
Abstract
Abstract
Background:
With the increasing number of diabetic patients, it is likely that the number of diabetic foot infections will increase in upcoming years. Better strategies are required to optimize the outcomes of these infections.
Methods:
The current literature was reviewed to define best practices in the management of diabetic foot infections.
Results:
Management requires differentiation of colonization from infection. Classification of the severity of an infection is commonly important to interpret the effectiveness of care. Although many kinds of bacteria are associated with these infections, methicillin-resistant Staphylococcus aureus has emerged as a major pathogen. Management of these severe infections usually necessitates hospitalization with rigorous medical management, prudent debridement of wounds, and appropriate antibiotic therapy targeting the responsible pathogens.
Conclusions:
Effective multidisciplinary management of the diabetic foot can reduce the rate of severe infections and the number and extent of amputations.
Foot problems in diabetic patients increase morbidity and mortality rates. Four hundred forty-nine diabetic patients with foot ulcers were followed for 12 mos [4], and only 45% were alive, without amputation, and ulcer free at the endpoint. A total of 17% died [5]. Patients with a foot ulcer had a three-year survival rate of 72%, compared with 87% if no foot ulcers were noted [6]. These facts emphasize that most physicians need a working knowledge of the pathophysiology and management of foot ulcers in patients with diabetes mellitus.
Foot ulcers in diabetic patients have multiple causes. Risk factors include peripheral neuropathy, vascular insufficiency, osteoarthropathic deformities, patient disabilities, maladaptive patient behavior, and healthcare system failures [3]. Peripheral neuropathy, injury, and foot deformity are present in 63% of patients with a foot ulcer [1,7]. Once an ulcer is present, infection becomes a major concern, although infection is rarely the inciting cause.
Classification of Foot Ulcers
A diabetic foot ulcer is commonly present without infection [3]. This is important to remember, as a non-infected diabetic ulcer needs treatment aimed at the cause [8]. This treatment includes proper wound care, off-loading of foot or contact point pressure, optimizing glucose control, and appropriate consultation for what is believed to be the inciting cause. No antibiotic therapy is necessary.
Various classification systems are used for foot ulcers. The Wagner classification uses a grading system from 0 to 5 points [8]. Zero indicates no ulcerations, whereas 4 and 5 indicate infection is present, and 5 indicates extensive gangrene, usually necessitating amputation. The Infectious Diseases Society of America (IDSA) guidelines have a classification system just for diabetic foot infections. This system ranks infection from uninfected to severe and by Perfusion, Extent/size, Depth tissue, Infection, Sensation (PEDIS) grade 1–4 [3]. These systems can be helpful for clinical decision-making concerning the need for debridement and antibiotic use.
Acute infections
The pathogens infecting diabetic ulcers are varied and relate to the clinical presentation of the patient. Most ulcers become infected either as a result of poor wound care or poor management of the patient's diabetes mellitus. An acute ulcer that has not been treated with antibiotics is most likely to be infected with common skin organisms [5]. The pathogens most likely to be isolated are beta-hemolytic streptococci and Staphylococcus aureus, either methicillin-sensitive or methicillin-resistant (MRSA) [9].
Chronic infections
Once a chronic ulcer is present or the ulcer has been treated with multiple courses of antibiotics, the bacterial isolates can change. Beside gram-positive organisms, Enterobacteriaceae are commonly encountered. If the lesion has been treated with protracted periods of soaking, Pseudomonas aeruginosa is common [3,10].
Fetid foot
Ulcer chronicity without healing and multiple antibiotic courses will allow almost any microorganism to be isolated, including enterococci and even fungi. The final step in this process occurs when ischemia develops. This is the classic fetid foot, when bacterial isolates include aerobic and anaerobic bacteria [11,12]. These patients commonly have multiple bacterial isolates, including Bacteroides fragilis.
