
Abstract
Abstract
Background:
Synthetic mesh is used commonly in the repair of abdominal wall hernias. Infection at the surgical site where mesh is present poses a formidable clinical problem.
Methods:
The current surgical literature was reviewed to formulate accepted approaches to the management of hernia repairs with infected mesh.
Results:
Prevention of mesh infection is best achieved by judicious use of systemic antibiotics. Topical antibiotics often are used without convincing evidence to support their value. Laparoscopic repairs have lower infection rates than open repairs. Evidence is lacking to support lower rates of infection with mesh of specific composition or with antibacterial agents that coat the mesh. The diagnosis of mesh infection is principally a clinical one. Repairs of infected mesh usually necessitate antibiotics and removal of the foreign material. Clinical judgment is required for attempts at salvaging portions of the mesh. Component separation or biological materials may be used in those circumstances for hernia repair in which large defects are created by removal of the infected synthetic material.
Conclusions:
Prevention of mesh infections remains the best strategy. Clinical judgment is essential in determining the degree of mesh removal. Continued clinical studies are necessary to improve the outcomes of established mesh infection in hernia repairs.
Nearly all herniorrhaphies, particularly inguinal procedures, are performed in the outpatient setting, which influences the ability to estimate the occurrence of infection accurately because of variability in follow-up and capturing the number of patients receiving the procedure [1]. Similarly, lack of standardization of the definition of “infection” creates additional variability. Nonetheless, randomized controlled trials utilizing the criteria of the U.S. Centers for Disease Control and Prevention (CDC) for the definition of surgical site infection (SSI) and a reasonable degree of followup in years provide estimates of around 1%–2%, which translates into about 7,500 to 15,000 cases a year [1–3]. Perhaps this is not an enormous burden, but those who have managed infections in the context of mesh typically come away with a great desire to prevent them.
Prevention
Preparation
The use of universal sterile precautions (i.e., sterile gown, gloves, field drape, and disinfectant solution) clearly reduces central venous catheter-related infections, and such data can be extrapolated to the equally clean procedure of mesh herniorrhaphy [4, 5]. It is imperative to permit the preparative disinfectant to air dry to capitalize on its antimicrobial properties; hasty blot drying with a laparotomy pad or towel negates any benefit. Many surgeons utilize additionally a variety of adherent drapes, such as those impregnated with iodophor, to minimize contact between skin, gloves, and mesh. Such additional barrier precautions, theoretically, should translate into a reduced risk of infection. However, available data suggest the contrary. In 1998, Webster and Alghamdi conducted a meta-analysis of the use of sterile plastic adhesive drapes (i.e., Incise™ or Opsite™ [Smith & Nephew PLC, London, United Kingdom]; Ioban™ [3M Company St. Paul, MN]) to reduce surgical site infections after open operations, including cesarean section and general, abdominal, and hip surgery [6]. The studies were of variable quality, with only two meeting the criteria for high quality. The authors could not identify evidence of a protective effect. To the contrary, the data suggested harm and a higher risk of infection: 13.9% (n = 1,556) vs. 11.2% (n = 1,552) for a 2.7% absolute increased risk of surgical site infection (odds ratio [OR] 1.23; 95% confidence interval [CI] 1.02–1.48) [6]. Restricting the analysis to iodophor-impregnated drapes still failed to show any benefit (OR 1.03; 95% CI 0.66–1.60) [6]. Use of the drapes might have provided an inappropriate level of comfort that translated into less attention to the fundamentals of surgical technique, such as ensuring hemostasis and minimizing diathermic devitalization of tissue, which appear to be associated with infection risk [7]. Alternatively, the authors proposed that the most obvious explanation for their observations is that adequate disinfection prior to surgery renders the skin an unlikely primary source of SSI. Thus, attempts to isolate the skin from the deeper aspects of the wound using an adhesive drape may be pointless and even harmful, as excessive moisture under plastic drapes may encourage bacteria residing in hair follicles to migrate to the surface and multiply [6]. Although the studies were not performed in the context of the placement of mesh, these data are relatively robust and convincing that adherent drapes do not reduce the risk of infection.
