tracheobronchial tree.
Points in italics are those that directly prevent aspiration of bacteria into the lungs.
Similarly, Table 2 identifies the 10 Level I items that address VAP treatment. However, some identify what not to do and how the treatment regimen can be modified. Only the first four items (highlighted in italics) actually address positive treatment strategies designed to identify and annihilate the invading micro-organisms. Given the quality of the data and the direct impact of the items highlighted in Tables 1 and 2, it would seem that a better ventilator bundle could be created through their consistent use.
Points in italics are possible treatment strategies.
Conclusions
A close review of the current literature on recurrent VAP reveals it to be flawed. Many if not most cases of “recurrent” VAP could actually be cases of persistence. Because there is no established definition of VAP resolution, analytical flaws appear to have developed, creating a situation where a new BAL culture is identified as a case of “recurrent” VAP in a persistently ill patient.
The distinction between recurrent and persistent pneumonia is critical, as they imply different clinical failures. Recurrent pneumonia suggests that measures designed to prevent pneumonia, such as those identified in Table 1, either have failed or have been implemented improperly. On the other hand, persistent pneumonia suggests that treatment measures, such as those identified in Table 2, have failed. It is only through careful and critical analysis of clinical shortcomings that we are able to improve our processes of care. Therefore, one should be skeptical of concepts that equate persistence with recurrence.
Despite the literature's flaws, it does appear to demonstrate that recurrent VAP is associated with worse disease at the time of the initial episode and longer time on the ventilator. However, any future understanding of recurrent VAP should establish firmly that the initial VAP has resolved by using stronger criteria than completion of an antimicrobial regimen of arbitrary duration. Given that specific criteria are applied in making the diagnosis of pneumonia, it would seem logical that the absence of those same criteria could be taken as a sign of complete resolution.
The initial ventilator bundle approach to preventing VAP, although simple and therefore popular, has had limited effectiveness in changing clinical outcomes. Broader and more consistent adherence to published guidelines designed to prevent and treat VAP should reduce persistence and prevent recurrence.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Presented at the 29th Annual Meeting of the Surgical Infection Society, Chicago, Illinois, May 6–9, 2009.