It is important to understand the clinical progression of infection in a diabetic ulcer so overtreatment is avoided. Oral antibiotics often are sufficient for acute infections. These antibiotics are directed at streptococci and staphylococci. The risk of MRSA infection must be assessed [13]. Isolation of MRSA continues to increase, although empiric MRSA coverage is not recommended [3,14]. Treatment of chronic infected ulcers should include coverage for gram-positive and gram-negative organisms, including P. aeruginosa. A patient with fetid foot should receive initial broad-spectrum antibacterial coverage, although debridement and amputation are the most important interventions.
Besides the clinical history, the degree of tissue involvement is used to estimate the severity of infection [3]. Uninfected wounds show no signs of inflammation. A mild infection has at least two of the following signs: Purulence, erythema, pain, tenderness, warmth, or induration. Cellulitis is limited to no greater than 2 cm around the ulcer, and no systemic signs are present. A moderate infection shows more than one of the following: Cellulitis > 2 cm from the ulcer, lymphangitic streaking, spread beneath the superficial fascia, deep tissue abscess, gangrene, or deep tissue involvement. A severe infection is present when the patient has systemic signs of infection. This classification system can be used to assess a patient's need for hospitalization. Mild infections do not necessitate hospitalization, whereas hospitalization is necessary for severe infections. Moderate infections may or may not necessitate hospitalization.
We recently completed a review of a large database, trying to identify factors that affect outcomes for diabetic patients with complicated skin and soft tissue infections [15]. This study involved a retrospective review of prospectively collected data from the Cardinal Health Outcomes Research Database [15]. Data from 97 hospitals over a four-year period (2003–2007) were analyzed [16]; all patients had been hospitalized for a complicated skin and soft tissue infection. A foot infection was the reason for hospitalization of 2,220 of the 3,030 patients. The most common bacterial isolates are listed in Table 1. Methicillin-resistant S. aureus was the only bacterium to show an increase over time in both foot and non-foot infections. The increase was from 14.0% to 24.6% (p = 0.006) for non-foot infections and from 11.6% to 21.9% (p < 0.0001) for foot infections (Fig. 1).
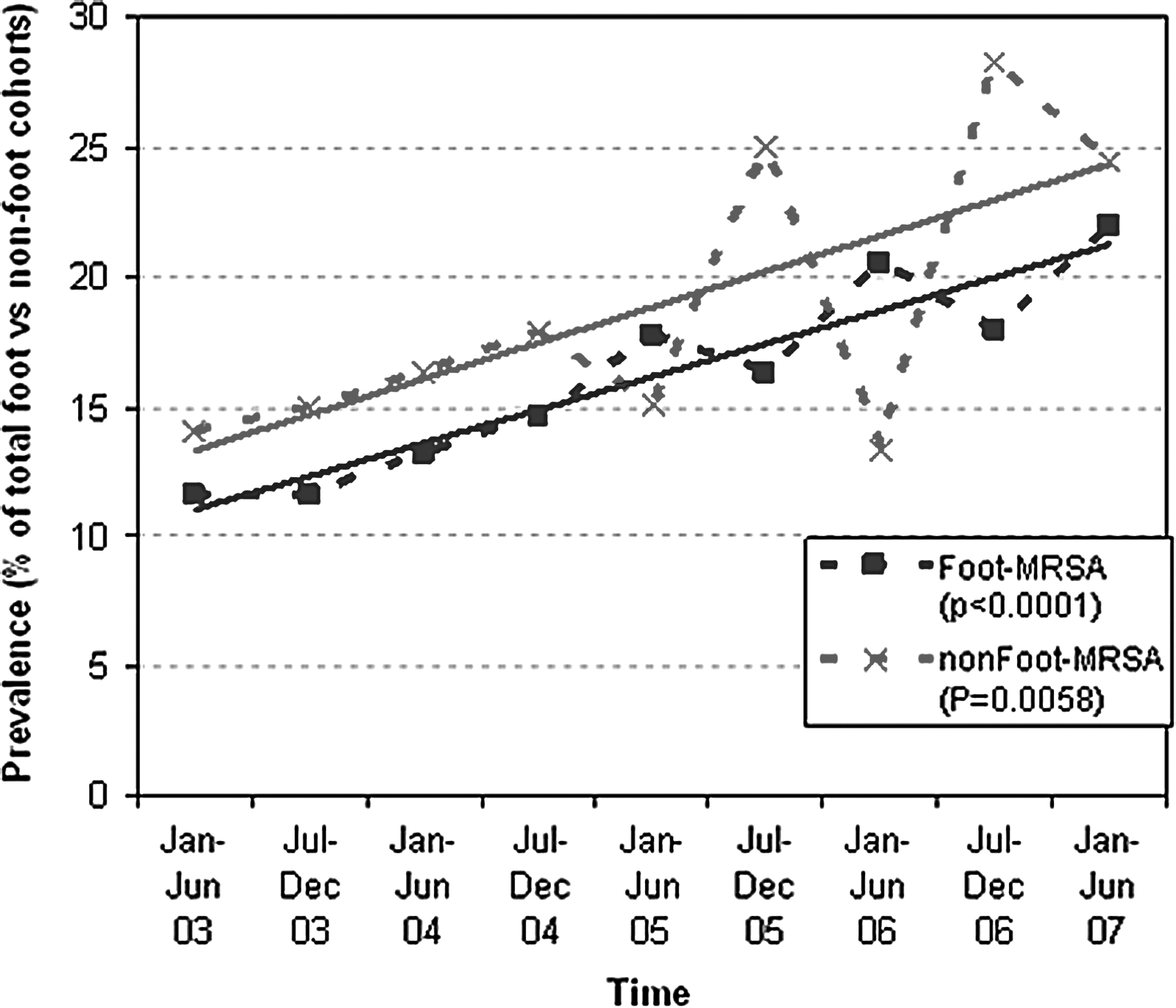