Antibiotic prophylaxis
Antibiotic prophylaxis for low-risk procedures such as mesh herniorrhaphy continues to be an area of debate. In part, this stems from difficulty in identifying a statistically significant difference in an outcome that is infrequent and requires a sufficiently long duration of observation to detect. In the meta-analysis of Sanchez-Manuel et al., 12 trials were included, which were of reasonably good quality [2]. There was variability in the definitions of infection (e.g., requirement for a positive site culture) and duration of followup (range one month–two years). Most surgeons utilized β-lactam antibiotics, typically administered parenterally (n = 7). There was little heterogeneity among the trials, and hence, a pooled estimate was considered appropriate. For the entire cohort, the preoperative administration of antibiotics was associated with an absolute 1.5 percentage point reduction (1.4% vs. 2.9%) in the risk of SSI (OR 0.64; 95% CI 0.48–0.85) [2]. When restricted to abdominal wall mesh herniorrhaphy, the evidence supporting preoperative antibiotics was even more compelling: OR 0.48 (95% CI 0.27–0.85) [2]. Other systematic reviews specific to antibiotics in the context of mesh herniorrhaphy call these results into question; however, these studies were less powered, demonstrating similar point estimates although with wider confidence intervals [3]. Antibiotics must be administered within 30 min prior to operative incision [8].
Antibiotic irrigation
Many surgeons derive satisfaction from irrigating wounds with a variety of antibiotic and antiseptic formulations. Although theoretically sensible, there are few data in general, let alone in the context of herniorrhaphy, to inform one's practice. Literature from spine surgery suggests that irrigating the wound with dilute povidone-iodine solution vs. saline may afford some protection, as shown in the randomized trial conducted by Cheng et al., which enrolled 414 patients [9]. After a mean followup of 15.5 mos, those investigators observed a significant reduction in early (5–30 days) postoperative SSI (0 vs. 3.4% [n = 7]; p = 0.007) [9]. More robust evidence comes from meta-analyses conducted in general surgical cases. In the Cochrane meta-analysis of SSI after appendectomy conducted by Andersen et al., a benefit from antibiotic irrigation was observed only in high-risk cases, including abscess or perforation [10]. Surgical site infection in this context was reduced by 57% (OR 0.43; 95% CI 0.18–1.01), although this situation is difficult to generalize to the clean case of mesh hernia repair. In cases of simple appendicitis, there was non-significant increase in SSI (OR 1.30; 95% CI 0.64–2.30) [10]. Literature from obstetric and gynecologic surgery similarly supports the view that in low-risk cases, irrigation with antibiotic is of little benefit [11–13]. Hence, although probably not harmful, antibiotic irrigation likely is merely a superfluous expense providing little benefit.
Choice of mesh
Contemporary data demonstrate convincingly that for groin hernia, open mesh repair (i.e., Lichtenstein, Stoppa, plug and patch) yields a marked (nearly 75%) reduction in recurrence (OR 0.26; 95% CI 0.17–0.38) compared with non-mesh repairs (i.e., Bassini, McVay, Shouldice), with no potential increase in SSI (OR 1.24; 95% CI 0.84, 1.84) [18]. As mesh repair is the predominant technique of herniorrhaphy, attention has shifted to identifying the “ideal” mesh: One that best minimizes the rates of both recurrence and infection. Earlier studies suggested that monofilament prosthetics shelter fewer bacteria, and there now are reasonably good data to support the use of monofilament mesh [14]. Coating mesh with antimicrobial agents such as metal ions (e.g., silver) may provide clinical benefit, although determining their efficacy and effectiveness awaits the rigors of additional clinical trials [15–17]. At present, there are no data from well-controlled clinical trials to support a specific mesh or component as superior in the primary repair of hernias.
In the setting of incisional hernia, however, there are additional choices that may provide an equally durable repair and carry the added benefit of a reduced risk of infection. A recent meta-analysis of laparoscopic vs. open incisional herniorrhaphy incorporated five trials, with a total of 366 patients [19–22]. The investigators looked at a composite incisional complication score and did observe a benefit in favor of laparoscopic mesh herniorrhaphy (OR 0.49; 95% CI 0.33–0.73) [19]. Focused assessment of infections suggests that laparoscopic repair may be of benefit. The data would seem applicable to inguinal herniorrhaphy as well.
Similarly, there are reasonably good data in the context of large incisional/ventral hernias that repair by component separation is of benefit. The randomized controlled trial of de Vries Reilingh et al. [23, 25], the only trial in a recent meta-analysis of open herniorrhaphy [23–25], randomized 37 patients to either mesh (n = 18) or component separation (n = 19). The mean size of these defects was large, being 400 cm2. Although there was no observed difference in the rates of recurrence—11% vs. 10% (OR 0.96, 95% CI 0.55, 1.69)—or time to recurrence (p = 0.59) for a 36-month followup period, the authors did note a difference in the rates of SSI and reoperation for incision complications in favor of component separation: 7% vs. 2% (p = 0.05; OR 0.30; 95% CI 0.07–1.26)[23, 24].
Diagnosis
Clinical
In most circumstances, the diagnosis of infection with in situ mesh is obvious. Systemic signs of infection such as fever, malaise, and chills may or may not be present, particularly in the young otherwise-healthy patient. However, local acute inflammatory signs typically are present, including pain, erythema, tenderness, swelling, and local warmth, the classic “rubor et tumor cum et dolore” described by Celsius in 1 AD [26]. In the context of these findings, it is imperative to distinguish between superficial and deep prosthetic infections, as the treatment, vis-à-vis the need for operative intervention differs, with deep infections being considerably more challenging.
Imaging
Both ultrasonography and computed tomography (CT) are of immense utility in determining the presence and extent of infection and are able to differentiate the type of mesh (polypropylene [PPE] vs. expanded polytetrafluoroethylene [ePTFE]). Newer modalities, such as ciné magnetic resonance imaging (MRI) may provide higher resolution and additional information that facilitates care.
Ultrasonography
Ultrasonography, beyond its known value in monitoring recurrences, is sensitive to the diagnosis and characterization of periprosthetic fluid collections [27, 28]. The thick echogenic line of PPE is distinguished easily from the thinner, less echogenic ePTFE [28]. Its accuracy in identifying perigraft infections has been quantified by Crespi et al., who evaluated prospectively the sensitivity of ultrasonography in 31 herniorrhaphies performed laparoscopically (n = 17) or open (n = 14) with PPE mesh [29]. High-resolution 7.5- to 10-MHz linear transducers and 3.5-MHz convex probes were utilized. Those investigators identified four seromas, two abscesses, and two occurrences of misfolding, which were all confirmed with CT. The investigators concluded that ultrasonography provides a rapid and sensitive means to evaluate mesh herniorrhaphy complications with accuracy approaching that of CT [29]. Other studies confirm the utility of ultrasonography [27]. Additional advantages include the absence of radiation; the dynamic images that enable real-time characterization of the anatomy; and the opportunity for guided fluid sampling or drainage. Additional, theoretical utility may come in the ability to enhance bacterial isolation, a modality being utilized in orthopedic prosthesis infections [30].
Computed tomography
Computed tomography scanning is the gold standard for evaluation of mesh and surrounding structures/viscera. Both PPE and ePTFE can be visualized and characterized on the basis of their different composition and thickness [28, 31]. The thinness of PPE, although a distinguishing characteristic, renders it more difficult to discern, being appreciable in only 20% of cases in one study [28]. By contrast, ePTFE mesh is seen universally [28, 32]. Although similar to ultrasonography in identifying fluid collections, CT with intravenous contrast medium provides the additional benefit of indirect evidence of physiology (i.e., inflammatory rim enhancement). Computed tomography proved to be of greater utility in characterizing larger regions of interest, such as in the setting of incisional hernias. In these circumstances, the necessary information regarding surrounding viscera is provided by CT.