Prevalence of methicillin-resistant S. aureus in foot (filled squares) and other sites among patients with diabetes mellitus hospitalized in 2003–2007. Reprinted from Lipsky et al. [16].
From Lipsky et al. [16].
Patients with infections of sites other than the foot were more severely ill at presentation and had a higher mortality rate than patients with foot infections (2.2% vs. 1.0%; p < 0.05). Independent risk factors for death were polymicrobial infections including P. aeruginosa (odds ratio [OR] 3.1), monomicrobial infection with other gram-negative bacteria (OR 8.7), greater illness severity (OR 1.9), and transfer from another hospital (OR 5.1). These factors and the need for major surgery also were associated independently with longer stays and higher costs.
A poster presentation at the European Congress of Clinical Microbiology and Infectious Disease used the same database to evaluate lower-extremity amputation in patients with diabetes mellitus and foot infections [17]. Among 3,000 patients, 647 had an amputation. Polymicrobial infection was found in 57% of the patients requiring amputation. Lower-extremity amputation also was associated with surgical site infection in the leg, vasculopathy, hypoalbuminemia, leukocytosis, coagulopathy, and polymicrobial infection. Methicillin-resistant S. aureus and Pseudomonas were the two bacteria found most commonly in the polymicrobial infections.
Management principles are broadly outlined in Figure 2 [18]. Initial management involves proper ulcer and foot care and assessment for ischemia and neuropathy. Normalization of the blood glucose concentration must be part of the overall treatment plan, as well as good nutrition and off-loading of the foot. Review of previous treatments, especially antibiotic exposure, is imperative for proper categorization of possible pathogens [3,5]. Culture acquisition is imperative. Tissue culture should be used and swab cultures discouraged [19]. Proper debridement when necessary should be done early and be conservative whenever possible [20]. Revascularization may play a role after adequate debridement [21]. Antibiotic choices can be informed by the IDSA guidelines [3,13]. Antibiotic therapy is always an adjunct in the overall treatment plan, and narrowing of the antibiotic regimen should occur whenever possible. Treatment failures must be evaluated for osteomyelitis, and if it is present, bone debridement should be done if possible [21]. Amputation is one form of debridement, but lesser procedures also can be successful in properly chosen cases [22].