Magnetic resonance imaging
Functional ciné MRI is beneficial in diagnosing complications of implanted synthetic mesh after hernia repair. This modality eliminates radiation exposure and provides exceptional resolution. Fischer et al. utilized a 1.5T system to assess the benefit of functional MRI [33]. Twenty patients presented with intra-abdominal adhesions, with nine exhibiting adhesions in more than one location. Of note, PPE mesh could not be seen, whereas all ePTFE meshes were visible. Dynamic MRI also has excellent resolution, not only of periprosthetic collections, but also of adhesions and intestinal communications (e.g., fistula) as well [34]. This newer modality may prove to be of benefit in the complicated, high-risk patient for whom a true appreciation of the underlying anatomy and pathology would greatly facilitate the operative approach.
Treatment
Infected prosthetic material usually requires operative intervention. Although not ideal, removal of the mesh when recurrence is expected is preferable to attempting to treat an advanced mesh infection medically. Although historically it was taught that substantial differences exist in the treatment of specific prosthetic infections, with PPE, in contrast to ePTFE, being more amenable to in situ treatment, the data suggest that either mesh may be salvaged.
Antibiotics
Initial therapy requires the institution of empiric antibiotics, which are later tailored to the subsequent speciation and sensitivity analysis of the offending organisms. Staphylococcus aureus is by far the most common bacterium isolated, with an increasing proportion being methicillin resistant (MRSA). In a recent study, 63% of staphylococcal species isolated were MRSA [35]. Less common organisms are Streptococcus spp., Enterobacteriaceae, and anaerobic bacteria. Hence, initial antimicrobial therapy is combinatorial, including vancomycin in conjunction with an antibiotic with both gram-negative and anaerobic coverage. The presence of anaerobic organisms should raise concern about enteric communication or contamination and prompt additional imaging to delineate the potential source. Under such circumstances, attempts to salvage the mesh are likely to fail.
Salvage
The dilemma encountered universally is whether the mesh can be salvaged. Both the state of the patient and the site of infection will inform the decision. For the patient who is critically ill at presentation, with evidence of compromised physiology, there is little time for observation, and urgent operative exploration and removal of the offending infectious focus is essential. Similarly, ultrasonography or CT evidence of extensive, suppurative fluid collections renders salvage attemps imprudent, only contributing to delayed definitive therapy. However, in the context of superficial infection, wherein the deeper layers incorporating the mesh are considered spared or only partially involved, an attempt at salvage may be pursued. This would include an initial period of antibiotic therapy followed by superficial opening of the wound should such therapy prove insufficient (Fig. 1).
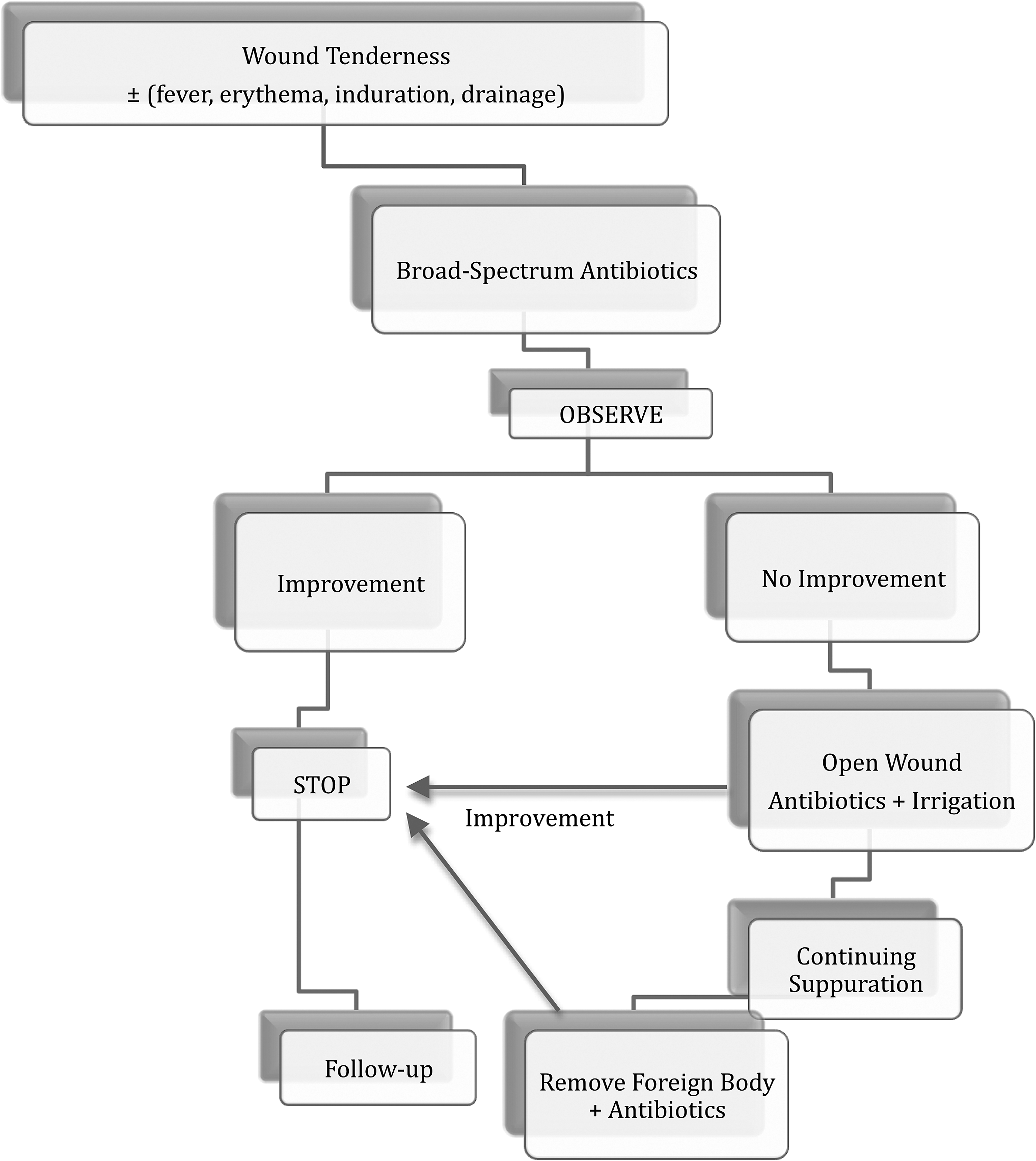
Management of infection with in situ mesh (Redrawn from Deysine, M., Pathophysiology, prevention and management of prosthetic infections in hernia surgery. Surg Clin North Am 1998; 78:1105–15)
Deeper infections that incorporate the mesh pose a larger challenge. The literature is replete with case reports and observational trials of successful salvage of almost every type of mesh in the setting of infection. Hence, these data do not lend themselves to any evidence-based algorithmic approach, although dispelled anecdotal tenets that the mesh itself (i.e., PPE vs. ePTFE) dictates a particular approach.
Recent studies have indicated that infections involving ePTFE mesh may not necessitate surgical excision as the only recourse. Paton et al. studied 22 patients presenting with documented ePTFE infections a mean of 70 days (range 10–148 days) after placement [36]. Although 14 patients with extensive involvement required excision, the authors were able to salvage seven of the eight grafts with limited involvement. Management consisted of either partial excision and vacuum-assisted closure or percutaneous drainage of perigraft fluid collections in combination with four weeks of antibiotics. Similar success was observed in two patients in whom infected ePTFE was managed by percutaneous drainage, gentamicin irrigation, and parenteral antibiotics. At 12 and 16 mos of follow-up, both infections had resolved with retention of the mesh [37]. These data support the idea that extensive ePTFE mesh infections are best managed by expeditious excision. However, mesh with less progressive infections may be salvageable, albeit with considerable effort.
Similar data exist for PPE. Petersen et al. studied 121 incisional herniorrhaphies: PPE (n = 77), polyester (n = 7), and ePTFE (n = 37) [38]. The mean time to infection was 4.5 mos (range, 0.5–16 mos). All three infected ePTFE patches required removal, whereas drainage was sufficient for the infected PPE and polyester meshes. By contrast, in a study of 423 meshes implanted for groin, femoral, umbilical, and incisional hernias with a mean follow-up of 15 mos (range, 3–73 mos), there were five prosthetic mesh infections, all of which necessitated removal [39]. Collectively, these data support the conclusion that appropriate patient selection, guided by clinical assessment and ancillary imaging to determine the nature and extent of mesh involvement, may afford salvage in some cases.