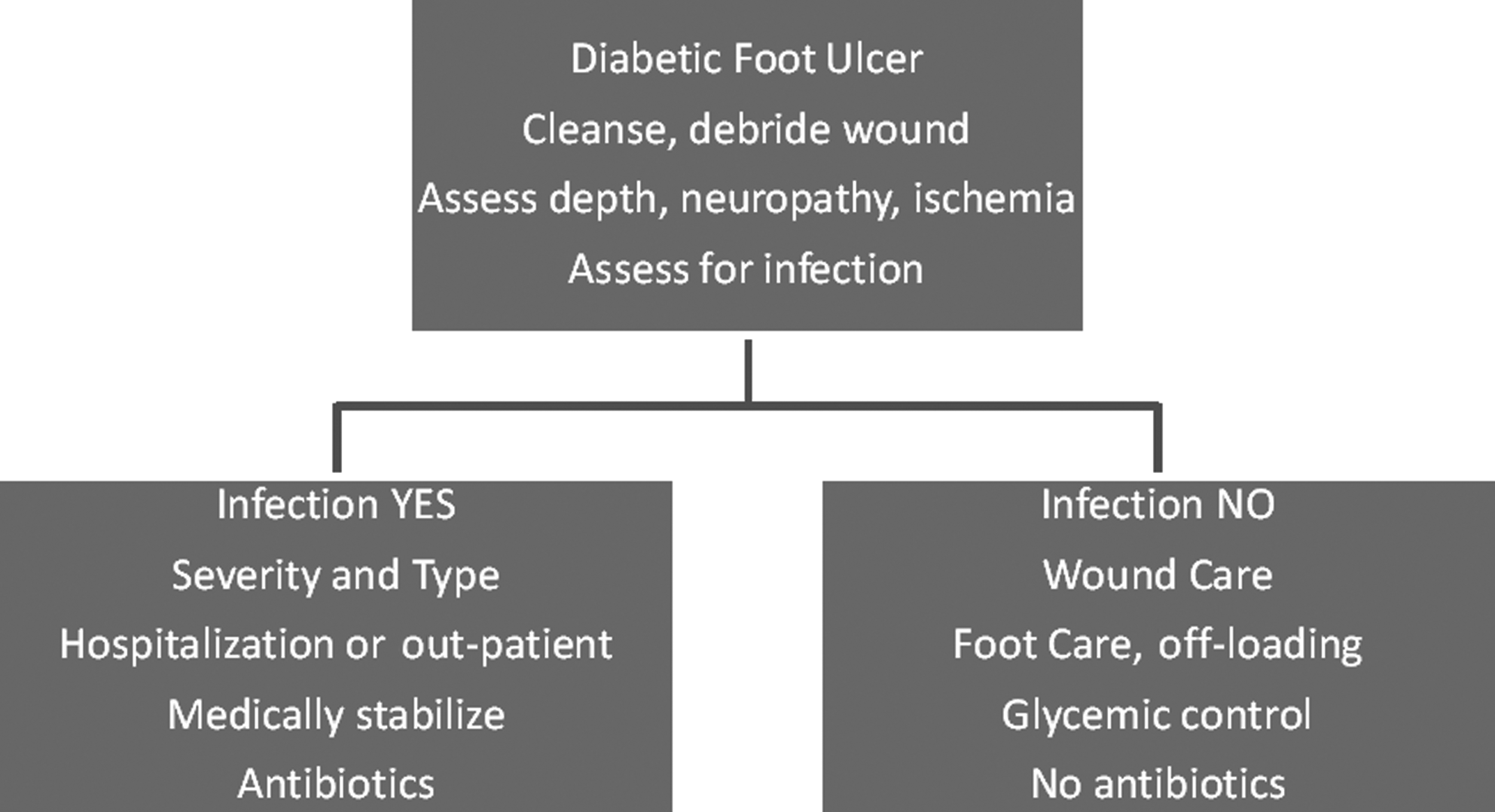
Management plan for diabetic foot ulcer.
In summary, the patient with diabetes mellitus and a foot infection represents an opportunity for care involving many disciplines and modalities. It is hoped that proper management can prevent a polymicrobial infection and amputation.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Presented at the 29th Annual Meeting of the Surgical Infection Society Chicago, Illinois, May 6–9, 2009.