Vacuum Assisted Closure® (VAC; Kinetic Concepts, Inc., San Antonio, TX) has proved beneficial in salvaging both PPE and ePTFE mesh, although most studies to date were retrospective and incorporated small cohorts. In a study by Tamhankar et al., four patients underwent VAC for treatment of infected mesh, all using an onlay of PPE mesh [40]. Continuous negative pressure was applied to the wound utilizing the polyurethane dressing for a mean of 4.7 weeks. The VAC initiated closure in all four patients and stimulated granulation on the mesh surface. In a case study by Kercher et al., a Dual Mesh™ (W.L. Gore and Associates) infection was treated with VAC in a 37-year-old woman with multiple co-morbidities [41]. Four months after her ventral hernia repair, the patient returned with exposed mesh, from which cultures isolated MRSA. Progressive debridement, with partial mesh excision, surgical closure, and re-approximation with PPE sutures salvaged the mesh with no evidence of infection at 18 mos of followup. These data, although uncontrolled and from small cohort analyses, dispel prior tenets that infected mesh, particularly ePTFE, requires excision. Furthermore, they support a trial of salvage for the non-toxic patient with localized infection (Fig. 1).
Excision and repair
Despite the success described for salvage techniques, the majority of deep mesh infections will necessitate excision. In the setting of ePTFE, excision is facilitated by the absence of mesh incorporation. Excision of PPE can be more challenging because of adhesive cicatrix formation. Although complete excision is preferable, a balance must be maintained between the risks of relentless pursuit it and iatrogenic injury. This cautionary note is particularly salient in incisional herniorrhaphies, where dense adhesions to the bowel may yield enterotomies and enterocutaneous fistulae, which are far more jeopardizing to the patient than a small retained piece of infected mesh.
Once the mesh is excised, a decision is made as to the means of repair. Inguinal hernias may be managed by primary repair (i.e., McVay, Shouldice, Bassini) and achieve reasonable closure, albeit at a higher risk of recurrence. This is attributable to both the tension-producing properties of these repairs as well as the fact that they are performed in the context of infection. A number of biological implants (e.g., Alloderm®, LifeCell, Branchburg, NJ, Surgisis® Cook, Bloomington, IN, Permacol™ LifeCell) have been developed with the purported ability to achieve a secure, durable closure in the context of contamination. Franklin et al. recently presented data on the placement of porcine small intestinal submucosa mesh (Surgisis) in 116 patients with potentially or grossly contaminated fields [42]. All procedures were performed laparoscopically. With 85% five-year follow-up (mean 52 ± 21 mos), the investigators observed seven recurrences and 11 seromas, thus concluding that placement of a bioprosthesis is a safe and feasible alternative to hernia repair [42]. Similar observations have been made in earlier, smaller studies, with a cautionary note that early graft failure may occur by overwhelming fascial infection and limit use [43, 44]. Similarly, small (<2 cm) umbilical and incisional hernias may be closed primarily with non-absorbable suture. Larger defects carry a higher risk of recurrence because of tension. This may be addressed to a degree using a biological mesh over- or underlay to distribute the tension evenly away from the primary repair or component separation.
Large incisional hernias create a particularly challenging situation. This stems from the large domain that must be addressed, as well as the fact that many of these patients present with considerable co-morbidities and physiological compromise. After mesh removal, one must consider whether repair can be undertake. In the setting of any physiologic compromise, it is prudent to postpone such measures and wait for a time when both patient and operative site are better. Primary repair typically is not feasible, particularly without tension; recurrence is all but guaranteed, with a rate of 12%–54% [45, 46]. Prosthetic mesh reduces the recurrence rate to 2%–24%; however, placement of permanent mesh in heavily contaminated fields carries infection rates as high as 50%–90% [47, 48]. Hence, under these circumstances, we propose a skin-only closure with large non-absorbable suture (i.e., No. 1 PPE). This technique provides a biological dressing to the underlying viscera, although granted, it does little to maintain the domain. At a later date, the patient is assessed for a component separation procedure.
Component separation
Component separation (i.e., separation of parts) involves the mobilization of components of the abdominal wall to achieve a tension-free repair using autogenous tissue. Classically, incision of the external abdominal oblique muscle lateral to the rectus abdominis aponeurosis and its separation from the underlying internal abdominal oblique muscle provide additional mobilization to enable primary midline closure of the linea alba [23, 25, 49]. A variety of techniques have been described to which the reader is referred [23, 25, 49–52]. The procedure carries the obvious advantage of avoiding prosthetic mesh or biological implants in a contaminated field; there also are data suggesting reasonable long-term success. In one study, 11 patients with ventral mesh herniorrhaphy in which the mesh was exposed, infected, non-incorporated, or associated with enterocutaneous fistula were managed by mesh removal and component separation [49]. The mean transverse dimension of the defect was 13 cm (range, 8–18 cm). After a followup of 24 mos (range 5–54 mos), there was one recurrence and two stitch abscesses. The recurrence was treated with exploration and primary repair, and after a further two-year period of observation, there was no clinical recurrence. Other investigators have reported slightly higher recurrence rates. de Vries Reilingh et al. observed a 32% recurrence rate for component separation without reinforcement in 43 patients with complex abdominal wall defects [25]. Notably, 15 of these patients had grossly contaminated sites, making this a high-risk population. Other authors utilizing component separation with reasonable follow-up (>12 mos) report favorable recurrence rates of 0–9% [53–56].
Biological implants
A variety of biological implants have become available with the purported properties of achieving a secure, durable closure in the context of contamination. Although short-term success is supported by the literature, considerable question persists as to their long-term durability. In a study of nine patients, three of whom had mesh excision because of infection, Parker et al. utilized a porcine acellular dermis (PermacolTM Covidien, Mannsfield, MA) underlay ensuring a 3-cm overlap using non-absorbable suture [57]. After a mean follow-up of 18.2 months, there was one recurrent hernia in the setting of a postoperative perigraft abscess that necessitated intentional graft removal. Of note, five patients had class II, III, or IV infection yet sustained no postoperative infectious complications. The authors concluded that porcine acellular dermis is a safe and acceptable alternative to prosthetic mesh in the repair of complicated abdominal wall defects.
A recent study followed 11 patients who underwent complex ventral herniorrhaphy with bridging acellular dermal matrix (ADM, Alloderm) in the context of infected mesh (n = 2), bowel resection (n = 4), enterocutaneous fistula (n = 2), or high risk for infection (n = 3) [58]. The details of herniorrhaphy were not provided. After a mean follow-up of 24 mos (range, 18–37 mos), eight recurrences were observed, of which seven patients underwent repeat herniorrhaphy. This high recurrence rate is in stark contrast to several earlier studies that reported much more favorable outcomes. Diaz et al. reported a recurrence rate of 16% in their series of 75 patients using ADM; however, the follow-up period was only nine mos [59]. Blatnik et al. noted that had their follow-up only been nine mos, they would have reported a recurrence rate of only 20% [58]. These studies highlight the importance of sufficiently long follow-up to assess the long-term durability of these repairs accurately.
Kolker et al. reported their experience with ADM using a sandwich technique in 16 patients [60]. After a mean follow-up of 16 mo, they observed no recurrences. Schuster et al. tried recently to identify factors that might predict recurrence with ADM [61]. They found the following factors: Use as a bridge (recurrence rate 50%) and inability to achieve skin closure. Interestingly, the number of sheets of ADM used did not affect the success rate, but this might stem from the nearly universal recurrence.
Conclusion
Mesh herniorrhaphy is the standardized approach for repair of abdominal wall defects. The experienced surgeon, despite adhering to all preventive measures to minimize infection, will still be challenged with abdominal wall infections with in situ mesh. Although an ideal algorithm for the treatment of mesh-related infections will continue to mature with the acquisition of evidence from clinical trials, Figure 1 will, it is hoped, provide some beneficial insight and guidance for the management of this complication.
Footnotes
Author Disclosure Statement
No conflicting financial interests exist.
Presented at the 29th Annual Meeting of the Surgical Infection Society, Chicago, Illinois, May 6–9, 2009.